
Figure 1.
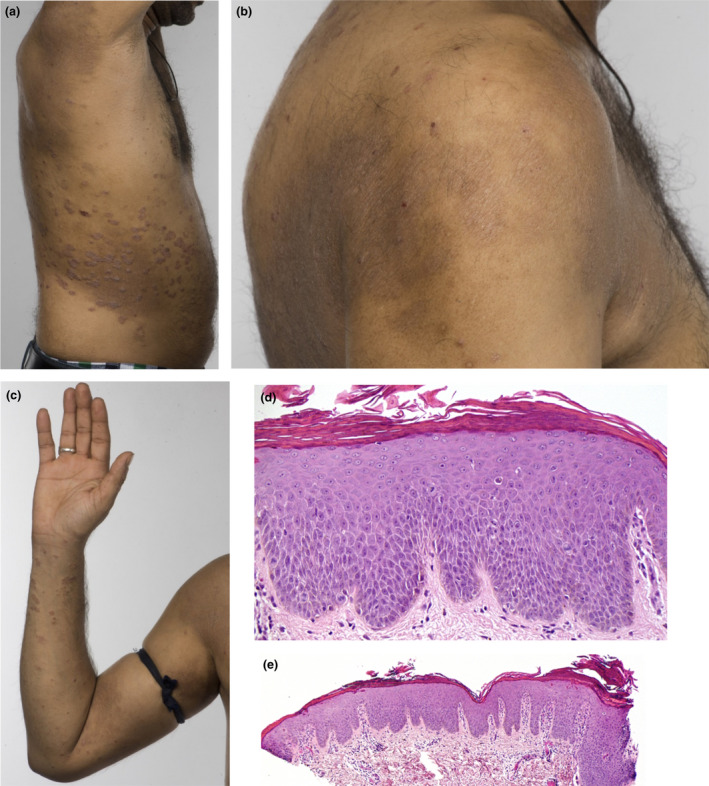
(a–e) Patient 4, a 34‐year‐old man with a 13‐year history of psoriasis, previously treated with ciclosporin, methotrexate and adalimumab, presented with flexural and periorbital eczema 81 days after starting ustekinumab. The eczema gradually resolved on stopping ustekinumab, although his psoriasis flared severely, reaching a Psoriasis Area Severity Index of 34.9. Infliximab resulted in a recurrence of paradoxical eczema (PE) 13 days after initiation, which persisted for > 2 years despite infliximab being stopped and treatment with ciclosporin and methotrexate initiated. Apremilast controlled the psoriasis, but not the PE. The patient was then started on secukinumab, resulting in recurrence of PE after 55 days, which persisted despite secukinumab being stopped and treatment with ciclosporin started. Tofacitinib, a Janus kinase inhibitor, also improved the PE but not the psoriasis. Finally, the patient was started on guselkumab while ciclosporin was continued, but the PE has persisted. (a‐c) Well‐defined, indurated plaques on the flanks and arms consistent with psoriasis, with coexisting eczema and lichenification affecting the shoulders and antecubital fossae, 18 months after stopping secukinumab. (d,e) Skin biopsy from the back showing (d) spongiosis and (e) psoriasiform hyperplasia. Haematoxylin and eosin, original magnification (d) × 200; (e) × 40. [Colour figure can be viewed at wileyonlinelibrary.com]