
Fig. 2.
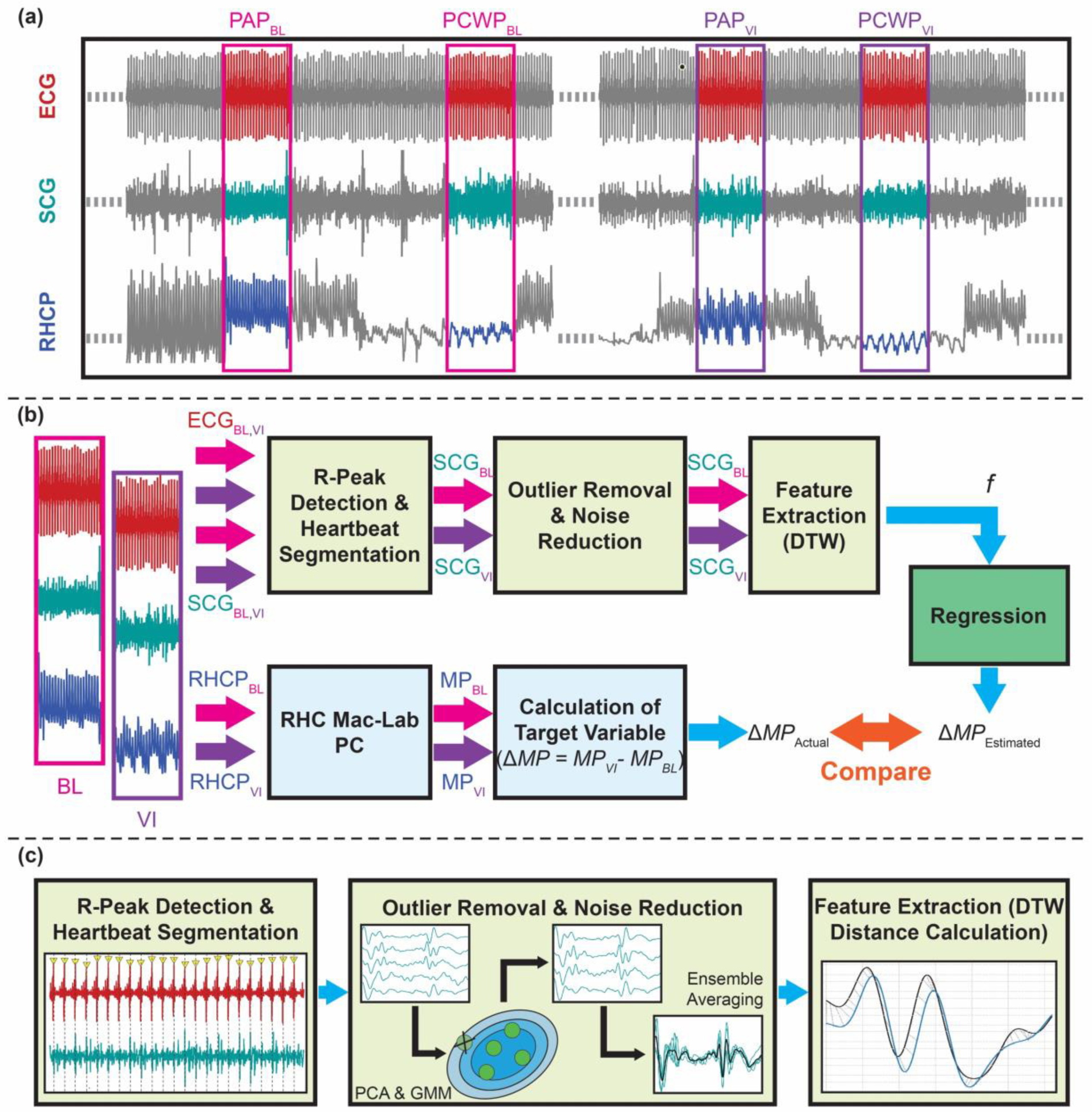
Overview of the method: (a) Wearable ECG and SCG (only showing one axis of the signal for simplicity) signals were synchronized with the right heart catheterization pressure (RHCP) signal. 20s long signals from both baseline (BL) and during vasodilator infusion (VI) were extracted when the catheter was recording pulmonary artery (PA) pressure and in pulmonary capillary wedge (PCW) pressure signals. (b) The R-peaks of the ECG signal were detected and later used to segment the corresponding SCG signals into individual heartbeats. Outlier removal and noise reduction steps were performed on the SCG heartbeats, and features were extracted to be used in the regression algorithm to estimate the changes in the RHC mean pressure (MP) values (e.g., changes in pulmonary artery mean pressure (ΔPAM), and changes in pulmonary capillary wedge mean pressure (ΔPCWP)). The MPBL and MPVI values were extracted from the RHC Mac-Lab computer and used to calculate the target variable (ΔPAM and ΔPCWP). (c) Details on the wearable signal processing: First, the R-peaks of the ECG signals were detected, and the SCG signals were segmented into individual heartbeats. Second, SCGBL and SCGVI heartbeats were passed through an outlier removal algorithm (using principal component analysis [PCA] and Gaussian mixture model (GMM)) and were ensemble-averaged to have two average SCG heartbeats per axis (one for BL and one for VI). Third, dynamic time warping (DTW) distances were calculated between the BL and VI heartbeats per axes and used as features (f) in the regression algorithm.