

Abstract
We formulate a MIDUS longitudinal data-based multi-population LISREL model to gauge variation among Black and White Americans in the reciprocal relationship across time between perceived major and everyday discrimination, and psychological distress. Two hypotheses building on prior theory and empirical findings are generated: reciprocity between perceived discrimination and distress, and stronger reciprocity among Blacks. Here, “reciprocity” denotes positive effects of perceived discrimination and mental health problems such as distress on each other across time. Both hypotheses are supported for relationships between perceived everyday discrimination and distress. The model controls for several potentially relevant variables.
Keywords: Perceived Discrimination, Psychological Distress, African-Americans, Stress and Coping, Race
The substantial role of discrimination in undermining Black Americans’ well-being and accounting for their subordinate socioeconomic position vis-à-vis Whites, in particular, is solidly documented (Bonilla-Silva 1996; Ellison, Musick, and Henderson 2008; Malat, Mayorga-Gallo, and Williams 2018; Pearlin et al. 2005; Quillian 2006). Social psychology-infused investigations have established the perception of discrimination as a chronic stressor to which Blacks are considerably more exposed than Whites, and as one that significantly undermines Blacks’ emotional well-being (Brown, Williams, and Jackson et al. 2000; Keyes 2009; Lee and Turney 2012; Malat, Mayorga-Gallo, and Williams 2018; Pearlin et al. 2005; Williams 2018). Fuller understanding of the role perceived discrimination plays in explaining connections between race and emotional well-being can be facilitated by research exploring a) reciprocal relationships between dimensions of perceived discrimination and key manifestations of emotional well-being; and b) the relative magnitude of these reciprocal perceived discrimination-emotional well-being relationships across races. The consequentialness of perceived discrimination to Black Americans’ mental health, for example, becomes established more comprehensively if this stressor is shown to not only undermine Blacks’ mental health, but to also be one that Blacks in poor mental health are likelier to become exposed to. If these reciprocal perceived discrimination-mental health relationships are also observed to be especially pronounced among Blacks, the consequentialness of perceived discrimination to Blacks’ mental health becomes even more soundly affirmed. Scant attention has been paid to the impact of emotional well-being on perceptions of discrimination in empirical investigations (Maryl and Saperstein 2013; Williams and Mohammed 2009). We explicate later that emotional well-being levels may shape both perceptions of given events as discriminatory, and (to the extent that personal agency can be impactful) the actual likelihood of discriminatory events occurring. The issue of possible racial variation in the perceived discrimination-emotional well-being relationship has received moderate attention at best; and utilization of cross-sectional rather than more theoretically appropriate longitudinal data has predominated. Longitudinal designs are generally preferable, since they facilitate clearer temporal separation of posited outcomes from predictors and statistical adjustment for baseline-levels of variables posited as outcomes. Incentivized by this goal of more thorough insight into the pertinence of perceived discrimination to connections between race and emotional well-being, we utilize longitudinal data to gauge variations among Black and White Americans in the reciprocal relationship between perceived major and everyday discrimination, and the mental health problem of psychological distress. Whites are an apt comparison group for Blacks for two main reasons that we elaborate on later: a) their dominant status in the American racial hierarchy and b) increasing resonance among them of the notion that discrimination is a consequential stressor in Whites’ lives. We posit that perceived discrimination dimensions and distress exert positive effects on each other, and that those reciprocal effects are more pronounced among Blacks. As will become apparent, we provide a detailed rationale for these two hypotheses that evolve from multiple prior empirical and theoretical contributions.
Background
Like many investigations exploring the relationship between perceived discrimination and emotional well-being, we draw heavily on Pearlin’s stress and coping perspective for theoretical underpinning (Pearlin 1999; Pearlin et al. 1981). A particularly relevant presumption of this perspective is that exposure to stressors – circumstances or events that hinder goal attainment or individuals’ normal adaptation capabilities – enhances one’s odds of experiencing mental health problems. Stressors have thus been typically posited as predictors of poor mental health. Even in the investigation that pioneered this hegemonic approach that posits stressors as predictors of emotional health, however, the potential for reciprocal effects is acknowledged: Pearlin et al. (1981: 351) concede, for example, the acceptability of a clinician “beginning” with depression in deciphering its connection to stressful life-events (emphasis added). Complexities inherent to stress and coping, they note, are more fully captured with attention to “multidirectionality.” Reciprocal relationships among manifestations of stress exposure and emotional well-being have been under-explored in studies incorporating the stress and coping perspective (Thoits 2010); and as indicated earlier, inattention to such reciprocity is generally conspicuous in studies addressing perceived discrimination. Furthermore, because stress and coping processes may differ across dominant and subordinate groups (Thoits 2010), investigations such as this assessment of Black-White variation in the reciprocal association between perceived discrimination and distress are particularly useful.
Major and everyday discrimination are the perceived discrimination dimensions examined most frequently in mental health-focused investigations. Major discrimination is so labeled because its occurrence may severely impede socioeconomic well-being. Everyday discrimination largely involves character assaults that may or may not impede socioeconomic well-being (Williams et al. 1997). The tendency for stressors to confront persons engaged in “ordinary – indeed, required – pursuits” (Pearlin and Schooler 1978: 3) is manifestly applicable to major and everyday discrimination.
African-Americans are significantly likelier than Whites to perceive both major and everyday discrimination (Williams 2018). A broad array of evidence – significantly reflecting the racist organization of American life – validates Blacks’ tendency to perceive more maltreatment. This evidence includes statistical studies and field experimental audits by impartial third parties that reveal pervasive anti-Black bias in employment, housing, governmental policy priorities, health care access, and other critical socioeconomic and institutional arenas (Ellison, Musick, and Henderson 2008; Malat, Mayorga-Gallo, and Williams 2018; Williams et al.). Additional validating evidence comes from experimental findings indicating widespread “implicit” bias against Blacks especially (Quillian 2006). Racism is sustained by classification and hierarchical organization of racial groups, with Blacks and other subordinate groups systemically disempowered, devalued, and allocated fewer desirable societal resources and opportunities. A culturally embedded ideology featuring socially generated and strategically curated hegemonic beliefs and stereotypes extoling whiteness and debasing blackness and other nonwhite statuses, facilitates racism (Bonilla-Silva 1996; Williams 2018). Discriminatory experiences that Blacks typically confront are rooted significantly in the racist structure of American social and economic life (Bonilla-Silva 1996; Williams 2018; Williams et al. 1997).
Their group’s dominant status in America’s racial milieu notwithstanding, nontrivial percentages of Whites either perceive discrimination or consider it a stressor germane to Whites’ experiences. As many as 38% of Whites nationally have reported experiencing racial discrimination personally (Maryl and Saperstein 2013). Additionally, 50% of Whites in a recent national survey contended that discrimination against White Americans is as big a problem as discrimination against Blacks (Malat, Mayorga-Gallo, and Williams 2018). In similar vein, by an average of more than one point on a 10-point scale, Whites in a separate national survey rated “reverse” anti-White discrimination as more widespread than anti-Black bias (Norton and Sommers 2011). Discrimination is thus seemingly on the perceptual “radar” of Black and White Americans; and this context renders it possible for significant relationships between perceived discrimination and mental health problems to prevail over time in either race. The pertinence of specific stressors to a group’s well-being hinges significantly on the relative magnitude, vis-a-vis appropriate contrast groups, of the relationship between those stressors and well-being. Therefore, this investigation of variation in the reciprocal relationship between the stress of perceived discrimination and problem of distress in a subordinate versus dominant racial group seems especially worthwhile.
The possible association between portrayals of discrimination as a significant stressor in Whites’ lives and the ideology upholding whiteness is noteworthy. Expositions on racism using “whiteness” lexicon (e.g., Malat, Mayorga-Gallo, and Williams 2018) detail multi-faceted ways in which racist systems prioritize advantaging persons of European descent and disadvantaging others. Various material and non-material resources have accrued disproportionately to White Americans via such prioritizing. Prominent historical and contemporary examples include preferred access to government-backed home financing (with accelerated paths to asset accumulation and access to better jobs, schooling, homes and neighborhoods figuring among derivative benefits), more favorable and affirming portrayals in media and popular culture, and a firmer foothold in the sharing economy (Malat, Mayorga-Gallo, and Williams 2018: 153). Two elements of the ideology supporting whiteness seem especially relevant to this investigation: 1) widespread expectation by Whites of socioeconomic success – particularly vis-à-vis Blacks and other nonwhites, and 2) downplaying the contribution of structural factors to inequality between groups in favor of explanations emphasizing values- and habit-related phenomena (Malat, Mayorga-Gallo, and Williams 2018). These planks upholding the ideology of whiteness seemingly yield conflicting presumptions regarding how the relationship between perceived discrimination and distress varies racially.
Stronger expectation of material and social success by Whites may result in them experiencing discrimination as a stressor more so than Blacks, and culminate in a stronger positive impact of discrimination on Whites’ distress. Given the earlier-noted status of discrimination as an elemental structural contributor to racial differences in well-being, expectation of relative success arguably suggests anticipation of existences that are relatively discrimination-free. Subordinate status in the whiteness hierarchy likely militates against Blacks expecting relatively discrimination-free existences. If lower expectation of discrimination is indeed germane to it being experienced as a stressor, the presumption that perceived discrimination promotes distress especially among Whites follows logically. This very presupposition undergirds the “psychological immunity” thesis invoked in some investigations of Black-White mental health differences: Prolonged exposure to discrimination, or socialization about discrimination-related adversity, equips Blacks with sturdier emotional resources to handle its strain. For example, Kessler, Mickelson, and Williams (1999: 209) suggest that groups exposed to systemic discrimination may develop emotion-focused coping strategies that blunt their damaging effects on mental health.
The element of whiteness ideology that features gainsaying of structural factors and prioritizing of values- and habit-based phenomena as explanations for inequality, is arguably suggestive of a relatively positive impact of perceived discrimination on Blacks’ distress. If the system of whiteness that privileges Whites and undermines Blacks is indeed fundamentally structural, then all other things being equal, Whites’ perceptions of discrimination may be construed as less genuine or credible than Blacks.’ Since odds of discrimination being experienced as a stressor likely strengthen in contexts where perceptions are relatively genuine or credible, Blacks would then be the group with more intense experiences. Anticipation of a stronger positive impact of perceived discrimination on Blacks’ distress then ensues. We review empirical findings regarding this question of Black-White variation in the impact of perceived discrimination on distress later, along with evidence addressing the less studied question of Black-White variation in the reciprocal impact of distress on perceived discrimination. We then formulate a hypothesis drawing on these prior findings, and on theoretical contributions.
Notwithstanding higher exposure to discrimination and many other stressors, African-Americans typically experience similar or lower levels of psychological distress and psychiatric disorder rates vis-à-vis Whites (Keyes 2009; Williams 2018). Distress denotes an unpleasant state of mind, and is a widely experienced problem occupying the negative end of the mental health continuum. Its primary components are depression and anxiety, the commonest manifestations of mental health problems. Depression encompasses mood-related symptoms such as sadness, worthlessness or suicide ideation, and malaise-related symptoms such as crying, poor appetite, and difficulty sleeping or concentrating. Anxiety encompasses symptoms such as restlessness, fear, and irritability. Depression and anxiety are “experienced by everyone to some degree at some time,” and are “especially useful indicators of subjective quality of life” (Ross and Mirowsky 2003: 411–16). General or nonspecific distress scales like the one we utilize tap constellations of mental health problems in populations, but are not designed to discretely identify persons with clinically significant conditions (Kessler et al. 2002). Notably, this assessment of Black-White variation in the reciprocal relationship between perceived discrimination and distress facilitates further exploration of Keyes (2009) intriguing contention that African-Americans’ mental health-specific “flourishing in the face of social inequality” would be more pronounced if not for discrimination. The absence of evidence suggesting physical health-related “flourishing” among Blacks warrants acknowledgment: Indications that stressful life-events induce chronic illness among Blacks more so than Whites (Jackson, Knight, and Rafferty 2010), are illustrative. The intriguing derivative question of whether the stress of discriminatory encounters is inordinately tied to the physical health of specific races, is outside the scope of this investigation.
Reciprocity between Discrimination and Distress? Insights from Prior Investigations
Stressors factor integrally in “chains” of mental health-related adversity that may ensnare individuals throughout the lifecourse (Pearlin et al. 2005). Stress proliferation, the adversarial chain involving exposure to initial “primary” stressors inducing exposure to “secondary” ones (Aneshensel 2015; Pearlin et al. 2005; Thoits 2010), has received substantial attention. Reciprocity across time between the stress of perceived discrimination and mental health problem of distress – perceived discrimination fostering distress and distress fostering perceived discrimination – is the distinct potential adversarial chain that we spotlight here.
Adversarial chains are also a salient underlying theme in Merton’s Matthew effect thesis, and the derivative concept of cumulative (dis)advantage. The Matthew effect involves persons possessing advantages accruing more over time, and those without gradually losing what they have (Merton 1968). Disadvantages of central theoretical relevance here are perceived major and everyday discrimination, and distress. The broad-spectrum mechanism of cumulative (dis)advantage facilitates perpetuation of inequality between groups at different social structural locations (e.g., races) across temporal processes such as the lifecourse. Favorable positions redound to additional relative gains across time, and unfavorable ones to additional losses (DiPrete and Eirich 2006: 271). Invoking the cumulative disadvantage theme, Pearlin et al. declare heightened exposure to chronic, often recurrent stressors like discrimination “inherent” to subordinate structural location. Such sustained exposure may cumulatively undermine individuals’ adaptational capabilities, and thus impair their health over time (Pearlin et al. 2005: 213–14). To the extent that we observe reciprocity between the stress of perceived discrimination and incisive mental health indicator of distress prevailing with differential intensity among Black and White Americans, the pertinence of discrimination to race-based mental health patterns would be affirmed all the more. Prior investigations provide good insight into why perceived discrimination and mental health problems might reinforce each across time. The potential impact of perceived discrimination on mental health problems suggested by these studies is elucidated next, followed by the reciprocal impact of mental health problems on perceived discrimination.
The capacity for perceived discrimination to undermine mental health derives from its status as a stressor. Chronic stress exposure may confront persons “with dogged evidence … inescapable proof of their inability to alter” life’s unwanted circumstances, and induce cripplingly negative interpretations of those strains (Pearlin et al. 1981: 338–39). Brown, Williams, and Jackson et al. (2000) posit a similarly deleterious impact of perceived discrimination: Intensified feelings of loss, ambiguity, strain, frustration, and injustice typically ensue. The above theses implicitly portray symptoms of distress as outcomes of stress exposure; and congruent patterns have been observed in several investigations examining perceived discrimination (e.g., Kessler, Mickelson, and Williams 1999; Keyes 2009; Lee and Turney 2012; Mossakowski 2003).
The impact of mental health or related constructs on perceived discrimination has received significantly less attention than the reciprocal relationship (Maryl and Saperstein 2013; Williams and Mohammed 2009); and mixed patterns are apparent in the four empirical investigations we located. Brown, Williams, and Jackson et al. (2000) observe a non-significant impact of distress and clinical depression on perceived racial discrimination in a Black American panel. Similarly, Pavalko, Mossakowski, and Hamilton (2003) detect a non-significant distress effect on perceived workplace discrimination in a panel of employed women. By contrast, Brody et al. (2006) observe a positive impact of problem behaviors (which incorporate depression indicators) on discrimination perceptions in an African-American adolescent panel. The fourth investigation (Phinney, Madden, and Santos 1998) assesses minority and immigrant adolescents, and finds negative associations between discrimination self-reports and favorable self-appraisals. The authors acknowledge that its cross-sectional design obscures the actual causal direction of the relationships.
Among the investigations referenced above, only Phinney, Madden, and Santos (1998: 940–48) elaborate on why emotional health might influence discrimination perceptions. They reason persuasively that poor mental health triggers a more downcast view of the world, which predisposes individuals to perceive discrimination. Pavalko, Mossakowski, and Hamilton (2003: 20) echo this theme while positing a greater likelihood of distressed persons defining workplace experiences as discriminatory. Similarly, Meyer (2003:263) suggests that emotionally healthier individuals are predisposed to “maximize perceptions of personal control and minimize recognition of discrimination” in ambiguous situations. These theses all suggest a positive impact of poor mental health on perceived discrimination.
The potential for mental health to influence perceived discrimination, however, likely extends beyond its connection to favorable definitions of circumstances. Inasmuch as the self is not merely a social product, but a social force (Rosenberg 1990), it may not merely shape interpretation of events. It may also shape their objective content. [This self-concept-focused thesis seems applicable given the strong association between favorable self-appraisals and more direct mental health indicators like distress (Pearlin et al. 1981; Rosenberg 1990)]. “Armed” with sturdy emotional health, individuals should be less prone to tolerate unfair treatment. Furthermore, should such treatment occur, the aggrieved would be better motivated and equipped to effect its cessation, and perhaps to even obtain recompense from, or punishment for perpetrators. Essentially, holding constant environmental constraints that are unmodifiable via personal agency, emotionally healthy persons are probably less docile and penalty-free targets for discrimination: They can more readily marshal social, economic, and psychological resources to forestall or counter such maltreatment. Thus predispositions to define circumstances favorably aside, emotionally healthy persons are probably also less likely to be in situations construable as discriminatory. Commensurately, Thoits (2006: 311) argues that “mentally healthy individuals select themselves out of particular life events and strained circumstances” (emphasis added), and cope more effectively than the mentally unhealthy when confronted by stressful situations “that cannot be evaded.” [The status of discrimination as a stressor seemingly renders this selectivity argument relevant here, although discrimination isn’t explicitly referenced in Thoits’ discussion]. Several insights from theoretical contributions and empirical findings thus support the thesis of a positive reciprocal association between perceived discrimination and mental health problems like distress. Given our interest in ascertaining whether such reciprocity is more pronounced among Black or White Americans, research pertinent to this specific question warrants examination.
Black-White Variation in Reciprocity between Perceived Discrimination and Distress?
Assessments of racial variation in the relationship between perceived discrimination and distress or related mental health problems have been rare. (For exceptions, see Kessler, Mickelson, and Williams 1999; Lee and Turney 2012; Pavalko, Mossakowski, and Hamilton 2003; Ren, Amick, and Williams 1999; Salvatore and Shelton 2007; Williams et al. 1997.) All but the Pavalko-Mossakowski-Hamilton investigation address the impact of perceived discrimination on mental health-related constructs exclusively, leaving possible reciprocal effects unaddressed.
All the above-cited investigations save for Lee and Turney (2012) invoke the “psychological immunity” thesis referenced earlier. To reiterate, this thesis posits that discrimination is less harmful to Blacks’ mental health than Whites,’ since greater experience with and anticipation of discrimination renders Blacks more equipped to ward off its damage. Greater immunity from discrimination among Blacks, it bears noting, lessens odds of a stronger feedback loop between perceived discrimination and mental health problems among them vis-à-vis Whites. Tellingly perhaps, support for the psychological immunity thesis in these six investigations is tepid: Some find no race difference in the impact of discrimination on mental health outcomes (Lee and Turney 2012; Pavalko, Mossakowski, and Hamilton 2003). Others find limited evidence that Blacks’ psychological distress is more strongly affected by discrimination, compared to Whites (Kessler, Mickelson, and Williams 1999; Ren, Amick, and Williams 1999). Ultimately, Kessler, Mickelson and Williams portray the disorder patterns observed in some studies as signaling that Blacks are “doubly disadvantaged”: They experience more discrimination, and are more adversely affected by those experiences. Such a pattern enhances the possibility of stronger reciprocity between perceived discrimination and distress among Blacks vis-à-vis Whites. Additionally, in the same study reporting a stronger detrimental impact of “blatant” discrimination on cognitive functioning among Whites (Salvatore and Shelton 2007), a more harmful impact of “ambiguous” discrimination on Blacks’ functioning is also observed. Intriguingly, the investigators suggest that disproportionately harmful effects of discrimination on Blacks’ emotional health “ultimately become manifest” over the longer term (Salvatore and Shelton 2007: 814). Congruently, Gee and Walsemann (2009: 1681–82) suggest that chronic stressors like perceived discrimination require “time to manifest” into illness. Our investigation examines longer-term effects exclusively; and we anticipate a more positive impact of perceived discrimination constructs on distress among Blacks.
Given the predominance of literature exclusively addressing the impact of perceived discrimination on constructs tapping emotional suffering, the absence of empirical investigations of Black-White variation in the reciprocal impact of mental health on perceived discrimination is unsurprising. However, likely patterns are inferable. To begin with, evidence indicates that personal histories of experiencing discrimination predispose individuals to “notice, recall, and report” subsequent experiences (Meyer 2003:263). Pearlin et al. (2005: 209) label this inclination among persons previously discriminated against “a state of vigilant anticipation.” Various forms of evidence, as noted earlier, point to Blacks being significantly likelier than Whites to experience discrimination. Of even more potential relevance is evidence portraying Blacks as likelier than Whites to be in states of “heightened vigilance” toward discrimination (Williams 2018). Thus there is seemingly greater potential for given predictors like distress to influence perceived discrimination among Blacks than among Whites: Odds of variation in perceived discriminatory experiences are likely higher among Blacks. Furthermore, the previously discussed factors that may inordinately expose distressed persons to discrimination arguably apply especially to those from subordinate backgrounds. The often cumulative disadvantages tied to subordinate structural location likely augment those intertwined with distress to generate greater exposure to discriminatory encounters. Additionally, if discrimination harms Blacks’ mental health more than Whites’ – as segments of Kessler, Mickelson, and Williams (1999) results indicate – such patterns may predispose Blacks in particular to connect mental health problems to discrimination. In effect, distressed states may induce vigilant anticipation of subsequent discrimination, and initiate the previously hypothesized reciprocity between perceived discrimination and distress among Blacks especially.1 For all the reasons articulated above, we anticipate a more positive impact of distress on perceived discrimination among Blacks.
The model we formulate facilitates assessment of whether the anticipated reciprocity between perceived discrimination and distress is indeed more pronounced among Black vis-à-vis White Americans. It includes statistical controls for constructs routinely observed or portrayed as consequential to the perceived discrimination-distress relationship – specifically, 1) coping resources of mastery and emotional support from others, 2) exposure to stressors other than perceived discrimination, and 3) aspects of social structural location other than race. Fittingly as well for a longitudinal study, the model includes statistical controls for effects of initial levels of perceived discrimination and distress upon the corresponding constructs observed subsequently (i.e., “stability” effects).
Hypotheses
To reiterate, we pose the following hypotheses:
H1: Reported experiences of discrimination will be positive predictors of subsequent psychological distress; and psychological distress will be a positive predictor of subsequent reported experiences of discrimination.
H2: The effects described in H1 will be stronger for Blacks than Whites.
Methods
Data
The 1995–‘96 and 2004–‘06 waves of the Midlife in the United States (MIDUS) surveys are utilized. MIDUS includes widely utilized, theory-informed indicators of perceived discrimination, distress and variables that may significantly influence these outcomes. The core group of “MIDUS1” respondents is a national probability sample of noninstitutionalized, English-speaking adults in the 48 contiguous states, ages 25 to 74. This core was augmented by probability oversamples of Blacks and Latinos from selected metropolitan areas, twins, and siblings. [More details on MIDUS samples and are obtainable at http://midus.colectica.org/]. Pursuit of the present investigation using the combination of “MIDUS2” and the “MIDUS3” wave collected 2013–’14 is unfeasible, as only 91 Blacks completed both the main and self-administered questionnaires at these most recent waves. Our analytical sample comprises the 3,561 White and 163 Black respondents to the self-administered and telephone portions of MIDUS1 and MIDUS2. Several critical questions were asked in the self-administered portions that were distributed via mail; and those portions had significantly lower response rates than the telephone-administered portions. Whites and Blacks analyzed here respectively represent 65% and 45% of the White and Black participants in the telephone and mail segments of MIDUS1. These respondents identified their main racial origin as “White” or “Black and/or African American” at either wave, and originated from either the core or a supplementary sample. Supplementary sample participants are included to maximize cases for Blacks, whose numbers are relatively low. We conducted two sets of preliminary analyses to address doubts that may arise about the representativeness of the Black subsample – in light of its smallness linked to the higher across-wave attrition rate for Blacks versus Whites. These analyses enhance confidence in the representativeness of the Black subsample. We detail them later.
Variables
Major and everyday discrimination items are typically summed, so as to capture the cumulative property of unfair treatment that research on perceived discrimination emphasizes (Williams et al. 1997; 2012). Thus perceived major discrimination at each wave is the sum across items gauging the following seven lifetime experiences attributed by the respondent to discrimination: being fired or denied promotion, not hired, treated unfairly by police, discouraged from furthering education, discouraged from seeking a job, prevented from renting or purchase a home by a landlord or realtor, and having neighbors who beleaguer. [For each experience, one or more incidences are coded 1, whereas no incidences are coded 0. These scores are summed over the seven experiences to produce a major discrimination score ranging from 0 to 7]. Perceived everyday discrimination at each wave is the sum across Likert-scaled items tapping the following experiences construed as discriminatory: being treated with less courtesy than others, accorded less respect, receiving poorer service than others at restaurants/stores, having people act as if “you are not smart,” “they are afraid of you,” “you are dishonest,” “you are not as good” as them, and being called names, “insulted,” “threatened,” or “harassed.” [Response options range from 1 = never to 4 = often for all items].
Psychological distress at each wave is a latent construct comprising indicators of nonspecific distress (Kessler et al. 2002). Items query instances in the past month (0 = none of the time to 5 = all of the time) when the respondent felt: so sad that nothing could cheer him/her up, nervous, restless or fidgety, hopeless, everything was an effort, worthless, cheerful, in good spirits, extremely happy, calm and peaceful, satisfied, and full of life.
Several control variables gauged at wave one are included as predictors of the discrimination and distress outcomes at wave two. They tap stressors, coping resources, or sociodemographic factors often portrayed as potentially consequential to stress or mental health problems among Blacks or Whites. A latent mastery construct comprises 11 items mirroring those developed by Pearlin and Schooler (1978): e.g., “I can do just about anything I … set my mind to,” and “what happens in my life is … beyond my control.” [Response options range from 1 = disagree strongly to 7 = agree strongly for all indicators. See Table 1 for the full list]. A latent emotional support construct combines several items gauging positive or negative support from close family members or friends: “How much do members of your family/your friends really care about you?”; “… understand the way you feel about things?” “… can you rely on your family members/your friends if you have a serious problem?”; “… can you open up to family/your friends if you need to talk about your worries?”; “How often do members of your family/your friends make too many demands on you?”; “… criticize you?” “… let you down when you are counting on them?”; and “… get on your nerves?” [Response options are 1 = not at all, 2 = a little, 3 = some, 4 = a lot]. We acknowledge that positive and negative emotional support and receipt of such support from specific sources (e.g., close family versus friends) are frequently analyzed as separate constructs. However, utilization here of a single support construct seems reasonable for three main reasons: 1) the secondary theoretical importance of emotional support in this investigation and related interest mainly in the collective impact of specific forms of support; 2) the uniformly non-problematic factor loadings of the latent construct’s indicators – with all loadings in each race exceeding the .3 threshold for “acceptable” and most exceeding the .5 threshold for “solid” (see Table 1); and c) the fact that key findings are unchanged when support is gauged as four constructs instead of one (each construct tapping positive/negative support from close family/friends).
Table 1.
Descriptive statistics for analyzed variables, and completely standardized LISREL loadings for latent constructs.
| MIDUS Wave One (1995– ‘96) | MIDUS Wave Two (2004– ‘06) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Blacks | Whites | Blacks | Whites | |||||||||
| Variable | Loading | Mean | Std. Dev | Loading | Mean | Std. Dev | Loading | Mean | Std. Dev | Loading | Mean | Std. Dev |
| Major Discrimination | – | 2.6 | 2.72 | – | .78 | 1.65 | – | 2.4 | 2.43 | – | .920 | 1.80 |
| Everyday Discriminat. | – | 18.9 | 6.20 | – | 12.3 | 4.09 | – | 17.5 | 6.21 | – | 12.5 | 4.16 |
| Psychological Distress | ||||||||||||
| So sad … | .672 | 1.55 | .915 | .672 | 1.37 | .676 | .645 | 1.59 | .922 | .645 | 1.35 | .656 |
| Nervous | .574 | 1.71 | .950 | .571 | 1.80 | .846 | .597 | 1.78 | .925 | .539 | 1.77 | .815 |
| Restless/fidgety | .604 | 1.63 | .897 | .536 | 1.74 | .834 | .663 | 1.80 | 1.04 | .512 | 1.73 | .812 |
| Hopeless | .756 | 1.33 | .773 | .684 | 1.25 | .615 | .821 | 1.52 | .976 | .637 | 1.24 | .603 |
| Everything an effort | .697 | 1.69 | 1.126 | .643 | 1.57 | .838 | .707 | 1.86 | 1.59 | .613 | 1.62 | .860 |
| Worthless | .715 | 1.33 | .809 | .621 | 1.26 | .639 | .746 | 1.40 | .889 | .603 | 1.25 | .636 |
| Cheerful | −.796 | 3.69 | .810 | −.778 | 3.62 | .681 | −.824 | 3.68 | .785 | −.795 | 3.63 | .676 |
| In good spirits | −.826 | 3.76 | .754 | −.806 | 3.72 | .667 | −.808 | 3.84 | .704 | −.824 | 3.74 | .659 |
| Extremely happy | −.691 | 3.13 | .962 | −.707 | 2.94 | .934 | −.720 | 3.25 | 1.07 | −.707 | 2.93 | .958 |
| Calm and peaceful | −.762 | 3.58 | .914 | −.761 | 3.42 | .874 | −.764 | 3.65 | .926 | −.744 | 3.48 | .847 |
| Satisfied | −.707 | 3.51 | .925 | −.790 | 3.48 | .921 | −.776 | 3.51 | .934 | −.778 | 3.52 | .888 |
| Full of life | −.701 | 3.61 | .952 | −.779 | 3.28 | .996 | −.773 | 3.55 | 1.06 | −.757 | 3.25 | .997 |
| Mastery | ||||||||||||
| There is little I can do … | −.653 | 2.96 | 2.214 | −.569 | 2.55 | 1.790 | – | – | – | – | – | – |
| I often feel helpless … | −.753 | 3.01 | 2.056 | −.707 | 2.66 | 1.807 | – | – | – | – | – | – |
| I can do … anything … | .444 | 6.20 | 1.343 | .444 | 5.86 | 1.357 | – | – | – | – | – | – |
| Others determine … | −.746 | 2.29 | 1.895 | −.618 | 2.07 | 1.497 | – | – | – | – | – | – |
| … beyond my control | −.754 | 2.69 | 2.065 | −.645 | 2.68 | 1.816 | – | – | – | – | – | – |
| … find a way to succeed | .298 | 6.24 | 1.216 | .412 | 6.02 | 1.211 | – | – | – | – | – | – |
| … many things interfere | −.567 | 4.26 | 2.079 | −.530 | 3.79 | 1.928 | – | – | – | – | – | – |
| I have little control … | −.819 | 2.70 | 2.023 | −.684 | 2.44 | 1.586 | – | – | – | – | – | – |
| … no way I can solve … | −.835 | 2.13 | 1.781 | −.689 | 1.88 | 1.306 | – | – | – | – | – | – |
| … being pushed around | −.671 | 2.73 | 2.064 | −.623 | 2.59 | 1.832 | – | – | – | – | – | – |
| … depends on me | .263 | 6.27 | 1.295 | .369 | 6.04 | 1.351 | – | – | – | – | – | – |
| Emotional Support | ||||||||||||
| Family cares | .620 | 3.70 | .593 | .574 | 3.77 | .523 | – | – | – | – | – | – |
| Family understands | .736 | 3.14 | .886 | .685 | 3.19 | .783 | – | – | – | – | – | – |
| Can rely on family | .644 | 3.51 | .776 | .574 | 3.64 | .684 | – | – | – | – | – | – |
| Can open up to family | .733 | 3.22 | .949 | .667 | 3.27 | .843 | – | – | – | – | – | – |
| Family too demanding | −.500 | 2.20 | .856 | −.371 | 2.12 | .752 | – | – | – | – | – | – |
| Family criticizes | −.562 | 2.22 | .834 | −.498 | 2.07 | .733 | – | – | – | – | – | – |
| Family lets R down | −.668 | 2.10 | .853 | −.545 | 1.94 | .745 | – | – | – | – | – | – |
| Family gets on nerves | −.606 | 2.37 | .921 | −.521 | 2.25 | .756 | – | – | – | – | – | – |
| Friends care | .632 | 3.34 | .806 | .545 | 3.42 | .661 | – | – | – | – | – | – |
| Friends understand | .607 | 3.18 | .843 | .521 | 3.14 | .722 | – | – | – | – | – | – |
| Can rely on friends | .538 | 3.17 | .885 | .484 | 3.32 | .780 | – | – | – | – | – | – |
| Can open up to friends | .490 | 3.16 | .928 | .465 | 3.15 | .834 | – | – | – | – | – | – |
| Friends too demanding | −.470 | 1.96 | .829 | −.327 | 1.89 | .624 | – | – | – | – | – | – |
| Friends criticize | −.452 | 1.96 | .726 | −.349 | 1.83 | .593 | – | – | – | – | – | – |
| Friends let R down | −.565 | 2.06 | .806 | −.436 | 1.92 | .631 | – | – | – | – | – | – |
| Friends get on nerves | −.415 | 2.16 | .797 | .373 | 2.02 | .643 | – | – | – | – | – | – |
| Chronic Financial Stress | ||||||||||||
| Rating of $ situation | −.910 | 5.77 | 2.55 | −.858 | 6.32 | 2.06 | – | – | – | – | – | – |
| Control over $ situation | −.676 | 7.06 | 2.72 | −.621 | 6.76 | 2.37 | – | – | – | – | – | – |
| $ to meet needs | −.605 | 1.59 | .606 | −.701 | 1.95 | .651 | – | – | – | – | – | – |
| Difficulty paying bills | .777 | 2.40 | .920 | .777 | 2.04 | .863 | – | – | – | – | – | – |
| Socioeconomic Status | ||||||||||||
| Education level | .518 | 6.33 | 2.50 | .471 | 7.15 | 2.47 | – | – | – | – | – | – |
| HH income last year | .564 | 53 g | 53.1 g | .658 | 76 g | 61.5 g | – | – | – | – | – | – |
| Chronic Ill-Health | ||||||||||||
| Self-rated physical health | −.478 | 3.90 | .966 | −.416 | 3.78 | .878 | – | – | – | – | – | – |
| Chronic health conditions | .328 | 2.50 | 2.55 | .703 | 2.31 | 2.35 | – | – | – | – | – | – |
| Activity limitations | .613 | 11.1 | 5.58 | .606 | 9.18 | 3.92 | – | – | – | – | – | – |
| Age | – | 46.5 | 11.95 | – | 47.5 | 12.46 | – | – | – | – | – | – |
| Gender (Female = 1) | – | .656 | .476 | – | .549 | .498 | – | – | – | – | – | – |
Minimum Fit Function Chi-square = 51,306/9058 df. RMSEA = .061.
A latent financial strain construct combines items gauging the respondent’s rating of his/her current financial situation (0 = worst possible … 10 = best possible), the amount of control s/he has over it (0 = “none” .… 10 = “very much”), whether available funds can meet financial obligations (1 = “not enough,” 2 = “just enough,” 3 = “more than” needed), and difficulty involved in paying monthly bills (1 = not at all difficult … 4 = very difficult). Chronic ill-health is a latent construct combining self-rated physical health vis-à-vis most men/women the respondent’s age (1 = much worse … 3 = about the same … 5 = much better), chronic conditions, and activity limitations. The chronic condition item sums across several indicators (0 = no; 1 = yes) gauging ailments experienced in the preceding year, e.g., asthma/bronchitis/emphysema, diabetes, bone/joint diseases, persistent back, stomach, mouth/gum/teeth, urinary tract/bladder, or hernia problems, migraines, AIDS/HIV, MS, or strokes. The activity limitations item sums indicators gauging how frequently health issues render these activities impossible: lifting/carrying groceries, bathing/dressing, climbing stairs, bending/kneeling/stooping, walking more than a mile, and one/several blocks. [Response options range from 1 = not at all … 4 = a lot for these activities]. Socioeconomic status is a latent construct combining respondent’s level of education (1 = no school/some grade school … 12 = Ph.D., MD, etc.), and total household income the preceding year. Age in years and gender (female = 1) are the other sociodemographic control variables.
Analytical Strategy
We formulated a LISREL8.8 multi-population model (Jöreskog and Sörbom 2003) to assess Black-White variation in the reciprocal relationship between perceived discrimination and distress across time. We began by using LISREL8.8-PRELIS’multiple imputation feature to replace missing data on all observed variables with imputed values reflecting within-case patterns occurring across other variables with non-missing data. Imputed values inserted by PRELIS are the average of those obtained over 12 iterations. The Black and White subsamples were separated during the multiple imputation procedure. It bears noting that since the overwhelming majority of observed variables had no missing data, very little imputation was required in either race: Indeed, save for the major discrimination constructs at waves 1 and 2 – for which valid responses total 89% and 90% of cases respectively among Blacks, and 96% and 97% respectively among Whites – valid responses equal or exceed 94% of cases for all observed variables among Blacks and 98% among Whites. These desirably high non-missing data percentages prevail in each race because of the restrictive analytical sample selection criteria referenced earlier. [I.e., respondents needed to have completed both the phone and self-administered surveys at both waves.] The data files generated using LISREL8.8-PRELIS’multiple imputation facility, which comprised small percentages of imputed values for some cases, were then utilized in the ensuing measurement and structural analyses. [Thus the measurement and structural models were estimated with complete data from all Black and White subsample members.]
We constructed measurement models to create latent variable “factor” scores for our multi-item constructs: psychological distress at waves one and two, and mastery, emotional support, chronic financial stress, chronic ill-health, and SES at wave one. Factor scores generated from measurement models by LISREL8.8 are reliable single-indicator equivalents of their multi-item counterparts (Jöreskog 2000). Table 1 displays completely standardized factor loadings for indicators of latent constructs, and descriptive statistics for all analyzed items.
Loadings in Table 1 are from a baseline multi-population measurement model in which loadings, error terms, and error covariances for corresponding indicators across waves are freed to differ across races. Tests for factorial invariance involved a) constraining loadings of items tapping specific constructs to be equal across races (i.e., collectively “fixing” them), b) comparing the Chi-square for each alternate model to the Chi-square from the baseline model with all loadings freed, and c) assessing the non-/significance of each Chi-square difference given the applicable degrees freedom. These tests pointed to substantial invariance in measurement of latent constructs across races. Because comparisons of coefficients involving latent constructs are acceptable where even partial measurement invariance obtains and only some loadings are statistically similar across groups (Reise, Widaman, and Pugh 1993), such comparisons across the Black and White subsamples in this investigation are permissible.
In the structural phases of the analysis, we utilized the latent variable “factor” scores generated at the measurement phase to represent all multi-item latent factors. Given the relative smallness of the Black sample, factor score usage allows us to preserve statistical power and avoid spreading the data too thinly across cases. As latent variable score versions of single-item constructs may be unreliable, we utilized original rather than latent variable score versions of single-item constructs throughout the analysis. Thus estimates involving the major and everyday discrimination constructs, for example, reflect the originally observed items rather than the latent variable score counterparts that LISREL also generated at the measurement phase.
The structural phase also features use of change score (“^”) versions of focal independent variables. These scores are obtained by subtracting wave one constructs from their wave 2 counterparts (e.g., ^distress = distress at wave two minus wave one distress). Both Allison (1990) and Finkel (1995) advocate the use of change scores in regression. Using the change in X on the right-hand-side (r.h.s.) of prediction equations avoids the potential collinearity problem entailed by having X1 and X2 in the same equation. It has the added interpretation advantage of its coefficient indicating the effect of a change in X on Y. Using also the lagged dependent variable on the r.h.s. is advised whenever there is theoretical support for a causal effect from lagged to subsequent incarnations of Y (Allison 1990; Finkel 1995). We contend that both perceptions of discrimination and distress are likely to influence subsequent incarnations of the same variable. As suggested earlier for example, individuals perceiving discrimination at a given point are probably more alert to the possibility of discrimination subsequently. Such vigilance should then increase the probability of discrimination being perceived at later points. The lethargy and downcast view of circumstances that are germane to distressed states at specific points, likely impair coping resources while simultaneously enhancing problem behavior involvement (e.g., alcohol abuse). Distress at later points thus becomes likelier.
Figure 1 depicts the model’s structural component in abridged form. All constructs are enclosed in squares, since our utilization of latent factor scores results in LISREL treating all constructs at the structural phase as single-indicator observed variables. [Had the structural portion been based on a full information model rather than one utilizing factor scores, then the eight latent variables described at the earlier measurement phase would have been enclosed in circles, as-per convention]. Thick arrows are utilized to minimize clutter, and signal effects of the same bracketed cluster of constructs on identical outcomes or bracketed clusters of outcomes. Thus the thick arrow emitting from control variables to the perceived discrimination outcomes, for example, represents twelve estimated paths: i.e., effects of each control variable on each discrimination outcome. Thin arrows depict effects of single predictors on outcomes.
Figure 1.
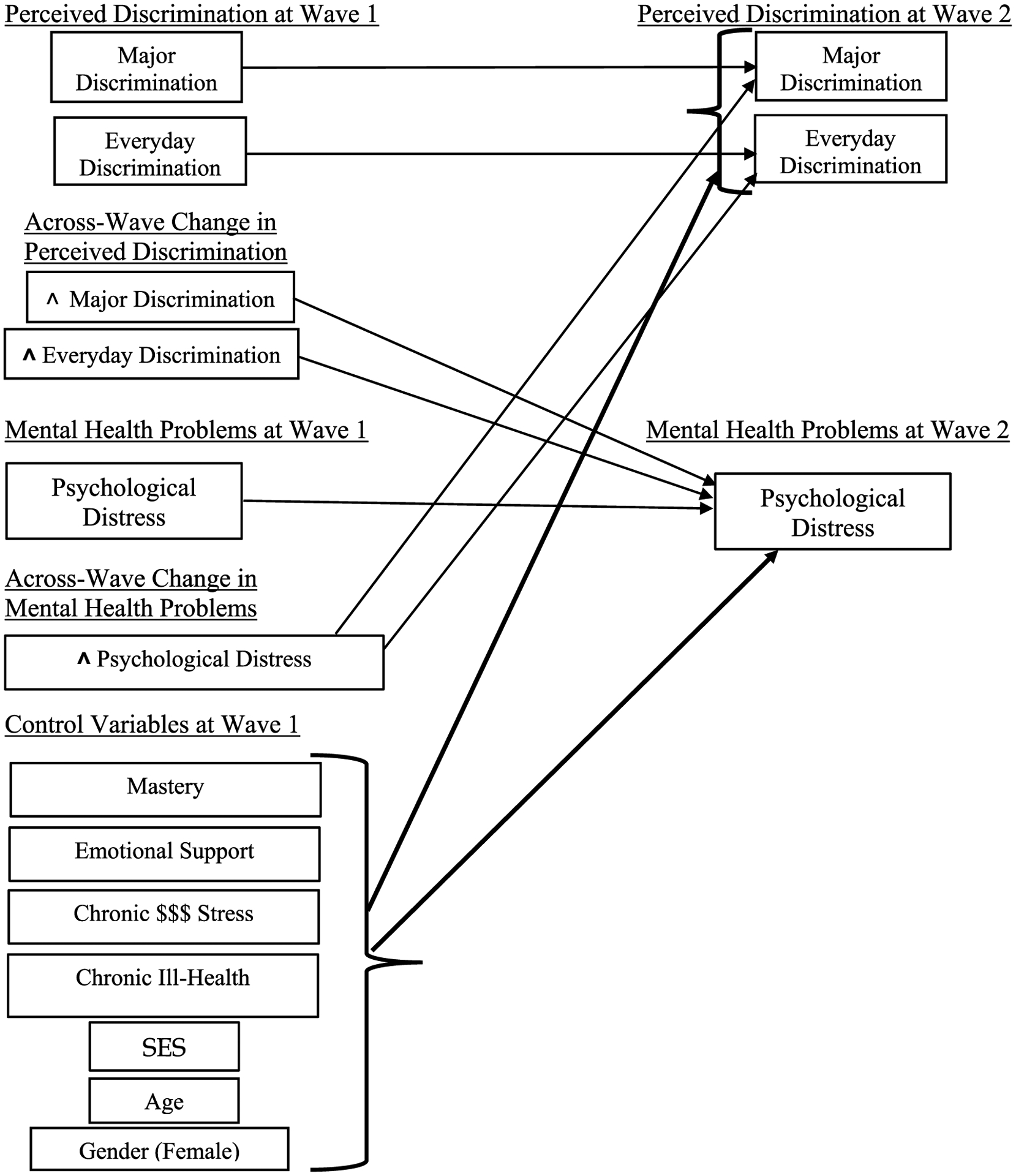
Depiction of the structural portion of the LISREL model predicting perceived discrimination and distress outcomes.
aThicker arrows (“→”) represent multiple structural paths emitting from/to variables within clusters enclosed in brackets; and thinner (“→”) arrows signal single paths.
To assess Black-White variation in the impact of the perceived discrimination and distress constructs on each other, we estimate separate pairs of multi-population models. The impact of each predictor is alternately “freed” (i.e., specified as different) and “fixed” (constrained to be equal) across groups. Significance of the Black-White difference in the impact of a predictor is signaled by a model Chi-square differential that meets the .05 two-tailed test threshold of 3.84 for one degree of freedom. Baseline models in these tests are ones with error variances of dependent variables and effects of all predictors freed across races. Coefficients in Figure 2 are from those baseline models.
Figure 2.
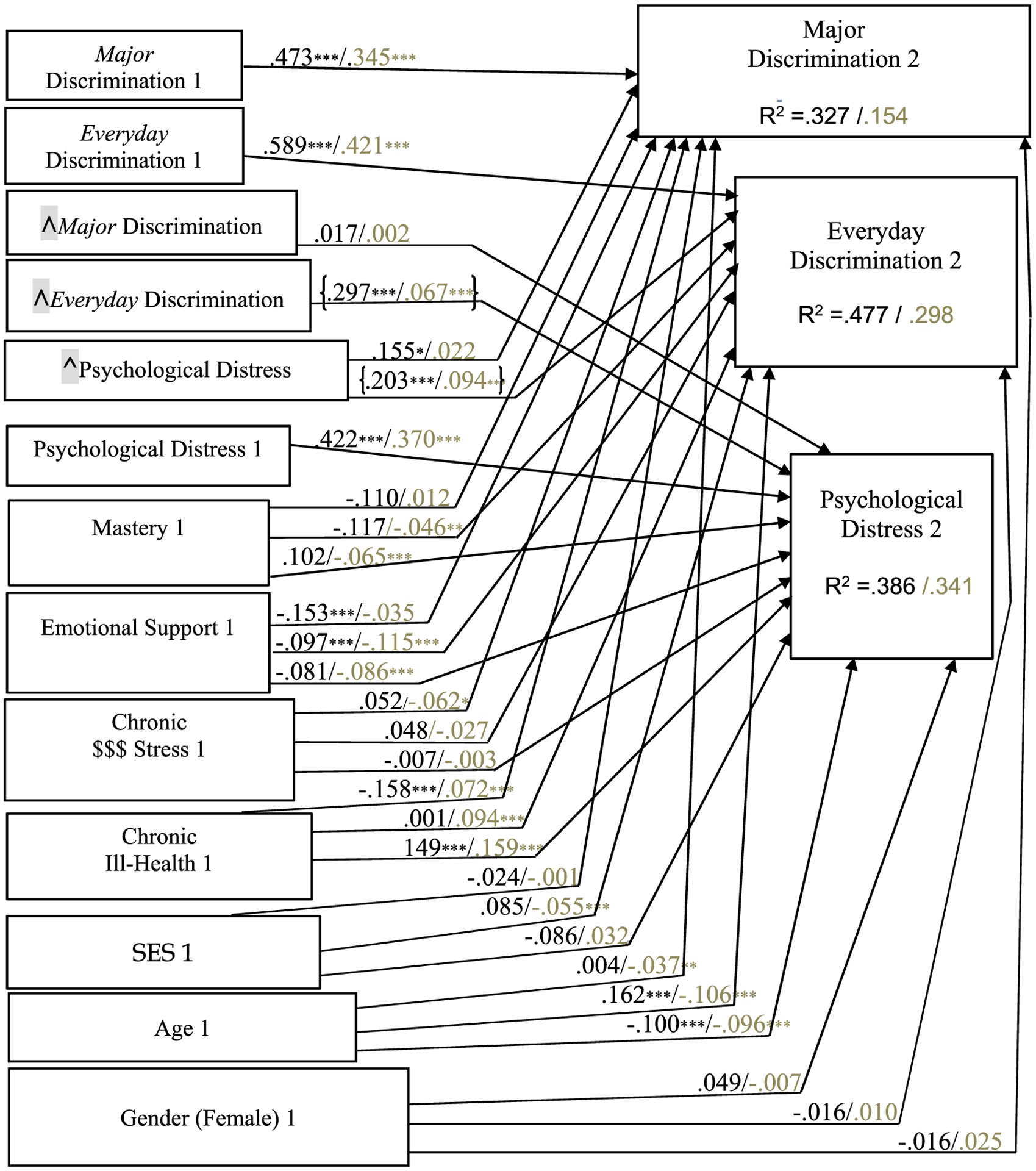
Fully standardized coefficients (darker font = Blacks/lighter font = Whites) from the structural segment of the LISREL model: MIDUS Wave 1 (1995–6) and Wave 2 (2004–6) data. N = 3561 Whites/163 Blacks. * p < .05; **p < .01; *** p < .001. Effects of focal predictors differing significantly across races are bracketed.
Assessing Adequacy of the Black Subsample
As noted earlier, we conducted two sets of preliminary analyses to address possible apprehension regarding the representativeness of the MIDUS-based Black panel utilized here. The first set involved comparing key attributes of the Black subsample with those of the 3,570 African-Americans in National Survey of American Life (NSAL) cross-sectional survey conducted between 2001 and 2003 – in-between the 1995–‘96 and 2004–‘06 MIDUS1 and MIDUS2 collection points. African-Americans in the NSAL represent a uniquely large, “nationally representative sample of African-Americans” (Jackson et al. 2004: 199). As Table 2 details, the six attributes on which our Black subsample and NSAL African-Americans were compared are the main independent and dependent constructs (major and everyday discrimination, and distress), two constructs closely related to distress (Major Depressive and Generalized Anxiety disorders), and one sociodemographic attribute (education).
Table 2.
Key attributes of the analyzed MIDUS-based Black/African-American panel (n = 163, data collection periods = 1995–‘96 and 2004–‘06), versus African-Americans in the NSAL (n = 3570, data collection period = 2001–‘03).
| MIDUS Black/African-American Panel | NSAL African-American Subsample | |
|---|---|---|
| Major Discrimination: The average of 9 indicators common across both datasets tapping lifetime exposure - one or more experiences coded 1 for each item | 3.06 (wave 1) 3.03 (wave 2) |
1.33 |
| Everyday Discrimination: The average across 9 common Likert-scaled items. Response options in the NSAL are the same ones utilized for this comparison: 1 = never, 2 = rarely, 3 = sometimes, and 4 = often. Six response options accompany the original MIDUS items: 1 = never, 2 = < once annually, 3 = a few times annually, 4 = a few times monthly, 5 = once or > weekly, and 6 = ~ every day. To facilitate the present comparison, categories 3&4 are collapsed into option number “3” and treated as equivalent to the NSAL items’ “3 = sometimes” category; and 5 & 6 are collapsed into an option “4” that is treated as = to the NSAL items’ “4 = often” | 2.12 (wave 1) 1.95 (wave 2) |
1.83 |
| Distress: The average across the 6 identically worded and Likert-scaled items appearing in both datasets querying symptoms in the preceding 30 days, i.e., how often R felt … “sad,” “nervous,” “restless,” “hopeless,” “everything was an effort,” and “worthless.” Response options: 1 = none of the time … 5 = all the time | 1.55 (wave 1) 1.66 (wave 2) |
1.64 |
| MDD: % experiencing this disorder in preceding year (using MIDUS/NSAL personnel-constructed dichotomous indicators) | 9.8% (wave 1) 9.8% (wave 2) |
6.6% |
| GAD: % experiencing this disorder in preceding year (using MIDUS/NSAL personnel-constructed dichotomous indicators) | 3.1% (wave 1) 3.1% (wave 2) |
2.5% |
| Average Education Level: 12 response options accompany the MIDUS measures: =1 no school/some grade school, 2 = eighth grade/junior high; 3 = some high school; 4 = GED; 5 = HS grad., 6 = 1–2 years of college; 7 = 3 or> years of college; 8 = 2-yr Assoc. degree/Voc. school diploma; 9 = BA; 10 = some grad school; 11 = MA; 12 = Ph.D., MD, etc. In the NSAL, education = actual years of schooling (17 = 17 or >) | 6.33 (wave 1) * Roughly equal to ~13 years 6.61 (wave 2) * Roughly equal to ~14 years |
12.32 |
Findings in Table 2 indicate substantial similarity between our MIDUS-derived Black panel and African-Americans in the NSAL. For four of the six examined constructs – average education levels, and exposure to everyday discrimination, distress, and GAD – patterns across the datasets are either virtually identical, or differences are slight. Differences seem larger in the case of a) major discrimination exposure, where Blacks at each MIDUS wave report more than twice as many experiences on average vis-a-vis NSAL African-Americans (i.e., 3.06 and 3.03 of 9 assessed forms vs. 1.33), and b) MDD, where the 12 month prevalence rate among Blacks at each MIDUS wave is one-third higher than that of African-Americans in the NSAL (9.8% versus 6.6%). Even for these constructs however, differences across datasets in the estimated prevalence of referenced phenomena seem far from considerable. Thus to reiterate, patterns in Table 2 suggest considerable similarity between the MIDUS-derived panel of Blacks analyzed here, and the uniquely large NSAL-derived sample that is representative of the African-American population during the specified period (Jackson et al. 2004).
The second set of preliminary analyses involved computing correlations between race and analyzed variables in a sample that combines the Black and White panels (Blacks coded 1, Whites 0), and assessing the level of congruence between obtained correlations and previously reported patterns.2 Inasmuch as such congruence signals that Blacks in MIDUS differ from, or are similar to Whites in ways replicating “known” (i.e., previously observed) patterns, confidence in the representativeness of the Black subsample should be enhanced. Substantial congruence prevails: Consistent with previous patterns, distress levels are statistically similar across races at each wave; and Blacks at each wave perceive significantly more major and everyday discrimination (Keyes 2009; Lee and Turney 2012; Maryl and Saperstein 2013; Williams 2018). Among control variables, levels of mastery are statistically similar across races. This replicates the pattern in the NSAL survey that Williams et al. (2012) observe. Emotional support from close family and friends is also statistically similar across races – consistent with patterns observed previously (e.g., Kiecolt, Hughes, and Keith 2008). Finally, consistent with firmly established patterns, socioeconomic status is significantly higher among Whites, and financial strain and physical ill-health higher among Blacks.
The preliminary analyses detailed above should assuage reservations that may arise regarding the representativeness of the Black subsample – given its smallness associated with the larger attrition rate across waves among Blacks relative to Whites.
Results
Estimates from the structural equation segment of the multi-population analysis are presented in Figure 2. [Table 3 lists zero-order correlations, separated by race, among all variables included in this same structural equation segment.] The fully standardized coefficients in Figure 2 facilitate direct comparisons of structural relationships between specific predictors and outcomes. Each arrow represents a relationship or “path” that is estimated, with coefficients for Blacks listed alongside coefficients for Whites (in lighter font). {Brackets} enclose coefficients involving perceived discrimination or distress predictor constructs that differ significantly across races. Significance tests for differences across races involving non-focal predictor constructs were not conducted, given their secondary theoretical importance.
Table 3.
Correlations among variables in the structural segment of the model, separated by race. MIDUS Wave 1 (1995–6) and Wave 2 (2004–6) data.
| Blacks | MAJORD2 | EVRYDAY2 | DISTRES2 | AGE1 | FEMALE1 | MAJORD1 |
|---|---|---|---|---|---|---|
| MAJORD2 | 1.000 | |||||
| EVRYDAY2 | 0.195 | 1.000 | ||||
| DISTRES2 | 0.016 | 0.034 | 1.000 | |||
| AGE1 | −0.026 | −0.238 | −0.233 | 1.000 | ||
| FEMALE1 | −0.135 | −0.108 | 0.079 | −0.076 | 1.000 | |
| MAJORD1 | 0.511 | 0.282 | 0.005 | 0.023 | −0.126 | 1.000 |
| EVRYDAY1 | 0.192 | 0.624 | −0.031 | −0.097 | −0.112 | 0.379 |
| SES1 | 0.158 | 0.169 | −0.177 | −0.067 | −0.236 | 0.371 |
| ^MAJORD | −0.284 | −0.120 | 0.066 | −0.040 | 0.023 | −0.666 |
| ^EVRYDAY | 0.038 | −0.160 | 0.326 | −0.166 | 0.003 | −0.041 |
| ^DISTRES | 0.092 | 0.015 | −0.157 | −0.011 | −0.115 | −0.023 |
| CHRONIL1 | −0.094 | 0.042 | 0.265 | 0.109 | 0.282 | −0.010 |
| $STRESS1 | 0.088 | 0.132 | 0.279 | −0.201 | 0.182 | 0.083 |
| EMOTSUP1 | −0.265 | −0.336 | −0.289 | 0.174 | 0.132 | −0.241 |
| DISTRES1 | 0.044 | 0.110 | 0.499 | −0.200 | 0.180 | 0.104 |
| MASTERY1 | −0.115 | −0.101 | −0.174 | −0.119 | −0.076 | −0.051 |
| Blacks | EVRYDAY1 | SES1 | ^MAJORD | ^EVRYDAY | ^DISTRES | CHRONIL1 |
| EVRYDAY1 | 1.000 | |||||
| SES1 | 0.209 | 1.000 | ||||
| ^ MAJORD | −0.221 | −0.231 | 1.000 | |||
| ^EVRYDAY | −0.419 | −0.043 | 0.247 | 1.000 | ||
| ^DISTRES | −0.226 | 0.024 | 0.138 | 0.276 | 1.000 | |
| CHRONIL1 | 0.073 | −0.355 | −0.073 | −0.034 | −0.104 | 1.000 |
| $STRESS1 | 0.108 | −0.328 | −0.042 | 0.030 | −0.199 | 0.323 |
| EMOTSUP1 | −0.325 | 0.010 | 0.047 | −0.018 | 0.201 | −0.183 |
| DISTRES1 | 0.168 | −0.183 | −0.072 | 0.030 | −0.575 | 0.338 |
| MASTERY1 | −0.071 | 0.352 | −0.020 | −0.036 | 0.266 | −0.329 |
| Blacks | $STRESS1 | EMOTSUP1 | DISTRES1 | MASTERY1 | ||
| $STRESS1 | 1.000 | |||||
| EMOTSUP1 | −0.328 | 1.000 | ||||
| DISTRES1 | 0.442 | −0.452 | 1.000 | |||
| MASTERY1 | −0.223 | 0.361 | −0.411 | 1.000 | ||
| Whites | MAJORD2 | EVRYDAY2 | DISTRES2 | AGE1 | FEMALE1 | MAJORD1 |
| MAJORD2 | 1.000 | |||||
| EVRYDAY2 | 0.099 | 1.000 | ||||
| DISTRES2 | 0.084 | 0.153 | 1.000 | |||
| AGE1 | −0.065 | −0.166 | −0.130 | 1.000 | ||
| FEMALE1 | 0.059 | 0.034 | 0.034 | −0.015 | 1.000 | |
| MAJORD1 | 0.371 | 0.162 | 0.080 | −0.043 | 0.067 | 1.000 |
| EVRYDAY1 | 0.146 | 0.495 | 0.135 | −0.147 | 0.019 | 0.308 |
| SES1 | −0.055 | −0.125 | −0.167 | −0.102 | −0.157 | −0.004 |
| ^MAJORD | −0.163 | −0.009 | 0.017 | −0.033 | −0.002 | −0.483 |
| ^EVRYDAY | −0.022 | −0.183 | 0.076 | −0.022 | 0.016 | −0.076 |
| ^DISTRES | 0.013 | 0.079 | −0.144 | −0.034 | 0.004 | −0.003 |
| CHRONIL1 | 0.137 | 0.208 | 0.404 | 0.110 | 0.151 | 0.125 |
| $STRESS1 | 0.153 | 0.191 | 0.286 | −0.228 | 0.055 | 0.156 |
| EMOTSUP1 | −0.118 | −0.293 | −0.328 | 0.168 | 0.097 | −0.143 |
| DISTRES1 | 0.111 | 0.202 | 0.544 | −0.115 | 0.035 | 0.125 |
| MASTERY1 | −0.078 | −0.201 | −0.397 | −0.049 | −0.076 | −0.069 |
| Whites | EVRYDAY1 | SES1 | ^ MAJORD | ^EVRYDAY | ^DISTRES | CHRONIL1 |
| EVRYDAY1 | 1.000 | |||||
| SES1 | −0.080 | 1.000 | ||||
| ^MAJORD | −0.041 | −0.046 | 1.000 | |||
| EVRYDAY | −0.478 | −0.047 | 0.131 | 1.000 | ||
| ^DISTRES | −0.009 | −0.033 | 0.020 | 0.090 | 1.000 | |
| CHRONIL1 | 0.165 | −0.389 | 0.017 | 0.049 | −0.053 | 1.000 |
| $STRESS1 | 0.219 | −0.459 | 0.014 | −0.022 | −0.074 | 0.334 |
| EMOTSUP1 | −0.312 | 0.042 | 0.007 | 0.012 | 0.058 | −0.238 |
| DISTRES1 | 0.231 | −0.158 | −0.001 | −0.006 | −0.356 | 0.523 |
| MASTERY1 | −0.192 | 0.301 | −0.012 | −0.018 | 0.142 | −0.442 |
| Whites | $STRESS1 | EMOTSUP1 | DISTRES1 | MASTERY1 | ||
| $STRESS1 | 1.000 | |||||
| EMOTSUP1 | −0.294 | 1.000 | ||||
| DISTRES1 | 0.407 | −0.440 | 1.000 | |||
| MASTERY1 | −0.382 | 0.389 | −0.606 | 1.000 |
Variable name key: MAJORD1/2 = Major Discrimination at wave 1/2; EVRYDAY1/2 = Everyday Discrimination at wave 1/2; DISTRES1/2 = Psychological Distress at wave 1/2; ^MAJORD = Change in Major Discrimination across waves; ^EVRYDAY = Change in Everyday Discrimination across waves; ^DISTRES = Change in Psychological Distress across waves; SES1 = SES at wave 1; CHRONIL1 = Chronic Ill Health at wave 1; $STRESS1 = Chronic $ $ Stress at wave 1; EMOTSUP1 = Emotional Support at wave 1; MASTERY1 = Mastery @ wave 1; AGE1 = Age at wave 1; FEMALE1 = Gender (Female = 1) at wave 1.
Findings in Figure 2 yield substantial-if-not-comprehensive support for the hypotheses anticipating reciprocity between perceived discrimination and psychological distress, and more pronounced reciprocity among Blacks. [As used here, “reciprocity” denotes positive effects of perceived discrimination dimensions and distress on each other]. Evidence of such reciprocity is restricted to the relationship between perceived everyday discrimination and distress in each race. Perceived major discrimination does not significantly influence distress in either race; and the reciprocal impact of distress on major discrimination is significant among Blacks only. Importantly, there are no signs in either race of perceived discrimination inhibiting distress over time, or of distress suppressing perceived discrimination. Among Blacks, elevated exposure to perceived everyday discrimination across waves is associated with more distress at wave two (.297⋆⋆); and elevated distress across waves is positively associated with perceived everyday discrimination at wave two (.203⋆⋆). These two coefficients significantly exceed the also positive corresponding coefficients among Whites (i.e., .067⋆⋆⋆ and .094⋆⋆⋆). Significance of these Black-White differentials is signaled by enclosure of both pairs of coefficients in brackets. The paths among Whites are deemed less pronounced than their counterparts among Blacks based on the criterion outlined previously: Differences between Chi-square values for the alternate models with each path “fixed” versus “freed” across races each exceed the .05 significance threshold of 3.84 for a two-tailed test.
The significant Black-White differentials in effects of everyday discrimination and distress on each other comport with the thesis of stronger reciprocity between discrimination and mental health problems among Blacks: Increased perceived exposure to everyday discrimination across waves aligns with distress among Blacks primarily. Predominantly among Blacks as well, increased distress is associated with perceived encounters with everyday discrimination. Additionally, appertaining two competing theses cited earlier – i.e., of Blacks having greater “psychological immunity” from discrimination, versus being more adversely affected by this stressor – the Black-White difference in the impact of everyday discrimination evidently supports the latter thesis and not the former.
Patterns in Figure 2 are unaffected by two adjustments to the model: 1) addition of paths from each dimension of discrimination at wave one to the other dimension at wave two; and as noted earlier 2) operationalizing emotional support as four constructs versus one in equations predicting the perceived discrimination and distress outcomes (i.e., positive/negative support from close family/friends).
Discussion
We gauged variation among Black and White Americans in the reciprocal relationship between perceived major and everyday discrimination, and the mental health problem of psychological distress. Two hypotheses informed by prior theoretical and empirical contributions evolved from this exploration of “multidirectionality” (Pearlin et al. 1981): positive effects of perceived discrimination and distress constructs on each other across time, and more pronounced signs of such reciprocity among Blacks. Both hypotheses are supported for relationships between everyday discrimination and distress. No reciprocity prevails between major discrimination and distress in either race. The stronger connection in both races between perceived everyday versus major discrimination and distress comports with patterns reported in several prior studies (e.g., Lee and Turney 2012; Mossakowski 2003; Williams et al. 2012).
As signaled by their fitting moniker, indignities constituting everyday discrimination typically have a more recurrent and accumulative quality than major discrimination encounters. The latter are usually episodic and discrete (Lee and Turney 2012; Williams et al. 1997). Everyday discrimination encounters thus seem likelier than major ones to be salient or “fresh” in individuals’ minds at given time-points. They may thus be more readily accessible to exert influence upon, or be influenced by, mental health status. Congruently, Williams et al. (1997: 349) suggest that persistent, repeated chronic stressors bear more adversely upon health than sporadic and time-limited ones.
The reciprocity observed here between everyday discrimination and psychological distress, is construable as a distinctive “chain” of adversity (Pearlin et al. 2005) besetting Black and White Americans. Encounters with everyday discrimination and distress are revealed here to be problematic in part because these adversities reinforce each other over time. Thus, experiencing the adversity of elevated everyday discrimination enhances proneness over time to the adversity of more distress; and confronting the adversity of elevated distress enhances exposure to the adversity of more everyday discrimination. If we may interpret this everyday discrimination-psychological distress adversarial chain using “Matthew effect”-associated parlance (Merton 1968), the pronounced disadvantage associated with experiencing relatively high everyday discrimination or distress prevails substantially because the stress of everyday discrimination and mental health problem of distress reinforce each other over time.
Effects of perceived everyday discrimination on distress in both races comport with the earlier-noted potential for stress to induce feelings such as loss, strain and ambiguity, to erode individuals’ self-assessed ability to head off unwanted events, and dampen their inclination to press forward despite adversity (Brown, Williams, and Jackson et al. 2000; Pearlin et al. 1981). Problematic emotions such as these are salient features of distress. The reciprocal effect of distress on perceived everyday discrimination in each race, and on perceived major discrimination among Blacks, may reflect either of the potentially relevant processes outlined earlier: 1) Better mental health probably fosters relatively upbeat interpretations of others’ motives (Phinney, Madden, and Santos 1998). Perhaps more consequentially, 2) given similar socio-environmental constraints, emotional health likely “arms” individuals with the psychological wherewithal to forestall unfair treatment or halt it swiftly after it starts. The latter process is likely intertwined with the self’s capacity as a social force shaping individuals’ experiences (Rosenberg 1990), and the related notion of emotionally healthier persons selecting themselves out of problematic circumstances and interpersonal encounters (Thoits 2006).
The greater apparent intensity among Blacks of the perceived everyday discrimination-psychological distress adversarial chain is also of nontrivial theoretical significance. For one thing, the pattern substantiates the earlier-referenced presumption that subordinate groups’ well-being is inordinately undermined by the cumulative disadvantage process (DiPrete and Eirich 2006; Pearlin et al. 2005). More so among Blacks than among Whites, similar increases in exposure to everyday discrimination translate into greater distress; and similar increases in distress redound to greater exposure to everyday discrimination. Furthermore, the stronger association between everyday discrimination and Blacks’ distress evidently supports the thesis that Blacks are more disadvantaged by discrimination than Whites, rather than being more psychologically immune to its effects (Kessler, Mickelson, and Williams 1999). As to why everyday discrimination appears more damaging to Blacks’ emotional health than Whites,’ it may simply be that day-to-day discrimination facing Blacks is more severe. Supplementary analyses that we conducted revealed that among Blacks especially, elevated exposure to everyday discrimination across waves is associated with anxiety and depression levels that exceed thresholds for Generalized Anxiety and Major Depressive Disorders.3 [These supplementary analyses also indicated similarity in GAD and MDD levels across races]. An elevated propensity among Blacks for perceived everyday discrimination to foster clinically significant anxiety and depression may be construed as a self-authenticating signal of the greater severity of the discrimination confronting Blacks vis-à-vis Whites. Furthermore, any greater propensity for everyday discrimination to trigger MDD particularly among Blacks is even more consequential given what is known about Blacks’ depression: Once clinical thresholds are reached, Blacks’ depression is likelier than Whites’ to be more persistent and severe, to involve greater impairment, and to go untreated (Williams 2018).
If everyday discrimination confronting Blacks is indeed more severe than that besetting Whites, odds of this stressor being experienced as such by Blacks are also seemingly enhanced. As detailed earlier, conflicting propositions regarding which group is likelier to experience discrimination as stressful are derivable from two elements of the ideology sustaining whiteness that seem especially relevant here (Malat, Mayorga-Gallo, and Williams 2018): 1) anticipation by Whites of socioeconomic success relative to Blacks especially – from which the presumption that Whites are likelier than Blacks to experience discrimination as a stressor is derivable, and 2) explanations for inequality that elevate values- and habit-related traits of individuals over structural factors – from which the presumption that Blacks are likelier to experience discrimination as a stressor is derivable. With respect to everyday discrimination at least, our findings evidently concur more with the idea of discrimination being experienced as a stressor by Blacks especially. Insofar as disadvantaging of blackness and advantaging of whiteness remains a priority animating American social life (Bonilla-Silva 1996; Malat, Mayorga-Gallo, and Williams 2018), the notion that everyday discrimination confronting Blacks is more pernicious than that facing Whites resonates all the more. The more pronounced association of elevated distress with perceived everyday discrimination among Blacks comports with the thesis proffered earlier that Blacks in poor mental health may be uniquely exposed targets for discrimination. A stronger pre-disposition toward perceiving discrimination among distressed Blacks – induced by especially intricate familiarity with disadvantages tied to discrimination and poor mental health – might also be contributing to the above pattern. As noted earlier, prior encounters with discrimination foster “vigilance” (Meyer 2003; Pearlin et al. 2005; Williams 2018), thereby enhancing odds of individuals defining subsequent discriminatory encounters as such.
The inordinate strength among backs of the everyday discrimination-psychological distress adversarial chain, it also bears mentioning, is not irreconcilable with tendency observed here and in prior studies for Blacks to exhibit similar rather than greater distress and psychiatric disorder levels vis-à-vis Whites. Our findings leave viable the proposition that Blacks’ aggregate-level distress and disorder levels might even trail Whites’ if Blacks were not more strongly enmeshed in the adversarial chain encompassing positive effects of perceived everyday discrimination and distress on each other across time. As referenced earlier, aggregate-level Black-White stress exposure differentials substantially inspire the “flourishing” hypothesis (Keyes 2009) – which emphasizes the tendency for Blacks to be no more prone to psychiatric disorders than Whites, notwithstanding Blacks’ greater exposure to race-related stressors such as discrimination.
Limitations
We again acknowledge the relative smallness of the analyzed Black subsample as a limitation. While Ns of 163 are not uniformly labeled “small,” the dwarfing by the size of our White subsample is significantly short of ideal. On the other hand, confidence in the representativeness of our Black subsample is enhanced by a high congruence between observed patterns and ones reported previously, and by comparisons with Black responses in the NSAL. It should also be noted that the autoregressive or “cross-lagged” approach to statistical modeling employed here is not an absolute panacea for ascertaining causal effects. We have shown that elevated perceived exposure to everyday discrimination over time redounds to greater current psychological distress, and elevated psychological distress redounds to greater perceived everyday discrimination within both races. Wave one counterparts of the endogenous variables (i.e., distress and perceived discrimination) are key statistical controls in these cross-lagged models. Their inclusion eliminates the possibility that even more antecedent versions of the given endogenous variable impact both the focus predictor and the current endogenous measure. However, it is not possible to rule out the driving force of some other time-varying factor that is causally antecedent to both focus and response. Only a randomized trial could solve this dilemma.
Conclusion
Future investigations may seek to probe more systematically the intriguing question of why Blacks appear no more prone to severe mental health problems than Whites despite greater exposure to multiple stressors, and the main pattern we have uncovered here: stronger embeddedness among Blacks in the adversarial chain embodying positive effects of perceived everyday discrimination and distress on each other across time. Assessment of a broad array of stress and emotional well-being or coping constructs will likely facilitate insightful cues. This expanded array might include, for example, areas of stress exposure where Whites are disadvantaged, and coping resources that Blacks and other minority groups have greater access to. Studies pursuing these research questions should ideally, like this investigation, utilize longitudinal models. A major strength of these models is the statistical controlling for baseline-levels of focal constructs and relatively effective temporal sequencing of outcomes from predictors that they facilitate. Collection of data that would enable reanalysis of the present research questions with a Black subsample substantially larger than the one utilized here would also obviously be welcome. The smallness of the analyzed Black subsample is acknowledged as a limitation of this investigation – even though confidence in its main findings is enhanced by high congruence between observed patterns and ones reported previously, and by earlier-detailed preliminary analyses that substantiate the Black subsample’s representativeness.
Notes on contributors
Gary Oates is associate professor of sociology at Bowling Green State University. His research is motivated by interest in the reciprocal relationship between social structural variables, and individuals’ orientations and traits that bear upon social problems. Race and race-related factors are the main structural variables addressed in his work.
Alfred DeMaris is emeritus professor of sociology at Bowling Green State University and statistical consultant for the department’s Center for Family and Demographic Research. His substantive interests are in heterosexual intimate relationships. His statistical concentration is on causal inference in regression modeling.
Footnotes
It bears acknowledging that even if the impact of perceived discrimination on distress initiates the anticipated feedback loop between both constructs among Blacks especially, such sequencing is not decipherable with the two-wave data source utilized here.
Since the latent variable scores representing each multi-item construct at the structural phase are standardized variables centered on within-race means, both races have identical means and standard deviations (0 and 1 respectively) for each latent variable score. Their utilization during this preliminary analysis was therefore unfeasible. Multi-item indexes used in this phase are thus averages of constituent indicators, with relevant “positively” or “negatively” worded items reverse-coded prior to computation.
Continuous constructs created by MIDUS personnel that tap GAD and MDD exposure are utilized in these analyses. Zero signals the absence of the referenced disorder at a survey wave. Non-zero values signal the likely presence, with higher values indicating greater severity. These disorder constructs reflect criteria specified in the Diagnostic and Statistical Manual of Disorders, Third Edition-Revised (DSM-III-R) (ICPSR 2007: 11–15).
Disclosure Statement
No potential conflict of interest was reported by the authors.
References
- Allison PD 1990. “Change Scores as Dependent Variables in Regression Analysis.” Sociological Methodology 20:93–114. doi: 10.2307/271083. [DOI] [Google Scholar]
- Aneshensel CS 2015. “Sociological Inquiry into Mental Health: The Legacy of Leonard I. Pearlin.” Journal of Health and Social Behavior 56:166–78. doi: 10.1177/0022146515583992. [DOI] [PubMed] [Google Scholar]
- Bonilla-Silva E 1996. “Rethinking Racism: Toward a Structural Interpretation.” American Sociological Review 62:465–80. doi: 10.2307/2657316. [DOI] [Google Scholar]
- Brody GH, Chen Y, Murry VM, and Cutrona CE. 2006. “Perceived Discrimination and the Adjustment of African American Youths: A Five-Year Longitudinal Analysis with Contextual Moderation Effects.” Child Development 77:1170–89. doi: 10.1111/j.1467-8624.2006.00927.x. [DOI] [PubMed] [Google Scholar]
- Brown TN, Williams DR, Jackson JS, Neighbors HW, Torres M, Sellers SL, and Brown KT. 2000. “Being Black and Feeling Blue: The Mental Health Consequences of Racial Discrimination.” Race and Society 2:117–31. doi: 10.1016/S1090-9524(00)00010-3. [DOI] [Google Scholar]
- DiPrete Thomas A. and Eirich GM. 2006. “Cumulative Advantage as A Mechanism for Inequality: A Review of Theoretical and Empirical Developments.” Annual Review of Sociology 32:271–97. doi: 10.1146/annurev.soc.32.061604.123127. [DOI] [Google Scholar]
- Ellison C, Musick MA, and Henderson AK. 2008. “Balm in Gilead: Racism, Religious Involvement, and Psychological Distress among African-American Adults.” Journal for the Scientific Study of Religion 47:291–309. doi: 10.1111/j.1468-5906.2008.00408.x. [DOI] [Google Scholar]
- Finkel SE 1995. Causal Analysis with Panel Data. Thousand Oaks, CA: Sage. [Google Scholar]
- Gee G and Walsemann K. 2009. “Does Health Predict the Reporting of Racial Discrimination or Do Reports of Discrimination Predict Health? Findings from the National Longitudinal Study of Youth.” Social Science and Medicine 68:1676–84. doi: 10.1016/j.socscimed.2009.02.002. [DOI] [PubMed] [Google Scholar]
- ICPSR. 2007. “ICPSR 2760: National Survey of Midlife Development in the United States 1995–1996. Index of Scales and Constructed Scales in MIDUS 1.” Ann Arbor, MI: Inter-university Consortium for Political and Social Research. www.icpsr.umich.edu. [Google Scholar]
- Jackson JS, Knight KM, and Rafferty JA. 2010. “Race and Unhealthy Behaviors: Chronic Stress, the HPA Axis, and Physical and Mental Health Disparities over the Life Course.” American Journal of Public Health 100:933–39. doi: 10.2105/AJPH.2008.143446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson JS, Torres M, Caldwell CH, Neighbors HW, Nesse RM, Taylor RJ, Trierweiler SJ, Williams DR. 2004. “The National Survey of American Life: A Study of Racial, Ethnic and Cultural Influences on Mental Disorders and Mental Health.” International Journal of Methods in Psychiatric Research 4:196–207. doi: 10.1002/mpr.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jöreskog K 2000. “Variable Scores and Their Uses.” (https://ssicentral.com/wp-content/uploads/2020/07/lis_lvscores.pdf).
- Jöreskog K and Sörbom D. 2003. LISREL8:5 for Windows [Computer Software]. Lincolnwood, IL: Scientific Software International, Inc. [Google Scholar]
- Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand S-LT, Walters EE, and Zaslavsky AM. 2002. “Short Screening Scales to Monitor Population Prevalences and Trends in Non-Specific Psychological Distress.” Psychological Medicine 32:959–76. doi: 10.1017/S0033291702006074. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Mickelson KD, and Williams DR. 1999. “The Prevalence, Distribution and Mental Health Correlates of Perceived Discrimination in the United States.” Journal of Health and Social Behavior 40:208–30. doi: 10.2307/2676349. [DOI] [PubMed] [Google Scholar]
- Keyes CLM 2009. “The Black–White Paradox in Health: Flourishing in the Face of Social Inequality and Discrimination.” Journal of Personality 77:1678–705. doi: 10.1111/j.1467-6494.2009.00597.x. [DOI] [PubMed] [Google Scholar]
- Kiecolt JK, Hughes M, and Keith VM. 2008. “Race, Social Relationships, and Mental Health.” Personal Relationship 15:229–45. doi: 10.1111/j.1475-6811.2008.00195.x. [DOI] [Google Scholar]
- Lee H and Turney K. 2012. “Investigating the Relationship between Perceived Discrimination, Social Status, and Mental Health.” Society and Mental Health 2:1–20. doi: 10.1177/2156869311433067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malat JA, Mayorga-Gallo S, and Williams DR. 2018. “The Effects of Whiteness on the Health of Whites in the USA.” Social Science and Medicine 199:148–56. doi: 10.1016/j.socscimed.2017.06.034. [DOI] [PubMed] [Google Scholar]
- Maryl D and Saperstein A. 2013. “When White People Report Racial Discrimination: The Role of Region, Religion, and Politics.” Social Science Research 42:742–54. doi: 10.1016/j.ssresearch.2012.12.007. [DOI] [PubMed] [Google Scholar]
- Merton RK 1968. “The Matthew Effect in Science: The Reward and Communication System of Science.” Science 199:55–63. [PubMed] [Google Scholar]
- Meyer LH 2003. “Prejudice as Stress: Conceptual and Measurement Problems.” American Journal of Public Health 93:262–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mossakowski KN 2003. “Coping with Perceived Discrimination: Does Ethnic Identity Protect Mental Health?” Journal of Health and Social Behavior 44:318–31. doi: 10.2307/1519782. [DOI] [PubMed] [Google Scholar]
- Norton MI and Sommers S. 2011. “Whites See Racism as a Zero-Sum Game that They are Now Losing.” Perspectives on Psychological Science 6:215–18. doi: 10.1177/1745691611406922. [DOI] [PubMed] [Google Scholar]
- Pavalko EK, Mossakowski KN, and Hamilton VJ. 2003. “Does Perceived Discrimination Affect Health? Longitudinal Relationships between Work Discrimination and Women’s Physical and Emotional Health.” Journal of Health and Social Behavior 43:18–33. doi: 10.2307/1519813. [DOI] [PubMed] [Google Scholar]
- Pearlin LI 1999. “The Stress Process Revisited: Reflections on Concepts and Their Interrelationships.” Pp. 395–415 in Handbook of the Sociology of Mental Health, edited by Aneshensel CS and Phelan JC. New York: Plenum. [Google Scholar]
- Pearlin LI and Schooler C. 1978. “The Structure of Coping.” Journal of Health and Social Behavior 19:2–21. doi: 10.2307/2136319. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Menaghan EG, Lieberman MA, and Mullan JT. 1981. “The Stress Process.” Journal of Health and Social Behavior 22:337–56. doi: 10.2307/2136676. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Schieman S, Fazio EM, and Meersman S. 2005. “Stress, Health, and the Life Course: Some Conceptual Perspectives.” Journal of Health and Social Behavior 46:205–19. doi: 10.1177/002214650504600206. [DOI] [PubMed] [Google Scholar]
- Phinney JS, Madden T, and Santos L. 1998. “Psychological Variables as Predictors of Perceived Ethnic Discrimination among Minority and Immigrant Adolescents.” Journal of Applied Social Psychology 28:937–53. doi: 10.1111/j.1559-1816.1998.tb01661.x. [DOI] [Google Scholar]
- Quillian L 2006. “New Approaches to Understanding Racial Prejudice and Discrimination.” Annual Review of Sociology 32:299–328. doi: 10.1146/annurev.soc.32.061604.123132. [DOI] [Google Scholar]
- Reise SP, Widaman KF, and Pugh RH. 1993. “Confirmatory Factor Analysis and Item Response Theory: Two Approaches for Exploring Measurement Invariance.” Psychological Bulletin 114:552–66. doi: 10.1037/0033-2909.114.3.552. [DOI] [PubMed] [Google Scholar]
- Ren XS, Amick BC, and Williams DR. 1999. “Racial/Ethnic Disparities in Health: The Interplay between Discrimination and Socioeconomic Status.” Ethnicity and Health 9:151–65. [PubMed] [Google Scholar]
- Rosenberg M 1990. “The Self-Concept: Social Product and Social Force.” Pp. 593–624 in Social Psychology: Sociological Perspectives, edited by Rosenberg M and Turner RH. Piscataway, NJ: Transaction Publishers. [Google Scholar]
- Ross CE and Mirowsky J. 2003. “Social Structure and Psychological Functioning: Distress, Perceived Control, and Trust.” Pp. 411–40 in Handbook of Social Psychology, edited by Delamater J. New York, NY: Kluwer-Plenum. [Google Scholar]
- Salvatore J and Shelton N. 2007. “Cognitive Costs of Exposure to Racial Prejudice.” Psychological Science 18:810–15. doi: 10.1111/j.1467-9280.2007.01984.x. [DOI] [PubMed] [Google Scholar]
- Thoits PA 2006. “Personal Agency in the Stress Process.” Journal of Health and Social Behavior 47:309–23. doi: 10.1177/002214650604700401. [DOI] [PubMed] [Google Scholar]
- Thoits PA 2010. “Stress and Health: Major Findings and Policy Implications.” Journal of Health and Social Behavior 51:41–53. doi: 10.1177/0022146510383499. [DOI] [PubMed] [Google Scholar]
- Williams DR 2018. “Stress and the Mental Health of Populations of Color: Advancing Our Understanding of Populations of Color.” Journal of Health and Social Behavior 59:466–85. doi: 10.1177/0022146518814251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Haile R, Mohammed SA, Herman A, Sonnega J, Jackson JS, Stein DJ. 2012. “Perceived Discrimination and Psychological Well- Being in the USA and South Africa.” Ethnicity and Health 17:111–33. doi: 10.1080/13557858.2012.654770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR and Mohammed SA. 2009. “Discrimination and Racial Disparities in Health: Evidence and Needed Research.” Journal of Behavioral Medicine 32:20–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Yu Y, Jackson JS, and Anderson NB. 1997. “Racial Differences in Physical and Mental Health: Socioeconomic Status, Stress and Discrimination.” Journal of Health Psychology 2:335–51. doi: 10.1177/135910539700200305. [DOI] [PubMed] [Google Scholar]
- Yang Y 2006. “How Does Functional Disability Affect Depressive Symptoms in Late Life? The Role of Perceived Social Support and Psychological Resources.” Journal of Health and Social Behavior 47:355–72. doi: 10.1177/002214650604700404. [DOI] [PubMed] [Google Scholar]