
Figure 3. 3.5‐s signal averaged tracing from the 26‐week fetus in Figure 2.
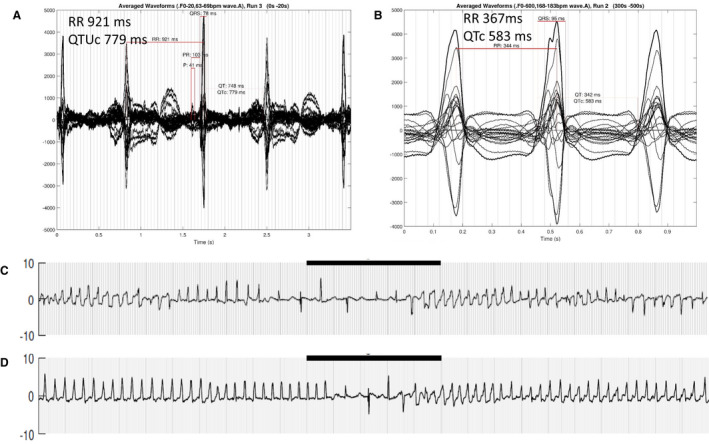
A, functional 2:1 AV block and marked QTU prolongation. B, 1‐s signal averaged tracing during monomorphic VT showing a very stable pattern of VT, unlike that seen typically with long QT syndrome. This fetus had both LQT1 and LQT2. The fetus required β‐blocker therapy pre‐ and postnatally, and a pacemaker and left stellate ganglionectomy after delivery. VT indicates ventricular tachycardia. C, Same fetus with periods of typical polymorphic torsades morphology. Black bar = 5 s. D, Same fetus, same run, showing the monomorphic‐appearing VT. Neither form of VT was recognized before fMCG, largely because of the relatively slow rate (163 beats/min), which was thought to be sinus rhythm. Both forms of VT responded in utero to maternal high‐dose propranolol therapy at 320 mg/d. AV indicates atrioventricular; LQT ‐ Long QT; TWA, T wave alternans; and VT, ventricular tachycardia.