
Figure 3.
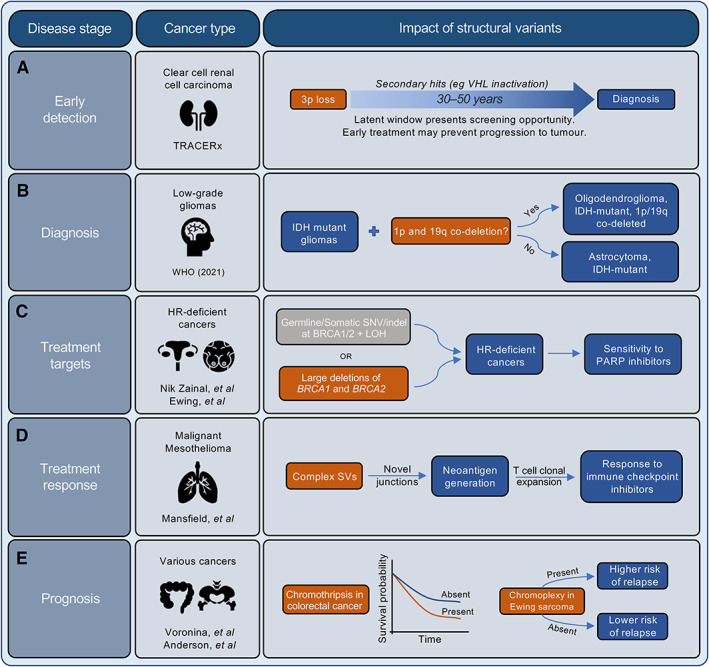
The clinical importance of structural variants (SVs) across all stages of the patient journey. SVs have significant potential in influencing the management of cancer patients throughout the disease trajectory. Some examples of the potential impact of SVs include: (A) Early detection: the TRACERx study on clear cell renal cell carcinoma [160] identified that 3p loss was frequently generated via chromothripsis, and that the loss could occur decades before diagnosis, suggesting the opportunity for early detection and intervention. (B) Diagnosis: the stratification of low‐grade gliomas (isocitrate dehydrogenase [IDH] mutant gliomas) has recently been updated by the WHO to include those with or without concurrent 1p and 19q co‐deletion [161]. (C) Treatment targets: tumours with large deletions of both BRCA1 and BRCA2 loci form a subset of HR‐deficient tumours that are exquisitely sensitive to PARP inhibitors [154, 155, 162]. (D) Treatment response: Mansfield et al [157, 158] demonstrated that malignant mesothelioma harbours neoantigens that are generated by complex SVs, and that their generation was associated with the clonal expansion of T cells, indicating that complex SV burden can be used to predict response to immune checkpoint inhibitors. (E) Prognosis: the presence of complex SVs are associated with poor prognosis. For example, patients with chromothripsis‐harbouring colorectal tumours have poorer survival rates compared to those without chromothripsis [163], and patients with Ewing sarcoma that contain chromoplexy have a higher risk of relapse following first‐line therapy [112].