
Fig. 7.
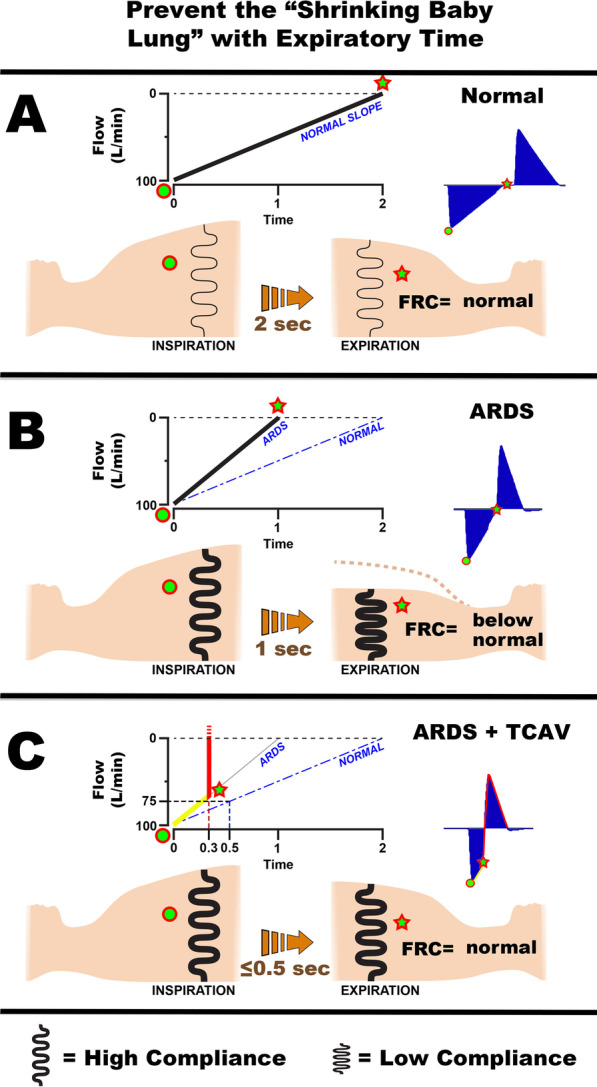
Using expiratory time and the airway pressure release ventilation (APRV) mode to maintain a normal functional residual capacity (FRC) and prevent progressive collapse of the ARDS lung (VILI vortex). A The Flow/Time curve (Fig. 4B) at the beginning of expiration (green dot) and at end expiration (Release Phase, red star). The normal lung is allowed to fully empty (Flow 0 L/min) to atmospheric pressure (0 cmH2O). The respiratory system compliance (CRS) in the normal lung is high, and therefore, the lung recoil is low (thin black spring). The slope of the expiratory flow curve (SlopeEF) is shallow (NORMAL SLOPE) taking ~ 2 s for the lung to fully empty. A functioning pulmonary surfactant system prevents lung collapse at atmospheric pressure, and FRC remains normal. The Flow/Time curve that would be seen on the ventilator monitor in blue (Fig. 4B, Gas Flow/Time). B ARDS diminishes surfactant function and dramatically decreases CRS, leading to increased lung recoil (thick black spring). This results in a steep SlopeEF (ARDS, solid black line) compared with a normal slope (NORMAL, dashed blue line). As a result, the lung empties rapidly (~ 1 s), and there is a marked reduction in FRC seem as large reduction in chest volume (green star). The Flow/Time curve that would be seen on the ventilator monitor in blue (Fig. 4B, Gas Flow/Time). C The TCAV method uses a fraction (75%) of the peak expiratory flow (100 L/min) to set the expiratory duration. Changes in the SlopeEF with decreasing CRS will modify the expiratory duration using this method (ARDS = 0.3 s; Normal = 0.5 s at the same 75% fraction). Note that in the ARDS lung the SlopeEF (yellow line) is steep and 75% is reached very rapidly (0.3 s) at which point the lung is rapidly re-inflated to the CPAP Phase (red line). In the normal lung, the SlopeEF is shallower and takes 0.5 s to reach 75% of the peak expiratory flow. The brief expiratory duration does not give the lung time to depressurize (Fig. 4B, TC-PEEP) or alveoli time to collapse (Fig. 6A, B, APRV 75%) maintaining a near normal FRC and preventing progressive lung collapse (VILI vortex). The Flow/Time curve that would be seen on the ventilator monitor in blue (Fig. 4B, Gas Flow/Time)