

Abstract
Introduction
Clinical indications on how to approach caregiving with a person living with dementia underline the need “to have an empathic attitude” requiring the caregiver to view the world from the perspective of the person with dementia. However, it is not easy for the caregiver to understand the perspective their patients have on day‐to‐day experiences. To put the caregivers in the person with dementia's shoes, the Virtual Dementia Tour (VDT) was developed in 2001, and has been administered to millions of health professionals, community leaders, and family caregivers.
Method
In this paper we present the Italian version of the VDT and discuss its internal validity and test–retest reliability for the pre–post experience survey defined by the VDT procedure.
Results
An Italian sample (N = 419; mean age = 44.8; standard deviation 14.2) completed the tour and a 5‐item survey provided before and after the experience revealed the disposition toward people with dementia changed.
Discussion
The VDT Italian version wasrevealed to be valid in supporting a positive perspective change in the perception of dementia as is seen in the original VDT used in English‐speaking countries.
Highlights
Empathy predicts a higher quality of caregiving for the person living with dementia.
The Virtual Dementia Tour (VDT) provides an experience from the person living with dementia's perspective and supports empathy.
We present the first Italian version of VDT and its manual translation and validation.
Italian VDT internal consistency and test–retest reliability were calculated.
Results confirms the reliability and validity of the Italian VDT for empathy.
Keywords: caregiver stress, dementia care, empathy, first‐person experience, simulation training, Virtual Dementia Tour
1. INTRODUCTION
In recent years, different dementia care strategies have been implemented worldwide after the publication of the “Global action plan on the public health response to dementia 2017–2025” at the 70th World Health Organization Assembly in May 2017.
Currently, dementia care focuses on non‐pharmacological strategies, intended as formalized and replicable interventions potentially capable of providing clinical benefits. These practices have proven to be particularly effective in stimulating and activating the cognitive–emotional–social functions that can provide high‐quality dementia care during disease progression. 1 These models as a whole are characterized by the active involvement of the person 2 considering their bio‐psychosocial complexity and are now widely proposed to mitigate the impact of the disease, reduce the disability deriving from neuropsychological decline, and support emotional‐relational abilities mainly expressed in the caregiver–person with dementia relationship. Accordingly, to increase professional competency in dementia care an empathy‐based model is always requested as a starting point for the treatment of dementia.
Empathy is a complex bio‐psychosocial concept, distinguished in two main constituents: the cognitive subcomponent, associated with functioning of the medial and dorsolateral regions of the prefrontal cortex, which impacts understanding of what another person is feeling on the basis of another persons’ perspective; 3 the emotional subcomponent, associated with activation of both subcortical and cortical structures, grounds the ability to attune with what another person feels. 4
Research shows how empathic care supports better clinical outcomes and decreased anxiety in general clinician–patient relationships, 5 but also how empathy assumes a central role in predicting a higher quality of caregiving for the person living with dementia. 6 Accordingly, it is urgent to develop educational interventions focused on heightening the caregiver's empathy, to introduce the highest quality of care for the person with dementia 7 , 8 and to reduce caregiver burden. 9
To achieve an empathetic perspective, it is necessary to detect and appraise the cognitive representations and emotions of the individual. The experiential approach to dementia care training forces this perspective to change understanding through providing the opportunity to view a person with dementia's perspective. When caregivers recognize dementia behavioral symptoms are part of the disease instead of intentional acts, the ability to understand the person with dementia increases. This profoundly changes the caregiving relationship, turning it into a more accepting, inclusive, and satisfactory one. 10
It is for this reason that the Virtual Dementia Tour (VDT) was developed in the United States. 11 The main aim of the VDT is to provide caregivers the opportunity to personally experience life from the perspective of the dementia population. The VDT working hypothesis states that when caregivers personally experience the limitations of dementia, they will be able to develop increased sensitivity to the needs of persons with dementia. To date, the VDT has been implemented in over 2000 healthcare organizations, distributed in 20 different countries, and conducted with over 3 million people. Research has shown the VDT increases the provision of empathic person‐centered care. 12
This paper aims to evaluate if the Virtual Dementia Tour can be used to increase awareness of the impact of dementia on everyday life in the Italian population. We present the Italian version of VDT in this paper, including the VDT manual translation process. As in the VDT procedure before and after the experience a survey is proposed to detect the effectiveness of the intervention by measuring the change in people's disposition to dementia, internal consistency analysis, reliability, and pre–post validity evaluation of the survey was conducted.
RESEARCH IN CONTEXT
Systematic Review: The authors reviewed the scientific literature using traditional sources (e.g., PubMed), as well as analyzing abstracts and presentations at international conferences. There are numerous recent publications that describe burnout in the caregiving professions for people with dementia, and they are appropriately cited. At the same time, few studies analyze how to support the caregiving relationship to avoid burnout.
Interpretation: Our results have helped to expand the data already collected worldwide about the effectiveness of the Virtual Dementia Tour to the Italian language culture. The results achieved are consistent with the results derived from previous studies currently in the public domain.
Future Directions: The article proposes a validation of the tool for its correct clinical use in Italian speakers and for the conduct of further studies in this cultural field. The methodological development of the Virtual Dementia Tour in Italian will allow the implementation of specific psycho‐educational interventions in the urban community (e.g., schools, neighborhoods, and nursing homes) to support formal or informal caregivers in their role of supporting people with dementia and improve the quality of their life.
2. MATERIALS AND METHOD
2.1. Participants
This study involving human participants was reviewed and approved by The University of Bergamo ethic committee according to the Declaration of Helsinki. Written informed consent to participate in this study and for the publication of any potentially identifiable images or data included in this article was provided by the participants.
The study voluntarily enrolled 419 Italian participants (328 females; 91 males) from 16 to 82 years old (mean age 45.75, standard deviation 14.95). They had different school levels (45.8% university; 37.4% high school; 16.5% secondary school; 0.5% primary school) and professional backgrounds (51.9% health; 7.2% education; 40.9 other).
Participants were asked to answer a 5‐question pre‐ and post‐survey (see Appendix S1 in supporting information) to record their experiences with the VDT. After the experience, a debrief meeting was also conducted.
2.2. Virtual Dementia Tour
The VDT is a dementia experiential training program developed by P. K. Beville 11 and widely used worldwide in dementia care education. VDT experience development was derived from neuroimaging research that evidenced the impact of brain neurodegeneration on sensory, cognitive, and praxis impairment generally observable in people living with dementia.
The VDT is composed of a timed experience in which participants were asked to wear items designed to simulate:
Pain that frequently accompanies neuropathy
Loss of sensory and fine hand motor skills
A variety of visual impairments
Confusion through audio stimulation
During the experience in which several time‐pressure tasks were provided to the participant, a trained observer marks behavior frequently exhibited by people with dementia (such as negative statements, whispering to self, requests for help, agitation, shadowing, wandering, hoarding, rummaging, repetitive behaviors, etc.).
2.3. Italian VDT translation process
The VDT procedure is described in a manual explaining to professionals how to provide the experience. To avoid loss of literal word meaning in the VDT manual for the Italian‐speaking population, translation and cross‐cultural adaptation of the VDT procedure from the US manual into Italian was performed consistently with the stages recommended by Beaton et al. 13
The translation process followed these steps:
Starting from the original US version, three independent native Italian‐language speakers (who have strong US English language skills) translated the manual.
Next, a comparison between the three Italian manual translations (1–2, 1–3, 2–3) was run.
The significant differences among the three translations were highlighted to identify whether the translators faithfully captured the meaning.
A panel composed of the three translators, two VDT experts, and two experts in dementia who do not participate in the VDT, was constituted to discuss the Italian–English disputed translations.
The final version of the Italian VDT manual was agreed upon.
The translation derived from the panel agreement is the one used for the validation of the VDT in the Italian population.
2.4. Procedure
Participants gave consent to participate in the VDT experience and a random number was assigned to each to anonymously record their participation data.
The participant then completed a pre‐experience survey, and to ensure uniformity of stated purpose and expectations, they were provided with a written instruction sheet containing ground rules for the VDT experience. After this step, each participant was individually led into a “preparation room,” where they were asked to wear patented VDT devices (garbing). Next, they were escorted to the VDT experience room. At the end of the experience the participant was taken to a debriefing room to remove the devices and to answer the post‐experience survey. Two certified trainers supervised the tour.
Finally, a group debriefing was conducted to allow discussion about participants’ experience during the VDT and to provide examples of how caregivers can help the person with dementia. This time is specifically designed for outlining empathic person‐centered care learning objectives and goals.
3. RESULTS
3.1. Manual translation
No major discrepancies were evidenced regarding forward (English to Italian) translation procedures. Slight cultural adaptation was necessary and agreed upon among the different translators. No substantial issues arose because the procedure part of VDT manual does not include any elements that could vary significantly among different cultures and lifestyles (personal care, daily activity, etc.). Slight differences were encountered though in the pre‐ and post‐experience survey translations. The decision on what could have been considered the most significant modification led to minor deviation from the original VDT survey version and the panel agreed to translate literally from the US version. None of the participants revealed any doubts about the VDT procedure and in answering the pre–post experience survey.
3.2. Data analysis
Analysis of the Italian VDT was structured in four steps and was conducted using Jamovi software, version 1.0.8.0. 14
First, we calculated means, standard deviations, scale internal consistency coefficients (Cronbach's α), and VDT pre‐experience survey item total correlations.
Second, a principal component analysis (Promax rotation) was conducted to assess VDT pre‐experience survey construct validity. For this study, the item fit with five variables from VDT pre‐experience survey was tested.
Then, a confirmatory factor analysis (CFA) was conducted to test the interrelationships among survey items, and to determine whether a set of items share common characteristics that define the construct. We evaluated the CFA model using four common fit indices: comparative fit index (CFI; recommended values ≥95), the Tucker‐Lewis index (TLI; ≥95), standardized root mean squared residual (SRMR) index (recommended values between 0 and 0.08), and root ‐mean square error of approximation (RMSEA, < .06).
At last, a pairwise Student's T analysis on (T0) pre‐ and (T1) post‐ surveys was conducted to compare participants’ answers provided before and after the VDT experience.
3.3. VDT survey internal consistency
To explore the Italian VDT survey internal consistency, answers collected in the before experience (pre‐VDT) were first analyzed using the Cronbach's α value. The correlation among questions loaded onto the same factor does not reveal a consistent value (α 0.25).
Thus, for underlying the different components addressed by the VDT survey, a principal component (PCA) analysis was conducted. Promax rotation revealed two grouping factors loading: Factor 1 (emotion) includes Q1 (0.721) and Q3 (0.695); Factor 2 (autonomy) includes Q4 (0.791) and Q5 (0.750). Q2 was also separately analyzed even if it does not adequately load onto the factor. Relation among factors is depicted in Figure 1.
FIGURE 1.

Path diagram picturing relations among the five items of the pre‐Virtual Dementia Tour experience survey
The CFA values for the specific indices indicated an adequate fit between the model and the data: CFI = 1.00, TLI = 1.10, SRMR = 0.012, and RMSEA = 0.00. All the values are within conventional standards for a good fit and this provides compelling evidence of a convergent validity on VDT constructs.
3.4. VDT survey reliability
Considering data obtained from a Likert scale, the test–retest reliability of the VDT surveys was calculated by correlating (Spearman's ρ) the respective answers provided for each inventory pre‐ and post‐VDT experience. Statistically significant strong positive correlations between pre‐ and post‐VDT surveys were observed for all the items (Q1—emotion understanding ρ = .139, P = .004; Q2 efficiency and executive functioning in simple tasks ρ = .129, P = .008; Q3 relaxation ρ = .130, P = .008; Q4 empathy and daily behaviors easiness ρ = .130, P < .001; Q5 adequate caregiving ρ = .196, P < .001) suggesting the VDT survey has a good test–retest reliability.
Correlation table and plots are depicted in Figure 2.
FIGURE 2.
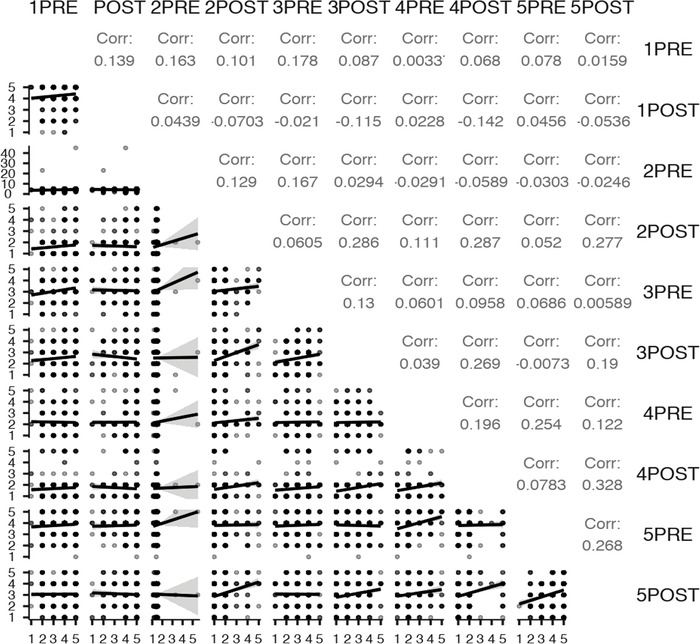
Virtual Dementia Tour pre‐ and post‐experience correlations (Spearman's ρ)
3.5. Pre—post VDT experience changes
A comparison between participants’ answers provided before and after the VDT experience was run using a pairwise Student's T analysis on pre‐ (T0) and post‐ (T1) VDT surveys. Detailed results (with mean and standard deviation data, statistical significance, and effect size) are depicted in Table 1 and Figure 3.
TABLE 1.
Comparisons between pre‐ (T0) and post‐ (T1) VDT survey answers. Means (standard deviations), statistical significance, and power
| T0 Pre‐VDT Mean (SD) | |||
|---|---|---|---|
| Item | T1 Post‐VDT Mean (SD) | Student's T P value | Cohen's d |
| Q1 Emotion understanding | 3.53 (1.04) | (–11.59) <.001 | −0.56 |
| 4.27 (0.91) | |||
| Q2 Efficiency in simple tasks | 4.12 (2.40) | (20.19) <.001 | 0.99 |
| 1.64 (0.88) | |||
| Q3 Relaxation | 3.11 (0.93) | (9.36) <.001 | 0.46 |
| 2.50 (1.09) | |||
| Q4 Daily behaviors easiness | 2.19 (0.75) | (9.28) <.001 | 0.45 |
| 1.69 (0.89) | |||
| Q5 Adequate caregiving | 3.80 (0.86) | (12.82) <.001 | 0.62 |
| 3.07 (1.03) |
Abbreviations: SD, standard deviation; VDT, Virtual Dementia Tour.
FIGURE 3.
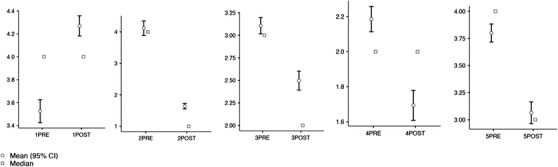
Plots depicting the modification pre‐ and post‐ Virtual Dementia Tour experience for each of the five questions proposed
4. DISCUSSION
4.1. VDT manual translation
A primary aim of this study was to culturally adapt and translate into Italian the original version of the VDT manual. This process was successful as the manual conversion has been carried out in accordance with the Beaton et al. 13 guidelines. The seven‐person panel involved in this phase did not encounter major difficulties during the translation and cultural adaptation of the VDT manual because it did not include procedure descriptions that could be performed differently according to lifestyle options and cultural habits. The VDT Italian version also did not have difficulties in the application of the instructions provided to participants during the experience. Moreover, the validation of the survey provided to the participants before and after the VDT is the tool by which the efficacy of the experience for a perspective change is measured and it is intrinsically linked to the validation process of the entire VDT in its Italian version. Thus, after being translated into Italian the pre‐ and post‐experience survey was followed by establishing internal consistency, reliability, and construct validity according to international literature recommendations.
4.2. Internal consistency
Although the internal consistency did not reveal a significant value for all the items, the PCA showed which of the questions could be grouped to understand the structure of the pre‐ and post‐VDT experience survey. From this analysis, in fact, it appears that questions one and three can refer to a common factor that describes the emotional dimension involved in the relationship with a person living with dementia. In particular, Q1 refers to the empathic capacity of the caregiver to judge their own ability in taking the emotional point of view of the person with dementia while Q3 intends to evaluate the emotional reaction of the caregiver themselves in getting involved in a relationship with the person with dementia. Accordingly, both questions can be considered the two sides of a unique factor exploring the intersubjective emotional attunement at play 15 that are necessary for being predisposed in everyday living with a dementia person. Constructing an inclusive relationship, based on the creation of a mutual alliance that can allow the person with dementia to feel understood and welcomed in its most intimate dimension and not considered a stressful element of the relationship, is the goal. 2 , 11
Questions four and five refer specifically to the autonomy dimension and the caregiver's awareness about the difficulties encountered by the person with dementia in facing daily activities. Q4 explores the level of caregivers’ awareness in understanding how to judge the difficulties that a person with dementia could face in carrying out the activities of her/his daily life. It implies a specific knowledge of the characteristics of the disease together with an ability to judge the functional fragility that this involves. At the same time, Q5 aims to assess perceived adequacy of services to support the person with dementia. These items show the participants’ understanding of how a person with dementia faces challenges of daily life and takes into consideration what difficulties she/he may encounter in it. Being able to view care through this lens is at the seat of empathic person‐centered care. When one is not only able to take the perspective of the other but can also evaluate needs of the other when they are not able to achieve their goals requires a deep level of empathy. 16 It also requires that one knows how to evaluate what is necessary for the other to be able to maintain themselves. 17 In this perspective, autonomy is not considered only as self‐determination, but in the case of dementia, it is a conscious inclusion from caregivers and aimed at the realization of an individual and autonomous action. Question 2 does not adequately load onto a factor but explores individual awareness of being able to face daily tasks compared to capability after the VDT experience. In fact, judging how to emotionally react within a relationship with people with dementia and how to create adequate scaffolding around the person in supporting their daily autonomy, undoubtedly requires evaluating how difficult it could be to efficaciously fit with the environmental challenges according to individual skills. 18 This is the yardstick human beings use to adequately emotionally react to each other, and create space for a successful autonomous interaction. Thus, even if not confirmed from the internal consistency Cronbach's α value, the survey items appear to be groupable in two main factors (emotion and autonomy) and glued together from the awareness one has about the daily difficulties encountered by a person with dementia. All together the survey questions explore the main dimension of what it would be like to live with dementia.
4.3. Principal component analysis
Even if the Cronbach's α value for internal consistency aAnalysis did not reveal a significant value, the results obtained from the PCA might support the use of emotion/autonomy subscores instead of the use of a total score. But considering the small number of items that define the factors, as well as their intrinsic relationship revealed by the four CFA common fit indices, it was considered more useful to continue to consider the VDT pre‐ and post‐experience survey as a single survey that could return an integrated picture of the three factors at stake. Consistently, the test–retest analysis evidenced how the survey measurement variation was due to replicable differences between VDT participants regardless of time, target items, or user profile thus confirming the reliability of the entire survey in evaluating participants’ attitudes on the five items both in pre‐ and post‐ VDT experience. Construct validity of the Italian version of the VDT pre‐ and post‐experience survey showed an adequate internal reliability for the survey. The overall acceptable goodness‐of‐fit indices support the construct validity of the VDT Italian translation.
4.4. Pre‐ and post‐VDT experience survey
The data on the differences in the responses to the pre‐ and post‐experience survey items were also concordant, showing how the T0 and T1 compare as conducted for the five survey items. Results show a statistically significant change in answers provided pre‐ and post‐VDT experience.
Q1 shows a significant improvement in the understanding of the emotions felt by a person with dementia after experiencing VDT. This result is in line with one of the main objectives that the VDT experiential approach, which postulates that experiencing what dementia is like, results in great understanding, empathy, and person‐centered care. Furthermore, this increased capacity, possible through VDT experience, has been further reinforced by literature and can be considered one of the fundamental steps for achieving an empathic disposition, 4 , 16 deemed absolutely necessary for person‐centered care in dementia. Q2 analyzes the subjective estimate that everyone has in being able to complete simple everyday activity which, before the VDT experience, was judged by the participants as very high and afterward decreases in a statistically significant way. The data shows how, after having encountered numerous difficulties in completing the tasks proposed by the VDT, after the motor and sensory limitations/distortions caused by the components worn during the experience, participants have gained a greater awareness of the difficulties people with dementia face every day. Having improved awareness of the difficulty experienced by the person with dementia allows us to obtain a very important result because it is precisely these misunderstandings that can generate reactions of irritation on the part of the caregivers when people with dementia are no longer capable of managing daily life independently. These data are consistent with results from Q3 in which the feeling of being relaxed significantly decreases after the VDT experience. This suggests that when participants are faced with the simulation of dementia, they find themselves out of their comfort zone and feeling frustrated by their losses in functioning. The uncomfortable feeling allows the participants themselves to better identify with a person with dementia when they seem to understand why sometimes people with dementia overreact to their experienced inability to manage their daily lives independently. In this way, we might think that, after the VDT experience, ordinary people are more aware of what may have caused an unexpected sudden change in mood in people with dementia. This conclusion appears to be supported by the significant change in evaluating the easiness of daily living for people with dementia (Q4) that decreases after the VDT experience. Finally, data observed in Q5 shows after the VDT experience, there is increased awareness of what is needed to assist a person with dementia. Most glaringly, participants before the experience believe that people with dementia get the care they need, but after experiencing what dementia is like 63% of participants state that people with dementia do not get the care they need.
5. CONCLUSION
This study seems to have been able to provide an Italian‐language version of VDT that may be a valid tool to support empathy toward the person with dementia. By gaining the perspective of the person with dementia while involved in daily activities, the survey revealed it has allowed caregivers to better understand their difficulties, as well as the consequent emotional reaction that can emerge after an inability to cope to environmental challenges.
This research confirms the reliability and validity of the VDT in Italy. This important finding shows that responses to the assessment before and after the VDT are in concert with the responses obtained to the same questions in the United States, solidifying the results and conclusions therein.
While caregiving for those with dementia continues to increase, the characteristics of the caregivers follow the same results in both countries. Just as dementia follows a specific course, it seems the responses from VDT participants follows a specific course with statistically significant results pre‐ and post‐experience. This consistency further solidifies validity.
The provision of empathic person‐centered care allows for relationship building with the person with dementia and will decrease abuse, neglect, and unnecessary medications, ensuring proper training ensues.
Future research will move in the direction of including VDT in the broad‐spectrum educational projects carried out in the Italian territory. This approach will be useful not only to people directly involved in dementia care work, but also to the wider public to stimulate the development of a more inclusive attitude toward people living with dementia.
CONFLICTS OF INTEREST
Author disclosures are available in the supporting information.
Supporting information
Supporting Information
Supporting Information
ACKNOWLEDGMENTS
The authors would like to thank Gwenyth Johnson who made significant contributions to the article writing improvement, proofreading the draft manuscript, and providing language help. The open‐source version of this article is made possible by the University of Bergamos contribution to the publication (grant SUSTFAMORG22).
Morganti F, Brignoli P, Beville PK. The Italian version of the Virtual Dementia Tour: Manual translation and an analysis of consistency, validity, and reliability of its pre‐ post‐experience survey. Alzheimer's Dement. 2022;8:e12323. 10.1002/trc2.12323
REFERENCES
- 1. Olazarán J, Reisberg B, Clare L, et al. Nonpharmacological therapies in Alzheimer's disease: a systematic review of efficacy. Dement Geriatr Cogn Disord. 2010;30:161‐178. [DOI] [PubMed] [Google Scholar]
- 2. Kitwood T. Dementia Reconsidered: The Person Comes First. Open University Press; 1997. [Google Scholar]
- 3. Baron‐Cohen S, Wheelwright S. The empathy quotient: an investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. J Autism Dev Disord. 2004;34:163‐175. [DOI] [PubMed] [Google Scholar]
- 4. Decety J, Jackson PL. The functional architecture of human empathy. Behav Cogn Neurosci Rev. 2004;3:71‐100. [DOI] [PubMed] [Google Scholar]
- 5. Derksen F, Bensing J, Lagro‐Janssen A. Effectiveness of empathy in general practice: a systematic review. Br J Gen Pract. 2013;63:e76‐e84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Panyavin I, Trujillo MA, Peralta SV, et al. Examining the influence of family dynamics on quality of care by informal caregivers of patients with Alzheimer's dementia in Argentina. Am J Alzheimers Dis Other Demen. 2015;30:613‐621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Hattink B, Meiland F, van der Roest H, et al. Web‐based STAR E‐learning course increases empathy and understanding in dementia caregivers: results from a randomized controlled trial in the Netherlands and the United Kingdom. J Med Internet Res. 2015;17:e241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wijma EM, Veerbeek MA, Prins M, Pot AM, Willemse BM. A virtual reality intervention to improve the understanding and empathy for people with dementia in informal caregivers: results of a pilot study. Aging Ment Health. 2017;10:1‐9. [DOI] [PubMed] [Google Scholar]
- 9. Schaufeli WB, Maslach C, Marek T. Series in applied psychology: Social issues and questions. Professional burnout: Recent developments in theory and research. Taylor & Francis; 1993. [Google Scholar]
- 10. Shim B, Barroso J, Davis LL. A comparative qualitative analysis of stories of spousal caregivers of people with dementia: negative, ambivalent, and positive experiences. Int J Nurs Stud. 2012;49:220‐229. [DOI] [PubMed] [Google Scholar]
- 11. Beville PK. Virtual Dementia tour helps sensitize health care providers. Am J Alzheimers Dis. 2002;17:183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Beville PK. (2019). Dementia aware competency evaluation, DACE®. https://www.secondwind.org/dacereg.html
- 13. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross‐cultural adaptation of self‐report measures. Spine. 2000;25:3186‐3189. [DOI] [PubMed] [Google Scholar]
- 14. The jamovi project (2019). jamovi . (Version 1.0) [Computer Software]. https://www.jamovi.org
- 15. Morganti F. What intersubjectivity affords: paving the way for a dialogue between cognitive science, social cognition and neuroscience. In: Morganti F, Carassa A, Riva G, eds. Enacting Intersubjectivity: a cognitive and social perspective to the study of interactions. IOS Press; 2008. [Google Scholar]
- 16. Berthoz A, Thirioux B. A spatial and perspective change theory of the difference between sympathy and empathy. Paragrana, 2010;19:32‐61. 10.1524/para.2010.0003 [DOI] [Google Scholar]
- 17. Deci E, Ryan R. The “What” and “Why” of goal pursuits: human needs and the self‐determination of behavior. Psychol Inq. 2000; 11: 227‐268. [Google Scholar]
- 18. Baltes PB, Reese HW, Lipsitt LP. Life‐span developmental psychology. Annu Rev Psychol. 1980; 31: 65‐110. [DOI] [PubMed] [Google Scholar]
- 19. Likert R. A technique for the measurement of attitudes. Arch. psychol. 1932;140:1‐55. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information
Supporting Information