
Fig. 6. SMCs from hypertensive patients show increased α1AR–TRPV4SMC and reduced TRPV4SMC–BK channel signaling.
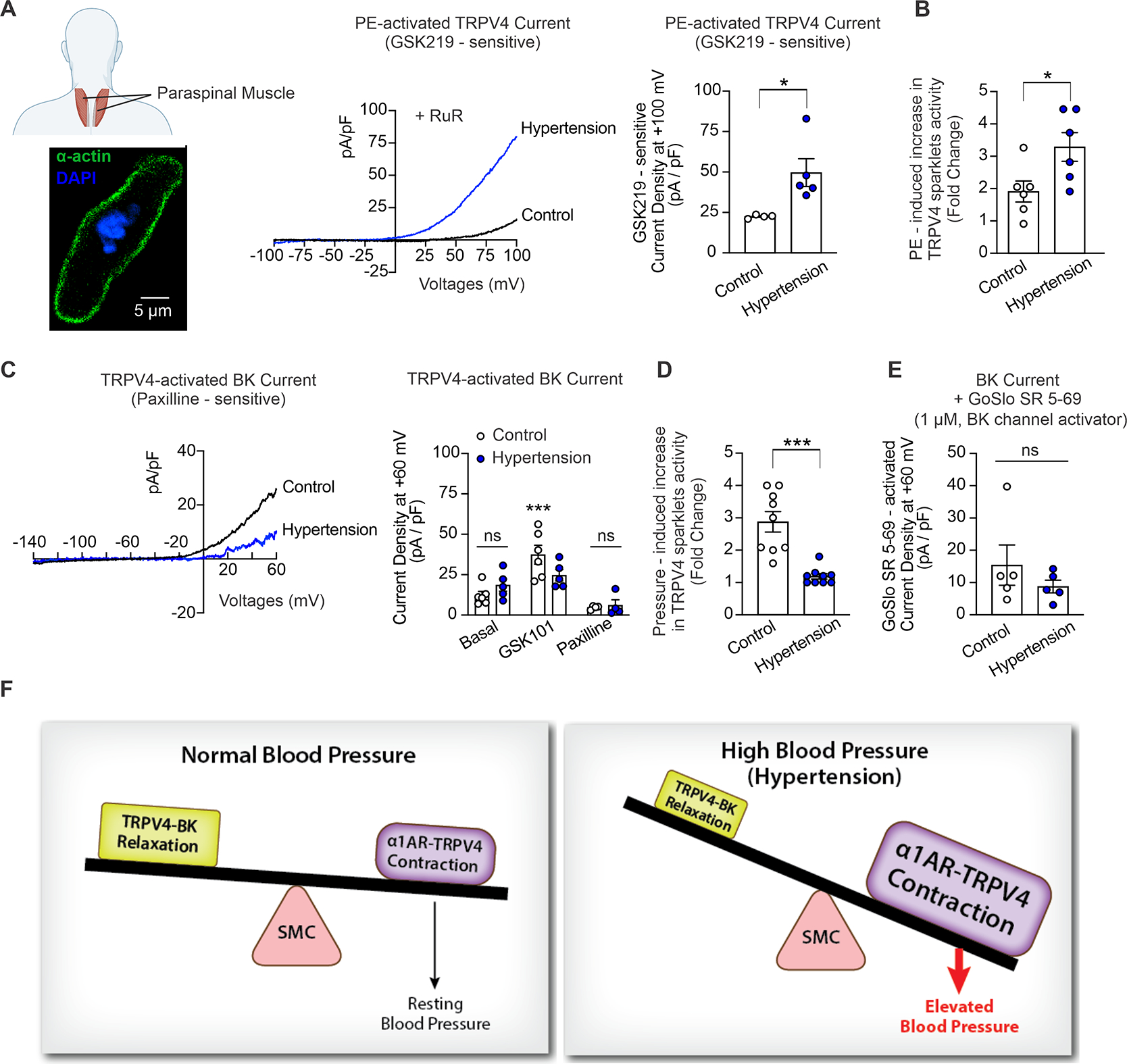
(A) Human vascular SMCs were isolated from paraspinal muscle arteries from non-hypertensive and hypertensive patients (1–2 SMCs per subject per treatment group for functional studies). The inset (Left bottom) shows widefield images of an isolated SMC from a human paraspinal muscle artery, stained for α-actin (green) and counterstained with the nuclear dye DAPI (blue). The fusiform shape (positive α-actin staining) is characteristic of isolated SMCs selected for patch-clamp experiments. Middle, representative whole-cell patch-clamp traces for PE (1 μM)-induced, GSK219 (100 nM)-sensitive ionic currents at +100 mV in SMCs freshly isolated from paraspinal muscle arteries of non-hypertensive (control) subjects and hypertensive patients at +100 mV. Right, averaged GSK219-sensitive outward currents (current at +100 mV in the presence of PE minus current in the presence of PE + GSK219 [100 nM]) in SMCs isolated from paraspinal muscle arteries from non-hypertensive (control, n = 4) subjects and hypertensive patients (n = 5) (*P < 0.05 vs. control, unpaired t-test). (B) PE-induced TRPV4SMC sparklet activity in non-hypertensive (n = 6) and hypertensive patients (n = 6). Pressurized human arteries were pretreated with CPA (20 μM), nifedipine (1 μM), and GSK101 (30 nM) (*P < 0.05 vs. Control; unpaired t-test). (C) Left, representative traces of GSK101 (30 nM)-induced, paxilline (1 μM)-sensitive BK currents in SMCs isolated from paraspinal muscle arteries of non-hypertensive (control) subjects and hypertensive patients, recorded in the whole-cell patch-clamp configuration. Right, averaged outward currents at +60 mV in SMCs isolated from paraspinal muscle arteries of non-hypertensive control subjects (n = 6) and hypertensive patients (n = 5) under basal conditions and in the presence of GSK101 (30 nM) and GSK101 + paxilline (1 μM) (***P < 0.001 vs. Basal; ns, not significant; two-way ANOVA). (D) Increased intraluminal pressure (from 20 mmHg to 80 mmHg)-induced TRPV4SMC sparklet activity in non-hypertensive (n = 9) and hypertensive patients (n = 9). Pressurized human arteries were treated with CPA (20 μM), nifedipine (1 μM), and GSK101 (30 nM) (***P < 0.001 vs. Control; unpaired t-test). (E) Averaged GoSlo SR 5–69-activated outward currents at +60 mV (current in the presence of GoSlo SR 5–69 minus currents before addition of GoSlo SR 5–69) in SMCs isolated from paraspinal muscle arteries from non-hypertensive control subjects (n = 5) and hypertensive patients (n = 5) (ns, not significant; unpaired t-test). (F) Schematic diagram showing the imbalance between α1AR:TRPV4SMC and TRPV4SMC:BK channel signaling in hypertension, which leads to increased constriction of resistance arteries and elevated blood pressure.