
Fig. 1.
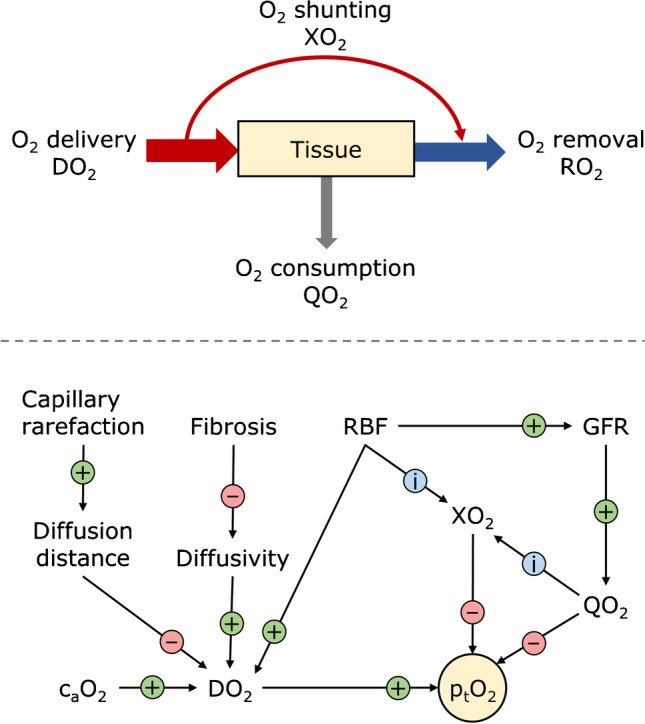
Key factors determining oxygen partial pressure in tissue. Top panel: Tissue oxygenation is a function of O2 delivery (DO2), consumption (QO2), and removal (RO2). About 10–15% of O2 delivered to the kidney is consumed under normal physiologic conditions. Not all renal tissues are supplied equally, which is, in part, due to arterial-to-venous oxygen shunting (XO2). O2 not consumed by the kidney is removed by venous efflux. Bottom panel: Tissue partial pressure of oxygen (ptO2) is dependent on factors that influence O2 delivery, consumption, and removal. Circled + and − signs indicate the effect of an increase in the factor upstream of the corresponding arrow on the parameter pointed by the arrowhead under the assumption that everything else remains the same. Circled i indicates that an increase in the respective factor will influence the indicated parameter. Only selected factors are shown. An increase in renal blood flow (RBF) increases DO2 and glomerular filtration rate (GFR), and may influence XO2. Whether XO2 increases is dependent on the location of the tissue under observation, among other factors. XO2 is also influenced by QO2. Since QO2 produces the arterial-to-venous pO2 gradients necessary for XO2, an increase in consumption will likely, but not necessarily, increase shunting; the local arrangement of O2 sinks and sources plays a role as well. More shunting leads to reduced ptO2. Increased GFR leads to higher QO2, as O2 demand for Na+ reabsorption increases, and thereby to reduced ptO2. DO2 increases with increased arterial blood oxygen concentration (caO2) and partial pressure. Capillary rarefaction and fibrosis reduce oxygen delivery to tissue due to increased diffusion distance and reduced diffusivity, respectively