

Abstract
Objective:
To assess the effects of weight loss and weight gain on hip and knee radiographic changes, pain, and joint replacement over 4 years.
Methods:
Participants (n=2752) from the Osteoarthritis (OA) Initiative were classified as those with weight gain (>5% gain), weight loss (>−5% loss), or as controls (−3 to 3% change) over four years. Generalized estimating equations (adjusted for age, gender, and BMI) were used to assess the relationship between weight change group and 4-year changes in knee radiographic OA (Kellgren Lawrence grade (KL)), hip OA (Croft summary grade), joint space narrowing (JSN), and joint pain.
Results:
For radiographic knee OA, weight loss was associated with significantly lower odds of KL grade worsening over four years (OR=0.69, 95%CI=0.53–0.91, p=0.009), and weight gain was significantly associated with higher odds of medial knee JSN (OR=1.29, 95%CI=1.01–1.64, p=0.038) compared to controls. For knee pain, weight loss was significantly associated with knee pain resolution over four years (OR=1.40, 95%CI=1.06–1.86, p=0.019) while weight gain was associated with knee pain development (OR=1.34, 95%CI= 1.08–1.67, p=0.009) compared to controls. For all hip outcomes, no significant associations (p>0.05) were found with weight change groups. The associations between weight change group and total hip or total knee replacement were not significant (p>0.05).
Conclusion:
This large, longitudinal study (n=2752 with 4-year follow-up) suggests that weight loss may protect against, and weight gain may exacerbate radiographic and symptomatic knee OA, while weight change (5% threshold) does not have significant effects on hip OA.
Keywords: weight loss, weight gain, radiographic hip OA, radiographic knee OA
Osteoarthritis (OA) is a disabling degenerative joint disease and a significant public health concern. OA is present in 10.5% of the US population (from The Institute of Health Metrics Evaluation (IHME)’s Global Burden of Disease (GBD) Tool), and patients with OA contribute $460 billion in all-cause medical costs (1). OA often affects large weight-bearing joints such as the hip and knee, and its prevalence increases with higher levels of BMI, especially among adults over 60 years (2). Obesity is a global worldwide epidemic(3), posing a great burden on OA: obese subjects have a 2.63 (95% CI 2.28, 3.05) odds of knee OA development compared to normal-weight controls (4), and obesity has resulted in a significant increase in the incidence of TKR even in a young population (5). Since obesity is a modifiable risk factor for OA (3, 6), understanding the effects of weight gain, and the potential preventive impact of weight loss on hip and knee OA is critical for the development of effective, long-term therapeutic strategies for OA.
Notable factors to be considered when investigating the effects of weight change on OA are (1) the amount of gain or loss (2), the affected tissue (this study focuses on hip and knee) (3), outcome measures (i.e., morphologic joint structure, clinical symptoms) and (4) follow-up time. While studies have shown beneficial effects of weight loss on knee OA (i.e., reduced symptomatic outcomes (7, 8), progression of MRI structural outcomes (9), inflammation (10), knee joint mechanical loads (11), serum markers for cartilage degradation (12)), fewer studies have investigated the effects of weight gain on knee OA (13). In addition, few studies have assessed the effects of both weight loss and weight gain on structural and symptomatic hip OA (14). Understanding how weight change affects hip and knee OA progression may aid clinicians in developing targeted, long-term strategies for site-specific informed recommendations to prevent joint degeneration.
This study utilized data from the Osteoarthritis Initiative (OAI), a longitudinal, multi-center, natural history study of OA, with publicly available clinical questionnaire data and radiographic images of the hip and knee joints. This database provides a unique opportunity to concurrently assess hip and knee joint radiographic and symptomatic longitudinal changes in relation to weight change in a large cohort. The purpose of this study was to assess the effects of weight loss and weight gain on knee and hip radiographic changes, pain, and joint replacement over 4 years using the OAI dataset.
MATERIALS AND METHODS
Subject Selection
This study utilized data from the Osteoarthritis Initiative (OAI https://www.niams.nih.gov/grants-funding/funded-research/osteoarthritis-initiative) (15), a multi-center, longitudinal study of individuals aged 45–79 years at enrollment, aimed at assessing biomarkers for OA development and progression. The OAI dataset includes radiographic knee and hip images of individuals scanned over eight years as well as questionnaires on symptoms. The study protocol, amendments, and informed consent documentation were reviewed and approved by the local institutional review boards of all participating centers.
The individuals in this study were selected as follows: of the 4796 individuals included in the OAI, we included n=4239 that had at least three (of five) annual BMI measurements available (necessary to determine if an individual cycled between weight gain and weight loss over 4 years, as described below). Of those, we excluded: (i) individuals with modest weight loss (16) defined as 3%–5% weight gain and 3%–5% weight loss (ii) individuals with end-stage OA (knee KL 4 or hip JSN grade 3 in the medial and lateral sides) in both knees or both hips, (iii) individuals with rheumatoid arthritis and other co-morbid diseases that may impact weight change (i.e., cardiac failure) and (iv) individuals with weight cycling (17). Based on these criteria, a total of 2752 individuals were included in this study (Figure 1). These individuals were classified in three groups: weight gain (>5%, n=714), weight loss (>−5%, n=485) and controls (−3 to 3% change, n=1553).
Figure 1:
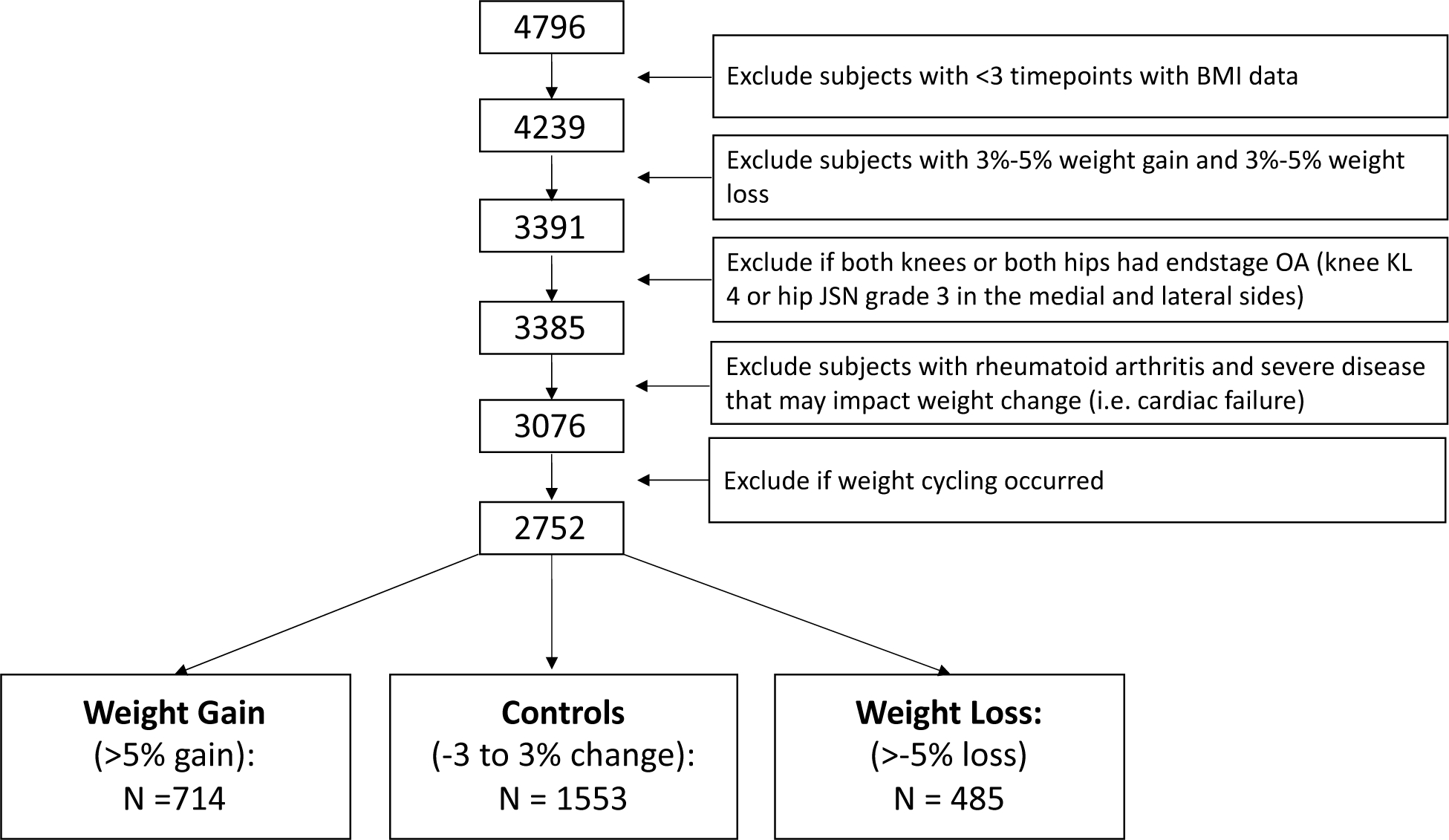
Participant Selection. Abbreviations: KL: Kellgren Lawrence Grade; JSN: Joint Space Narrowing.
Group Definitions
BMI measurements were used to determine the annual rate of change in BMI over 4 years in each individual. The slope of the regression line was multiplied by 4 to determine overall magnitude of BMI change, and the percentage change over 4 years was defined as the magnitude of BMI change divided by the baseline BMI. Individuals were classified into three groups based on their annual changes in BMI over 4 years: weight loss (>−5% change), weight gain (>5% change), and controls without weight change (−3 to 3% change). A 5% threshold was defined based on previous studies, reporting a clinically significant weight loss of 5% (18) and weight gain (13). Weight cycling (exclusion criteria) was defined as weight fluctuation based on the root mean square error (RMSE) of the regression line. We obtained RMSE measurements from each individual’s regression model, and their weight fluctuation was determined based on the RMSE. We defined weight cycling as an RMSE value (19) in the top 10% of all RMSE values. Subjects with weight cycling were excluded from the study as they would not fall into a clear category of weight loss and weight gain, and weight cycling may independently affect OA knee degenerative outcomes (17).
Radiographic Knee Assessment:
Standardized bilateral standing posterior-anterior fixed flexion knee radiographs were acquired in all subjects in the OAI. To assess baseline disease burden and progression of OA, Kellgren Lawrence (KL) gradings and joint space narrowing (JSN – medial and lateral knee joint sides) were assessed at baseline and 4-year follow-up (20). Knee radiographic progression (binary) was defined as positive if KL grade at 4-year follow-up was greater than KL grade at baseline. A KL grade of 0 at baseline and 1 at 4-year follow-up was not defined as positive progression, as KL1 is not uniformly considered as OA and the radiologic findings are considered as doubtful according to the original definition. Progression of JSN (binary) was defined as positive if JSN grade at 4-year follow-up was greater than JSN grade at baseline in either the medial or lateral side of the joint or both.
Radiographic Hip OA Assessment:
Weight-bearing pelvis radiographs at baseline and 4-years were acquired in all subjects in the OAI. Pelvis radiographs were assessed for hip OA using the OARSI atlas (21) by two musculoskeletal radiologists and a rheumatologist. Definite femoral and acetabular osteophytes and superolateral and superomedial JSN were defined as grade ≥2. Hips were classified as “definite RHOA” when the modified Croft grade was ≥2, when there were grade ≥1 femoral or grade ≥2 acetabular osteophytes plus definite JSN, when there were grade ≥2 femoral osteophytes regardless of other features or when there was superolateral JSN >=2 or superomedial JSN >=3 regardless of other features. Hips were classified as “possible RHOA” when other individual or combinations of indefinite individual radiographic features (IRFs) were present, and otherwise considered “normal” (22, 23). Hip radiographic worsening (binary) was defined as positive if a hip radiographic grading at 4 years was greater than that at baseline. A similar definition for binary progression of JSN was utilized. JSN progression was defined in the superolateral and superomedial sides of the hip joint, and also if either the superolateral or superomedial side of the joint had progression.
Knee and Hip Pain
Right and left hip and knee pain were assessed at baseline and 4-years. Individuals were asked whether they had pain, aching or stiffness in the hip or knee on most days of a month during the past year (24). Those who said ‘yes’ were considered to have frequent hip or knee pain. In addition, individuals were also asked if they had hip or knee pain at any time in the 12 months prior to the visit. Individuals were classified into those that developed knee pain (no pain at baseline and developed pain at 4-years), those whose pain resolved (pain at baseline and no pain at 4-year follow-up) and those who had no pain at baseline or follow-up. Subjects with pain at baseline and follow-up were excluded from the analysis with pain as an outcome.
Total Hip and Total Knee Replacement
Individuals were classified as having a knee or hip replacement if they underwent a femoro-tibial total knee replacement (TKR) or total hip replacement (THR), respectively, during any annual timepoint between baseline and 4 years. The tabulated OAI variable was “closest OAI visit after knee or hip replacement.” Two participants (0.07%) had both hip and knee replacements.
Statistical Analysis
Descriptive statistical analysis was performed using SAS Studio version 3.8 (SAS Institute Inc., Cary, NC, USA) using a SAS macro program called “Tablen” (25). Differences in continuous parameters between groups were assessed using T-tests, and differences in categorical parameters between groups were assessed using Chi-squared tests.
The primary analysis was performed using RStudio Version 1.3.1093 (Vienna, Austria) (26). Generalized estimating equations with logistic regression (accounting for two knees or hips per person) were used to assess the relationship between weight change group and outcomes (binary 4-year radiographic progression, binary 4-year pain progression, or occurrence of joint replacement over 4 years). All analyses were adjusted for age, sex, and baseline BMI. An interaction with gender and weight change group was included in the analysis, and if significant, the analysis was subdivided in men and women separately.
RESULTS
Participant Characteristics
2752 participants were included in this study; of those, 714 were categorized having weight gain (>5%), 485 were categorized as having weight loss (>−5%), and 553 were categorized as controls with no weight change (−3 to 3%) over 4 years. Significant differences in age, gender, and baseline BMI were reported between groups (p>0.05). Compared to individuals with weight gain (age: 59.0±8.80 years, BMI: 28.3±4.60 kg/m2)) and controls (age: 61.8±9.14 years, BMI: 27.9±4.58 kg/m2), individuals with weight loss were the oldest (63.2±9.63 years, p<0.0001) and had the highest baseline BMI (28.8±4.79 kg/m2, p=0.0008). The weight gain group had the highest percentage (p<0.001) of females (65.5%) compared to the other groups (weight loss: 62.1% and controls with no weight change: 52.4%). All participant characteristics are listed in Table 1.
Table 1:
Participant Characteristics.
| No Weight change (N=1553) |
Weight gain (N=714) |
Weight loss (N=485) |
Total (N=2752) |
P-value | |
|---|---|---|---|---|---|
|
| |||||
| Age | <0.00011 | ||||
| Mean (SD) | 61.8 (9.14) | 59.0 (8.80) | 63.2 (9.63) | 61.3 (9.26) | |
| BMI | 0.00191 | ||||
| Mean (SD) | 27.9 (4.58) | 28.3 (4.60) | 28.8 (4.79) | 28.2 (4.63) | |
| Sex | <0.00012 | ||||
| Male | 740 (47.6%) | 246 (34.5%) | 184 (37.9%) | 1170 (42.5%) | |
| Female | 813 (52.4%) | 468 (65.5%) | 301 (62.1%) | 1582 (57.5%) | |
| RACE, n (%) | 0.00062 | ||||
| Other Non-white | 22 (1.4%) | 10 (1.4%) | 10 (2.1%) | 42 (1.5%) | |
| White or Caucasian | 1321 (85.1%) | 582 (81.6%) | 368 (76.0%) | 2271 (82.6%) | |
| Black or African American | 196 (12.6%) | 117 (16.4%) | 100 (20.7%) | 413 (15.0%) | |
| Asian | 14 (0.9%) | 4 (0.6%) | 6 (1.2%) | 24 (0.9%) | |
| Missing | 0 | 1 | 1 | 2 | |
T-test p-value
Chi-Square p-value
Radiographic Outcomes
Knee Radiographic outcomes
Of the 2752 individuals in this study (5504 knees), right or left knee KL worsening occurred in n=607 (11.0%) of knees, medial JSN occurred in n=563 (10.2%) of knees, lateral JSN occurred in n=256 (4.6%) of knees, and either medial or lateral JSN occurred in n=740 (13.4%) of knees. Knee KL worsening occurred in 83 knees (8.5%) in the weight loss group, 155 (10.9%) knees in the weight gain group and 369 knees (11.9%) in the control group. Medial JSN worsening occurred in 85 knees (8.8%) in the weight loss group, 160 (11.2%) knees in the weight gain group and 318 knees (10.2%) in the control group without weight change. Lateral JSN worsening occurred in 48 knees (4.9%) in the weight loss group, 59 (4.1%) knees in the weight gain group and 149 knees (4.8%) in the control group.
Table 2 lists the associations between weight change and knee radiographic outcomes. Weight loss was associated with significantly lower odds of KL grade worsening over four years (OR=0.69, 95%CI=0.53–0.91, p=0.009), and weight gain was significantly associated with higher odds of medial knee JSN (OR=1.29, 95%CI=1.01–1.64, p=0.038) compared to controls without weight change (Figure 2). The remaining associations between weight change and radiographic knee outcomes were not statistically significant (p>0.05).
Table 2:
Associations between weight change and knee and hip radiographic outcomes. Abbreviations: KL: Kellgren Lawrence Grade; JSN: Joint Space Narrowing; OR: odds ratio; CI: confidence interval. All GEE analyses are adjusted for age, gender and BMI and include right and left body sides.
| KNEE | KL worsening | Medial or lateral JSN | Medial JSN | Lateral JSN | ||||||||
|
| ||||||||||||
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |
| No Weight Change | Reference | Reference | Reference | Reference | ||||||||
| Weight Gain | 0.95 | 0.76 – 1.19 | 0.652 | 1.14 | 0.91 – 1.41 | 0.256 | 1.29 | 1.01 – 1.64 | 0.038 | 0.97 | 0.69 – 1.36 | 0.869 |
| Weight Loss | 0.69 | 0.53 – 0.91 | 0.009 | 0.88 | 0.68 – 1.13 | 0.318 | 0.85 | 0.63 – 1.13 | 0.263 | 1.01 | 0.69 – 1.47 | 0.956 |
|
| ||||||||||||
| HIP | Worsening of hip ROA | Superolateral or Superomedial JSN | Superomedial JSN | Superolateral JSN | ||||||||
|
| ||||||||||||
| No Weight Change | Reference | Reference | Reference | Reference | ||||||||
| Weight Gain | 1.31 | 0.88 – 1.95 | 0.181 | 1.17 | 0.81 – 1.68 | 0.411 | 1.23 | 0.79 – 1.90 | 0.362 | 1.16 | 0.71 – 1.88 | 0.560 |
| Weight Loss | 1.02 | 0.64 – 1.63 | 0.925 | 1.07 | 0.73 – 1.57 | 0.739 | 1.22 | 0.78 – 1.90 | 0.380 | 0.96 | 0.58 – 1.62 | 0.891 |
Figure 2:
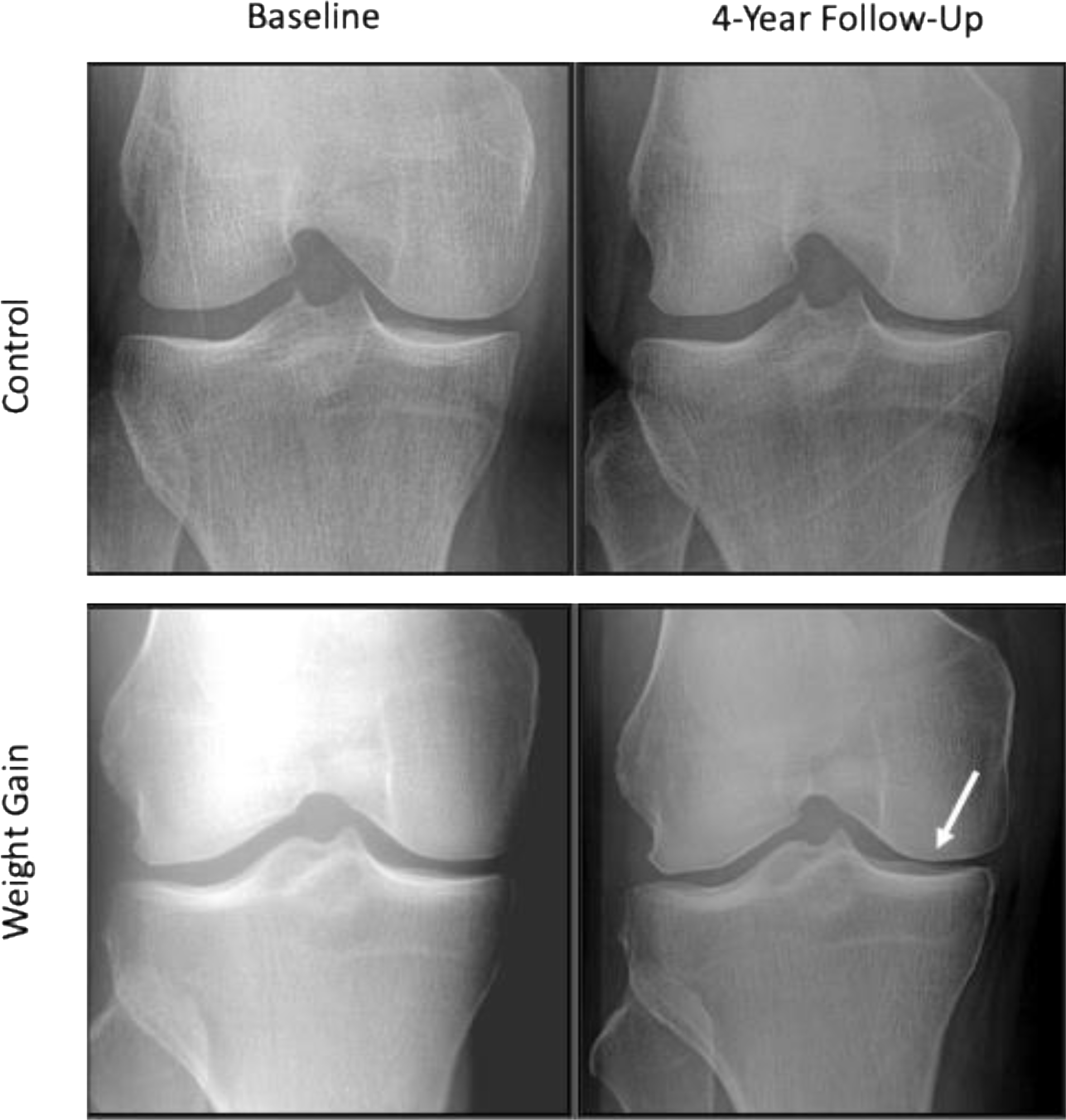
Top Row: A 54-year-old female in the control group (2.61% weight gain over 4 years) with JSN grade = 0 at both baseline and 4-year follow-up.
Bottom Row: A 55-year-old female in the weight gain group (12.57% weight gain over 4 years) with JSN grade = 0 at baseline and JSN grade = 1 at 4-year follow-up.
Hip Radiographic Outcomes
Of the 2752 individuals in this study (5504 hips), right or left hip radiographic worsening occurred in n=159 (2.9%) of hips, superomedial JSN occurred in n=175 (3.2%) of hips, superolateral JSN occurred in n=123 (2.2%) of hips, and either superomedial or superolateral JSN occurred in n=252 (4.4%) of hips. Hip KL worsening occurred in 26 hips (2.7%) in the weight loss group, 43 (3.0%) hips in the weight gain group and 90 hips (2.9%) in the control group without weight change. Hip superomedial JSN occurred in 36 hips (3.7%) in the weight loss group, 42 (2.9%) hips in the weight gain group and 97 hips (3.1%) in the control group. Hip superolateral JSN occurred in 20 hips (2.1%) in the weight loss group, 28 (2.0%) hips in the weight gain group and 75 hips (2.4%) in the control group without weight change. There were no statistically significant associations (p>0.05) between weight change and hip radiographic outcomes (Table 2).
Pain Outcomes
Knee pain
For knee pain development (defined as individuals with no knee pain at baseline and had knee pain at 4-year follow-up): of the 2752 individuals in this study (5504 knees) n=731 (13.3%) developed frequent knee pain (most days of the month in the past year), and 679 (12.3%) developed pain at any time in the past 12 months prior to the visit.
For knee pain resolution (defined as individuals with knee pain at baseline that did not have knee pain at 4-year follow-up): of the 2752 individuals in this study (5504 knees) n=865 (15.7%) had frequent knee pain resolution (most days of the month in the past year), and n=748 (13.6%) developed knee pain at any time in the past 12 months prior to the visit.
Table 3 lists the associations between weight change and knee pain outcomes. Weight loss was significantly associated with knee pain resolution (OR=1.40, 95% CI=1.06–1.86, p=0.019) while weight gain was associated with knee pain development over 4 years (OR=1.34, 95% CI=1.08–1.67, p=0.009) compared to the control group without weight change. The remaining associations between weight change and knee pain development or resolution were not statistically significant (p>0.05). Weight gain was not significantly associated with development of hip pain (OR=1.08, 95%CI=0.84–1.38, p=0.561), and weight loss was not significantly associated with hip pain resolution (OR=1.03, 95%CI=0.76–1.39, p=0.86).
Table 3:
Associations between weight change and knee and hip pain outcomes. Frequent knee pain is defined as having knee pain more than half the days of the month. Abbreviations: OR: odds ratio; CI: confidence interval. All GEE analyses are adjusted for age, gender and BMI and include right and left body sides.
| KNEE | Develop frequent knee pain | Knee pain development – any over 12 months | Frequent knee pain resolution | Knee pain resolution - any over 12 months | ||||||||
|
| ||||||||||||
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |
| No Weight Change | Reference | Reference | Reference | Reference | ||||||||
| Weight gain | 1.34 | 1.08 – 1.67 | 0.009 | 1.13 | 0.86 – 1.48 | 0.377 | 1.00 | 0.80 – 1.24 | 0.987 | 1.04 | 0.79 – 1.36 | 0.775 |
| Weight loss | 1.00 | 0.76 – 1.32 | 0.976 | 1.03 | 0.76 – 1.39 | 0.835 | 1.26 | 0.99 – 1.60 | 0.061 | 1.40 | 1.06 – 1.86 | 0.019 |
|
| ||||||||||||
| HIP | Develop frequent hip pain | Develop hip pain – any over 12 months | Frequent hip pain resolution | Hip pain resolution – any over 12 months | ||||||||
|
| ||||||||||||
| No Weight Change | Reference | Reference | Reference | Reference | ||||||||
| Weight gain | 1.08 | 0.84 – 1.38 | 0.561 | 1.00 | 0.79 – 1.26 | 0.993 | 0.91 | 0.70 – 1.19 | 0.513 | 1.15 | 0.92 – 1.43 | 0.222 |
| Weight Loss | 0.95 | 0.70 – 1.28 | 0.720 | 0.84 | 0.64 – 1.10 | 0.206 | 1.03 | 0.76 – 1.39 | 0.859 | 1.00 | 0.78 – 1.29 | 0.983 |
Hip pain
For hip pain development (defined as individuals with no hip pain at baseline that had hip pain at 4-year follow-up): of the 2752 individuals in this study (5504 hips) n=527 (9.6%) developed frequent hip pain (most days of the month in the past year), and n=762 (13.8%) developed hip pain at any time in the past 12 months prior to the visit.
For hip pain resolution (defined as individuals with hip pain at baseline that did not have hip pain at 4-year follow-up): of the 2752 individuals in this study (5504 knees) n=511 (9.3%) had frequent hip pain resolution (most days of the month in the past year), and n=864 (15.7%) had hip pain resolution at any time in the past 12 months prior to the visit. There were no statistically significant associations (p>0.05) between weight change and hip pain development or resolution over 4 years (Table 3).
Joint Replacement
Of the 2752 individuals enrolled in this study, n=79 (1.4%) had a TKR in either the right or left knee, and n=64 (1.2%) had a THR in either the right or left hip at any timepoint (measured annually) between baseline and 4 years. No significant associations were reported between weight change and either TKR or THR (p>0.05), Table 4.
Table 4:
Associations between weight change and total knee replacement (TKR) and total hip replacement (THR) outcomes. Abbreviations: OR: odds ratio; CI: confidence interval. All GEE analyses are adjusted for age, gender and BMI and include right and left body sides.
| THR | TKR | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| OR | 95% CI | P | OR | 95% CI | P | |
| No Weight Change | Reference | Reference | ||||
| Weight Gain | 1.37 | 0.74 – 2.55 | 0.31 | 1.50 | 0.90 – 2.49 | 0.12 |
| Weight Loss | 1.22 | 0.65 – 2.30 | 0.52 | 1.11 | 0.59 – 2.07 | 0.74 |
Gender Interactions
The interaction between weight change and gender was not significant for all analyses (p>0.05): The gender interaction p-values for knee radiographic outcomes ranged from p=0.43 for medial JSN to p=0.91 for lateral JSN, while the gender interaction p-values for hip radiographic outcomes ranged from p=0.41 for superolateral JSN to p=0.89 for worsening of hip ROA. The gender interaction p-values values for knee pain outcomes ranged from p=0.28 for knee pain resolution at any time in the past 12 months to p=0.62 for frequent knee pain resolution. The gender interaction p-values for hip pain outcomes ranged to p=0.47 for developing frequent hip pain to p=0.53 for developing hip pain at any time in the past 12 months. The p-values for the gender interaction between weight change and gender for TKR and THR outcomes were p=0.74 and p=0.30, respectively.
DISCUSSION
In this study, weight loss (>−5% loss over 4 years) was associated with significantly less progression of knee radiographic OA (KL grade) and less knee pain over 4 years. Weight gain (>5% over 4 years) was associated with greater medial knee radiographic progression and knee pain development. In contrast, no significant effects were observed between weight change (loss or gain) and hip OA. This large, longitudinal study (n=2752 with 4-year follow-up) suggests that weight loss may protect against, and weight gain may exacerbate radiographic and symptomatic knee OA, while weight change (5% threshold) does not have significant effects on hip OA.
This study reported that weight loss was associated with less knee KL worsening; however, no significant associations with knee JSN were observed. The varied results in radiographic progression outcomes in relation to weight loss may be due to distinct features of KL grade vs. JSN: KL grade can detect changes in osteophytes that may not be apparent when measuring JSN (i.e., KL grade=2 represents possible narrowing of the joint space with definite osteophyte formation (27)). Overall, this study showed that weight loss was associated with less KL progression, possibly driven by slower formation of osteophytes rather than worsening of JSN.
Similar to the present study, others have reported no significant associations between weight loss and knee JSN (28): Messier et al. found that 18-month changes (n=76) in joint space width (JSW) were not significantly different between “high” weight loss (10.2%), “low” weight loss (2.7%) and controls (1.5% gain) (29). Another study reported no changes in JSW over 18- months in 316 overweight and obese adults that were randomized into diet only groups, exercise only groups, diet and exercise groups, and controls(30). Three main differences are notable between our study and the above-mentioned studies: (1) sample size (our study enrolled n=2752 while their studies enrolled n=76 and n=316, respectively), (2) our study was retrospective in nature and the other studies were prospective, and (3) the follow-up time in our study was 4-years while the follow-up times in the above-mentioned studies were 18 months. While the differences in the three study designs (especially the follow-up time) impede their direct comparison, the primary JSN findings were in agreement: weight loss was not significantly associated with knee JSN, and according to our study, weight loss was associated with lower odds of KL grade progression (potentially due to slower osteophyte progression).
In the current study, weight gain was associated with increased medial knee JSN over 4 years. Similarly, Bucknor et al. reported that weight gain of over 5% over 4 years was associated with increased odds of cartilage (OR=11.3, 95%CI 3.5–51.4) and meniscus lesions (OR=4.5, 95%CI 1.4–17.3) measured on MRI (13), and Teichtahl et al. reported an association between weight gain and increased cartilage loss in adults with meniscal tears (31). Collectively, these studies suggest that weight gain may be associated with increased knee joint degeneration evidenced by both radiography and by MRI.
The significant associations between weight change and structural and symptomatic knee OA, but not hip OA observed in this study corroborate other previously published research. Studies have shown that: weight loss (>7.5%) was associated with reduced risk of TKR (HR= 0.69, 95%CI 0.54–0.87) and not THR (32), greater body mass index in men ages 20 to 29 years was correlated with an increased risk of subsequent knee, but not hip OA (33), and the relationship between BMI and pain prevalence was stronger for knee pain (underweight 12.1% to obesity class III 55.7%) than for hip pain (underweight 10.4% to obesity class III 23.3%) (2). In addition, Riejman et al. reported that a BMI of >27 kg/m2 at baseline was associated with incident knee OA (OR=3.3), but not with incident hip OA (34). Collectively, these studies suggest that weight change may have distinct effects on the knee compared to the hip.
The mechanisms underlying the relationship between weight change and OA are multi-factorial, potentially due to changes in mechanical loading patterns, inflammation, and blood biomarker concentrations. Studies have shown that weight loss in an overweight and obese osteoarthritic population had lower knee joint compressive loads during walking compared to low and no weight loss groups (29) as well as potential increases in knee adduction moment during weight gain (35). In addition, massive weight loss following gastric surgery resulted in decreased low-grade inflammation (12), increases in cartilage syntheses (N-terminal propeptide of type IIA collagen levels), and decreases in cartilage degradation (cartilage oligomeric matrix protein) (12). Increases in adipose tissue due to weight gain “may have a metabolic effect on joints via the dysregulation of cytokine production by adipose tissue that has been linked to hyperalgesia and the development and progression of chronic pain (35).” Overall, the mechanisms responsible for changes in joint degeneration due to weight change are complex, and future studies are needed to examine the interplay of factors involved in knee joint degeneration.
Potential explanations explaining the differing effects weight change on the knee vs. the hip are complex, and may include varied mechanical loading patterns that are anatomically-specific to the hip and knee (i.e., malalignment may not affect the hip joint (ball and socket), while it is associated with OA of the knee (34)), “the hip joint is less sensitive to obesity and weight change than the knee joint” (32), and cartilage thickness of the knee is significantly greater than that of the hip (p<0.001) (36)). Of interest, in the current study, hip and knee pain progression percentages had approximately similar ranges (knee pain range: 12.3% to 13.3%; hip pain range: 9.6% to 13.8%), while radiographic progression was greater in the knee than that in the hip (i.e., knee KL progression was 11.0% vs hip radiographic worsening was 2.9%). The lower percentage of hip radiographic progression compared to that of the knee highlights that structural progression in the knee vs. hip joint may have differing rates, that may not be evident when assessing changes in pain. Collectively, these studies suggest that weight change may have varied effects on the knee compared to the hip, and future explorations on the direct mechanisms responsible for these differences would be valuable.
The primary limitations of this study are its retrospective nature, lack of statistical correction for multiple testing, and the lack of information on reasons for and methods by which participants gained or lost weight. A future, prospective randomized controls study may aid in identifying the mechanisms responsible for differences in weight change effects between knee vs. hip. In addition, using MRI outcomes would be useful to better understand the impact of weight change on degeneration of individual joint tissues such as cartilage and bone marrow particularly in the hip, as studies in the knee have previously shown that weight loss is associated with slower progression of morphologic (9) and biochemical cartilage degeneration (37). MR images were not available in the OAI for in the hip joint; consequently, MRI-based hip joint morphology could not be quantified. While MRI-based T1rho or other cartilage quantitative measures would be of interest, T1rho measurements were not available in the OAI, and while T2 images were available in the knee, they were not available in the hip. Despite these limitations, the unique strengths of our study were its availability of outcomes measures in both the hip and the knee, its large sample size, and its relatively long follow-up duration.
Understanding the effects of weight change on the hip and knee joint degeneration may aid clinicians in developing site-specific recommendations for non-invasive therapies for knee and hip OA. For example, since this study showed no significant effects of structural or symptomatic changes with weight loss in the hip but demonstrated positive associations for the knee, clinicians may emphasize weight loss recommendations for knee OA prevention, and potentially explore incorporative strategies for hip, such as muscle strengthening (possibly in conjunction with weight loss). Overall, this study provides a foundation exploring the effects of weight change on radiographic OA; however, additional prospective and MRI-based studies in the hip must be undertaken for further understanding of hip soft tissue joint degeneration in relation to weight change.
Overall, the results of this study suggest that weight loss (>−5%) is associated with less knee radiographic worsening and decreases in knee pain over 4 years compared to no weight change. Weight gain (>5%) over 4 years is associated with higher odds of medial JSN and knee pain development over 4 years. No significant associations were found between weight change and hip radiographic OA or changes in hip pain.
SIGNIFICANCE AND INNOVATIONS.
Weight loss (>−5%) is associated with less knee radiographic worsening and decreases in knee pain over 4 years compared to no weight change.
Weight gain (>5%) is associated with higher odds of medial knee joint space narrowing and knee pain development over 4 years.
No significant associations were found between weight change and hip radiographic OA or changes in hip pain.
Understanding the effects of weight change on the hip and knee joint degeneration may aid clinicians in developing site-specific recommendations for non-invasive therapies for knee and hip OA.
Funding Source:
This study was funded by NIH R01-AR064771, NIH R01-AR078917 and NIH R01-AG070647. The OAI is a public-private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health.
Footnotes
Disclosure: The authors declared no conflict of interest.
REFERENCES:
- 1.Lo J, Chan L, Flynn S. A Systematic Review of the Incidence, Prevalence, Costs, and Activity and Work Limitations of Amputation, Osteoarthritis, Rheumatoid Arthritis, Back Pain, Multiple Sclerosis, Spinal Cord Injury, Stroke, and Traumatic Brain Injury in the United States: A 2019 Update. Archives of physical medicine and rehabilitation. 2021;102(1):115–31. Epub 2020/04/28. doi: 10.1016/j.apmr.2020.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Andersen RE, Crespo CJ, Bartlett SJ, Bathon JM, Fontaine KR. Relationship between body weight gain and significant knee, hip, and back pain in older Americans. Obesity research. 2003;11(10):1159–62. [DOI] [PubMed] [Google Scholar]
- 3.King LK, March L, Anandacoomarasamy A. Obesity & osteoarthritis. Indian J Med Res. 2013;138:185–93. [PMC free article] [PubMed] [Google Scholar]
- 4.Blagojevic M, Jinks C, Jeffery A, Jordan KP. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2010;18(1):24–33. Epub 2009/09/16. doi: 10.1016/j.joca.2009.08.010. [DOI] [PubMed] [Google Scholar]
- 5.Chen L, Zheng M, Chen Z, Peng Y, Jones C, Graves S, et al. The burden of end-stage osteoarthritis in Australia: a population-based study on the incidence of total knee replacement attributable to overweight/obesity. Osteoarthritis Cartilage. 2021. Epub 2021/12/11. doi: 10.1016/j.joca.2021.10.017. [DOI] [PubMed] [Google Scholar]
- 6.Christensen R, Bartels EM, Astrup A, Bliddal H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2007;66(4):433–9. Epub 2007/01/06. doi: 10.1136/ard.2006.065904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gersing AS, Solka M, Joseph GB, Schwaiger BJ, Heilmeier U, Feuerriegel G, et al. Progression of cartilage degeneration and clinical symptoms in obese and overweight individuals is dependent on the amount of weight loss: 48-month data from the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2016;24(7):1126–34. Epub 2016/02/02. doi: 10.1016/j.joca.2016.01.984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gudbergsen H, Boesen M, Lohmander LS, Christensen R, Henriksen M, Bartels EM, et al. Weight loss is effective for symptomatic relief in obese subjects with knee osteoarthritis independently of joint damage severity assessed by high-field MRI and radiography. Osteoarthritis Cartilage. 2012;20(6):495–502. Epub 2012/03/10. doi: 10.1016/j.joca.2012.02.639. [DOI] [PubMed] [Google Scholar]
- 9.Gersing AS, Schwaiger BJ, Nevitt MC, Joseph GB, Chanchek N, Guimaraes JB, et al. Is Weight Loss Associated with Less Progression of Changes in Knee Articular Cartilage among Obese and Overweight Patients as Assessed with MR Imaging over 48 Months? Data from the Osteoarthritis Initiative. Radiology. 2017;284(2):508–20. Epub 2017/05/04. doi: 10.1148/radiol.2017161005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Forsythe LK, Wallace JM, Livingstone MB. Obesity and inflammation: the effects of weight loss. Nutr Res Rev. 2008;21(2):117–33. Epub 2008/12/18. doi: 10.1017/S0954422408138732. [DOI] [PubMed] [Google Scholar]
- 11.Messier SP, Gutekunst DJ, Davis C, DeVita P. Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis Rheum. 2005;52(7):2026–32. Epub 2005/06/30. doi: 10.1002/art.21139. [DOI] [PubMed] [Google Scholar]
- 12.Richette P, Poitou C, Garnero P, Vicaut E, Bouillot JL, Lacorte JM, et al. Benefits of massive weight loss on symptoms, systemic inflammation and cartilage turnover in obese patients with knee osteoarthritis. Ann Rheum Dis. 2011;70(1):139–44. Epub 2010/10/29. doi: 10.1136/ard.2010.134015. [DOI] [PubMed] [Google Scholar]
- 13.Bucknor MD, Nardo L, Joseph GB, Alizai H, Srikhum W, Nevitt MC, et al. Association of cartilage degeneration with four year weight gain--3T MRI data from the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2015;23(4):525–31. doi: 10.1016/j.joca.2014.10.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Daugaard CL, Hangaard S, Bartels EM, Gudbergsen H, Christensen R, Bliddal H, et al. The effects of weight loss on imaging outcomes in osteoarthritis of the hip or knee in people who are overweight or obese: a systematic review. Osteoarthritis Cartilage. 2020;28(1):10–21. Epub 2019/11/30. doi: 10.1016/j.joca.2019.10.013. [DOI] [PubMed] [Google Scholar]
- 15.Peterfy C, Schneider E, Nevitt M. The osteoarthritis initiative: report on the design rationale for the magnetic resonance imaging protocol for the knee. Osteoarthritis and Cartilage. 2008;16:1433–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Swift DL, Johannsen NM, Lavie CJ, Earnest CP, Blair SN, Church TS. Effects of clinically significant weight loss with exercise training on insulin resistance and cardiometabolic adaptations. Obesity. 2016;24(4):812–9. Epub 2016/03/05. doi: 10.1002/oby.21404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Joseph GB, Ramezanpour S, McCulloch CE, Nevitt MC, Lynch J, Lane NE, et al. Weight Cycling and Knee Joint Degeneration in Individuals with Overweight or Obesity: Four-Year Magnetic Resonance Imaging Data from the Osteoarthritis Initiative. Obesity. 2021;29(5):909–18. Epub 2021/04/03. doi: 10.1002/oby.23129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Williamson DA, Bray GA, Ryan DH. Is 5% weight loss a satisfactory criterion to define clinically significant weight loss? Obesity. 2015;23(12):2319–20. Epub 2015/11/03. doi: 10.1002/oby.21358. [DOI] [PubMed] [Google Scholar]
- 19.Kataja-Tuomola M, Sundell J, Mannisto S, Virtanen MJ, Kontto J, Albanes D, et al. Short-term weight change and fluctuation as risk factors for type 2 diabetes in Finnish male smokers. European journal of epidemiology. 2010;25(5):333–9. Epub 2010/03/31. doi: 10.1007/s10654-010-9444-6. [DOI] [PubMed] [Google Scholar]
- 20.Kellgren J, Jeffrey M, Ball J. The epidemiology of chronic rheumatism. Atlas of standard radiographs of arthritis. Oxford, UK: Blackwell Scientific Publications; 1963. [Google Scholar]
- 21.Altman RD, Gold GE. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthritis Cartilage. 2007;15 Suppl A:A1–56. Epub 2007/02/27. doi: S1063-4584(06)00328-1 [pii] 10.1016/j.joca.2006.11.009 [doi]. PubMed PMID: 17320422. [DOI] [PubMed] [Google Scholar]
- 22.Croft P, Cooper C, Coggon D. Case definition of hip osteoarthritis in epidemiologic studies. J Rheumatol. 1994;21(4):591–2. [PubMed] [Google Scholar]
- 23.Arden NK, Lane NE, Parimi N, Javaid KM, Lui LY, Hochberg MC, et al. Defining incident radiographic hip osteoarthritis for epidemiologic studies in women. Arthritis Rheum. 2009;60(4):1052–9. Epub 2009/04/01. doi: 10.1002/art.24382 [doi]. PubMed PMID: 19333950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lawrence RC, Helmick CG, Arnett FC, Deyo RA, Felson DT, Giannini EH. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum. 1998;41:778–99. [DOI] [PubMed] [Google Scholar]
- 25.Meyers J Paper AD-088: Demographic Table and Subgroup Summary Macro %TABLEN. Pharmaceuticals SAS Users Group conference; San Francisco, CA: 2020. [Google Scholar]
- 26.Team RC. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2014. 2014. [Google Scholar]
- 27.Kohn MD, Sassoon AA, Fernando ND. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin Orthop Relat Res. 2016;474(8):1886–93. Epub 2016/02/14. doi: 10.1007/s11999-016-4732-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hunter DJ, Beavers DP, Eckstein F, Guermazi A, Loeser RF, Nicklas BJ, et al. The Intensive Diet and Exercise for Arthritis (IDEA) trial: 18-month radiographic and MRI outcomes. Osteoarthritis Cartilage. 2015;23(7):1090–8. Epub 2015/04/19. doi: 10.1016/j.joca.2015.03.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Messier SP, Legault C, Loeser RF, Van Arsdale SJ, Davis C, Ettinger WH, et al. Does high weight loss in older adults with knee osteoarthritis affect bone-on-bone joint loads and muscle forces during walking? Osteoarthritis Cartilage. 2011;19(3):272–80. Epub 2010/12/08. doi: 10.1016/j.joca.2010.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Messier SP, Loeser RF, Miller GD, Morgan TM, Rejeski WJ, Sevick MA, et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis Rheum-Us. 2004;50(5):1501–10. Epub 2004/05/18. doi: 10.1002/art.20256. [DOI] [PubMed] [Google Scholar]
- 31.Teichtahl AJ, Wluka AE, Wang Y, Strauss BJ, Proietto J, Dixon JB, et al. The longitudinal relationship between changes in body weight and changes in medial tibial cartilage, and pain among community-based adults with and without meniscal tears. Ann Rheum Dis. 2014;73(9):1652–8. Epub 2013/06/08. doi: 10.1136/annrheumdis-2013-203210. [DOI] [PubMed] [Google Scholar]
- 32.Jin X, Gibson AA, Gale J, Schneuer F, Ding D, March L, et al. Does weight loss reduce the incidence of total knee and hip replacement for osteoarthritis?-A prospective cohort study among middle-aged and older adults with overweight or obesity. Int J Obes (Lond). 2021;45(8):1696–704. Epub 2021/05/17. doi: 10.1038/s41366-021-00832-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gelber AC, Hochberg MC, Mead LA, Wang NY, Wigley FM, Klag MJ. Body mass index in young men and the risk of subsequent knee and hip osteoarthritis. The American journal of medicine. 1999;107(6):542–8. Epub 2000/01/07. doi: 10.1016/s0002-9343(99)00292-2. [DOI] [PubMed] [Google Scholar]
- 34.Reijman M, Pols HA, Bergink AP, Hazes JM, Belo JN, Lievense AM, et al. Body mass index associated with onset and progression of osteoarthritis of the knee but not of the hip: the Rotterdam Study. Ann Rheum Dis. 2007;66(2):158–62. Epub 2006/07/14. doi: 10.1136/ard.2006.053538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tanamas SK, Wluka AE, Davies-Tuck M, Wang Y, Strauss BJ, Proietto J, et al. Association of weight gain with incident knee pain, stiffness, and functional difficulties: a longitudinal study. Arthritis care & research. 2013;65(1):34–43. Epub 2012/06/08. doi: 10.1002/acr.21745. [DOI] [PubMed] [Google Scholar]
- 36.Shepherd DE, Seedhom BB. Thickness of human articular cartilage in joints of the lower limb. Ann Rheum Dis. 1999;58(1):27–34. Epub 1999/05/27. doi: 10.1136/ard.58.1.27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gersing AS, Schwaiger BJ, Nevitt MC, Zarnowski J, Joseph GB, Feuerriegel G, et al. Weight loss regimen in obese and overweight individuals is associated with reduced cartilage degeneration: 96-month data from the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2019;27(6):863–70. Epub 2019/03/03. doi: 10.1016/j.joca.2019.01.018. [DOI] [PMC free article] [PubMed] [Google Scholar]