
Figure 3. FDG‐PET, echocardiogram, and CMR images from patients with isolated CS ( A through F) and CS with extracardiac involvement (G through J).
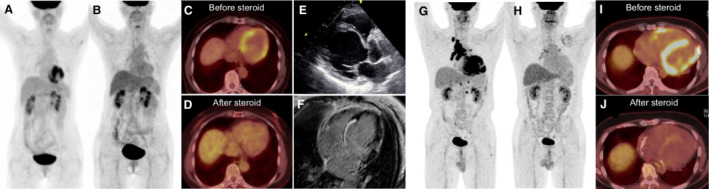
Panels A through F are images from a patient diagnosed with isolated CS. Maximum intensity projection (MIP; A) and axial image (C) of FDG‐PET demonstrate focal on diffuse myocardial uptake with SUVmax of 7.4. There was no FDG uptake in other organs. Echocardiogram also revealed prominent basal interventricular thinning with reduced left ventricular ejection fraction (E). CMR showed LGE in the basal interventricular septum and lateral wall (F). Follow‐up FDG‐PET evaluation after steroid therapy revealed improvement in myocardial uptake in MIP (B) and axial image (D) with SUVmax of 2.9. Panels G‐J show MIP (G and H) and axial images (I and J) of FDG‐PET images in another patient with CS with extracardiac involvement. Baseline FDG‐PET evaluation showed intense focal myocardial uptake (SUVmax 14.9; G and I) with hypermetabolic lymph nodes in the mediastinum and hilar regions. Administration of steroid therapy led to improvement in myocardial uptake (SUVmax 2.0; H and J). CMR indicates cardiac magnetic resonance imaging; CS, cardiac sarcoidosis; FDG, 18F‐fluorodeoxyglucose; FDG‐PET, 18F‐fluorodeoxyglucose positron emission tomography; LGE, late gadolinium enhancement; and SUVmax, maximum standardized uptake value.