

Abstract
Neurofibromtosis-1 (NF-1) is the commonest oculo-neuro-cutaneous syndrome with multiple ocular manifestations. Reporting three children who presented with unilateral glaucoma (buphthalmos), ipsilateral facial hemihypertrophy, and eyelid plexiform neurofibroma: completing the triad of François syndrome, a rare NF1 variant. Two presented with leukocoria and were referred to as retinoblastoma suspects. Histopathology showed ganglioneuroma, a benign choroidal tumor, associated with NF-1, which does not need treatment. Knowledge of this rare condition avoids misdiagnosis of retinoblastoma, prevents aggressive management, and the associated psychological impact.
Keywords: Buphthalmos, François syndrome, neurofibromatosis, retinoblastoma mimic
Neurofibromatosis-1 (NF-1) is the commonest neurocutaneous syndrome[1] with autosomal dominant hereditary. It is characterized by café-au-lait spots and plexiform neurofibromatosis along the distribution of the trigeminal nerve, skeletal dysplasias, and growth of both benign and malignant nervous system tumors. Ocular manifestations include iris Lisch nodules (do not interfere with vision), and optic nerve gliomas (causing vision loss and proptosis).[1]
Retinoblastoma, in contrast, is the commonest primary intraocular tumor arising from immature retinal cells. It is a round cell tumor of the under-5 age group that grows rapidly and can be fatal if not treated aggressively.[2]
Case Series
An eleven year old Sudanese girl had a painful, large, blind eye and “abnormal” facies. She was suspected to have retinoblastoma elsewhere; however, treatment was withheld due to an unconfirmed diagnosis.
She had left-sided buphthalmos, Lisch nodules, and cataract. The left face had large pigmented patches, thickened redundant skin, plexiform neurofibroma, and severe blepharoptosis. She sought cosmetic correction to avoid social exclusion [Fig. 1a and b].
Figure 1.
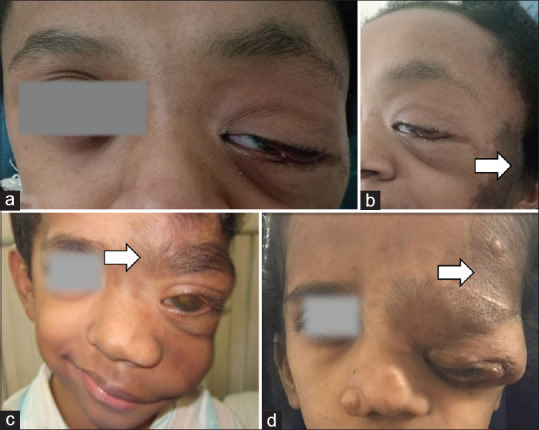
Clinical presentation (Case 1a. and b. Case 2c. Case 3d). Left-sided facial hemihypertrophy, café au lait spots (arrow), plexiform NF, and blepharoptosis
Imaging revealed sphenoidal-wing dysplasia. She underwent enucleation with a scleral-wrapped implant, and eyelid plexiform neuroma excision with ptosis correction using frontalis sling [Fig. 2d]. The eye-ball was 32 mm large with cataract and a choroidal mass [Fig. 2a and c]. Histopathology showed a mixture of mature ganglion cells and Schwann cells. Ganglion cells were large with eosinophilic cytoplasm, single nucleus, and prominent nucleolus, often containing brown pigment, neuromelanin, thus, establishing the diagnosis of ganglioneuroma [Fig. 3d]. The eyelid skin showed proliferation of Schwann cells, consistent with plexiform neurofibroma.
Figure 2.
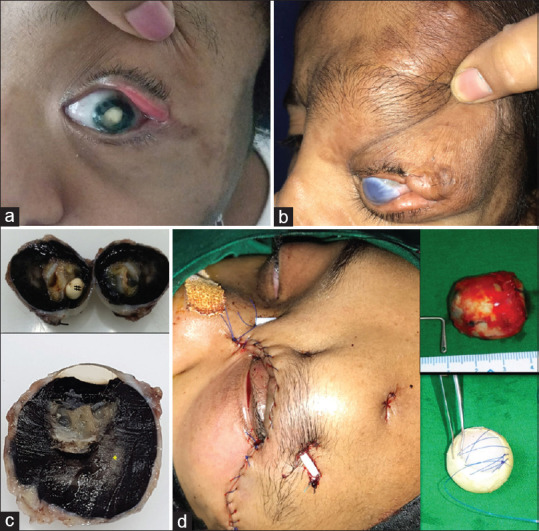
Ocular findings and management (a) Leukocoria and cataract (Case 1) (b) Buphthalmos and anterior staphyloma (Case 2) (c)Gross ocular findings cataractous lens (#) and intraocular and choroidal mass (*) (d) Surgical management with enucleation implant and eyelid mass resection and silicone sling surgery
Figure 3.
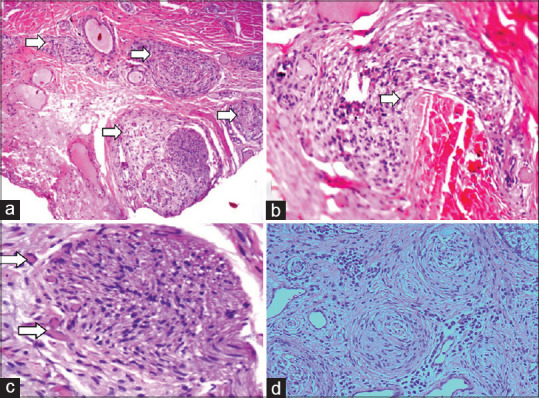
Histopathology (a) Diffuse choroidal hamartoma, (b)neuronal hamartoma, (c) ganglionic choroidal hamartoma, (d) choroidal ganglioneuroma)
A 5-year-old patient with leukocoria was referred as a retinoblastoma suspect. He had progressive vision loss and eye enlargement since birth [Fig. 1c]. Family history was insignificant. Examination revealed left-sided facial hemihypertrophy, hypertrichosis, café au lait spots, eyelid plexiform neurofibroma, and ptosis. The left eye had no perception of light, increased horizontal corneal diameter (14 mm), hyphema, iris neovascularization, and cataract. B scan showed increased axial length (34 mm) and choroidal thickening. Histopathology after enucleation showed diffuse neurofibromas, multiple choroidal hamartomas that were both ganglionic and neuronal [Fig. 3a-c]. He was advised to follow up for custom prosthesis and annual surveillance in view of NF-1.
A 12-year-old patient presented with a left-sided disfigured face and enlarged eye since birth. She faced a social boycott in her village. She had facial hemihypertrophy, plexiform neurofibroma involving the left forehead and eyelids [Fig. 1d]. Eyelids had ptosis, lateral canthal disinsertion, and ectropion [Fig. 2b]. The left eye had anterior staphyloma, an enlarged globe, and no perception of light.
She underwent left eye enucleation with an implant. Eyelid plexiform neurofibroma excision and reconstruction were done subsequently. The eyeball was 32 mm large; however, no choroidal mass or hamartoma was found.
Discussion
The current cases were unique in many ways. Patients had glaucoma and buphthalmos, ipsilateral facial hemihypertrophy, and eyelid plexiform neurofibroma—completing the triad of François syndrome.[3] All cases had cataract and buphthalmos. One was misdiagnosed and treated as infantile glaucoma before establishing a diagnosis.[4] Two had leukocoria due to the cataract and co-existing benign choroidal mass, invoking a suspicion of retinoblastoma. Histopathology of these revealed choroidal ganglioneuromas. These rare, benign intra-ocular tumors arise from primordial neural crest cells and are a part of the NF1 spectrum. Only five cases[5,6] of pediatric choroidal ganglioma with NF-1 are reported in the literature so far [Table 1]. When found in children below 5 years, this could be mistaken as retinoblastoma, which is potentially life-threatening, if not treated promptly. However, retinoblastoma is characterized by intraocular calcifications. Moreover, periocular café-au-lait spots and other features of NF-1 be absent in retinoblastoma. The presence of both retinoblastoma with NF is extremely rare and has been reported only once in the literature.[7]
Table 1.
Reported cases of pediatric choroidal ganglioneuroma in NF-1
| NO. | Demographics (AGE in yrs/sex/eye) | Eye findings Glaucoma=G Cataract=C Buphthalmos=B Leukocoria=L Complete vision loss=V Pain=P |
Management |
|---|---|---|---|
| Case 1[6] | 11 M OS | G + B + V + P | Evisceration + implant |
| Case 2[8] | 7 M OS | G + B + V + P + corneal opacity,+ hyphema + vitreous hemorrhage | Enucleation |
| Case 3[4] | 5 F OD | V + P + proptosis + cavernous sinus mass | Enucleation + Implant |
| Case 4[5] | 1 M OD | G + B + V + P + proptosis | Enucleation + Implant |
| Case 5[9] | 5 M OD | B | Enucleation |
| Case 6 Current series (Case 1) | 11 F OS | G + C + B + L + V + P | Enucleation + implant + neurofibroma resection |
| Case 7 Current series (Case 2) | 5 M OS | G + C + B + L + V + corneal opacity + hyphema + | Enucleation + implant |
Conclusion
In an NF-1 child with eye symptoms, an undiagnosed choroidal ganglioneuroma could exist. Knowledge of this rare, benign ocular tumor that may mimic retinoblastoma avoids the initiation of aggressive treatments such as chemotherapy, which is unwarranted in such cases. It also prevents the negative psychological impact that comes with diagnosing a pediatric malignancy. Being a multi-systemic, inheritable disorder, with a life-time risk of malignant tumors, regular follow-up is recommended.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
Dept of Radiology , SRCC Children’s Hospital Managed by NH, Mumbai
Dept of Pathology, Tata Memorial Hospital, Parel, Mumbai
KBHB Eye and ENT Hospital, Parel, Mumbai
References
- 1.Abdolrahimzadeh B, Piraino DC, Albanese G, Cruciani F, Rahimi S. Neurofibromatosis:An update of ophthalmic characteristics and applications of optical coherence tomography. Clin Ophthalmol. 2016;10:851–60. doi: 10.2147/OPTH.S102830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fabian ID, Onadim Z, Karaa E, Duncan C, Chowdhury T, Scheimberg I, et al. The management of retinoblastoma. Oncogene. 2018;37:1551–60. doi: 10.1038/s41388-017-0050-x. [DOI] [PubMed] [Google Scholar]
- 3.Francois J, Katz C. Association homolatérale d'hydrophtalmie, de névrome plexiforme de la paupière supérieure et d'hémihypertrophie faciale dans la maladie de Recklinghausen. Ophthalmologica. 1961;142:549–71. [Google Scholar]
- 4.Shome D, Vemuganti GK, Honavar SG. Choroidal ganglioneuroma in a patient with neurofibromatosis type 1:A case report. Eye (Lond) 2006;20:1450–1. doi: 10.1038/sj.eye.6702320. [DOI] [PubMed] [Google Scholar]
- 5.Mbagwu M, Rahmani B, Srivastava A, Burrowes D, Bryar PJ. Unsuspected ganglioneuroma of the choroid diagnosed after enucleation. Ocul Oncol Pathol. 2015;2:48–50. doi: 10.1159/000438863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Goyal S, Park A, Zeglam A, Brown H, Pemberton JD. Choroidal ganglioneuroma and orbital plexiform neurofibroma presenting as buphthalmos in an infant with neurofibromatosis type 1. Ophthalmic Plast Reconstr Surg. 2016;32:e87–9. doi: 10.1097/IOP.0000000000000266. [DOI] [PubMed] [Google Scholar]
- 7.Das A, Ghosh P, Zameer L, Ramprasad VL, Bhaduri A. Simultaneous diagnosis of unilateral retinoblastoma and contralateral optic pathway glioma in a child with neurofibromatosis type 1. Pediatr Hematol Oncol. 2019;36:82–5. doi: 10.1080/08880018.2019.1591550. [DOI] [PubMed] [Google Scholar]
- 8.Ishijima K, Kase S, Noda M, Ishida S. Intraocular neovascularization associated with choroidal ganglioneuroma in neurofibromatosis type 1. Eur J Ophthalmol. 2011;21:837–40. doi: 10.5301/EJO.2011.8317. [DOI] [PubMed] [Google Scholar]
- 9.Gilani A, Treece A. Choroidal ganglioneuronal hamartoma in neurofibromatosis type-1. J Pediatr Ophthalmol Strabismus. 2018;55:412. doi: 10.3928/01913913-20180709-04. [DOI] [PubMed] [Google Scholar]