
FIGURE 5.
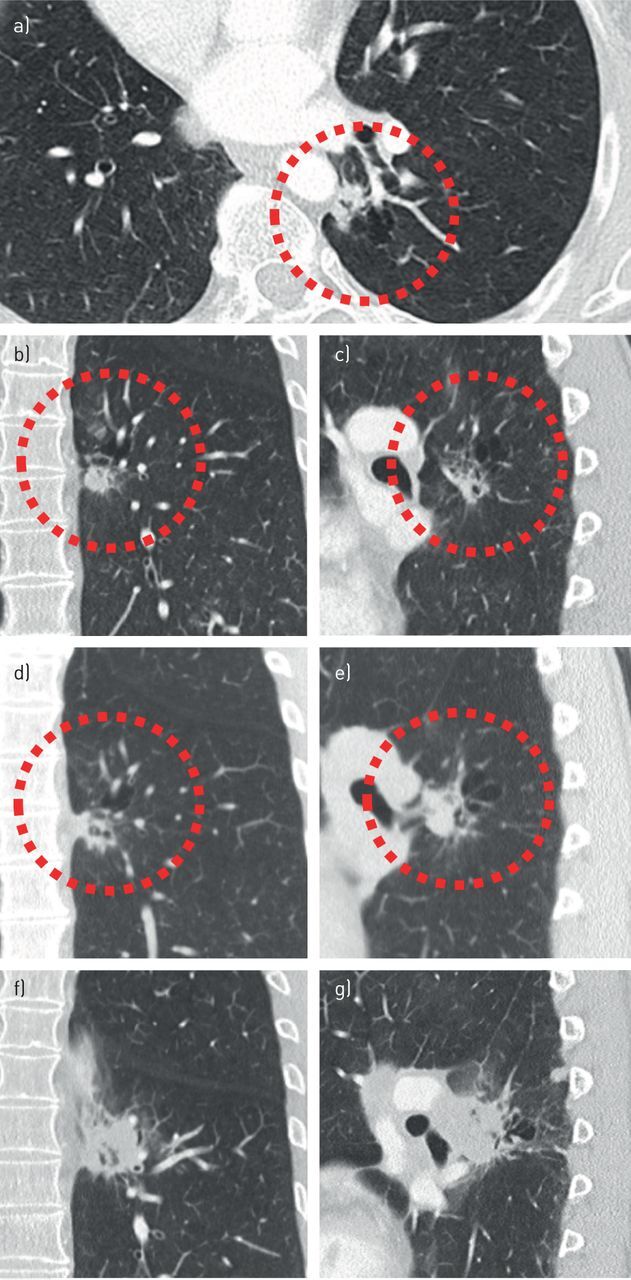
Failure to recognise cyst-related malignancies can lead to significant diagnostic delay. a–c) A cyst-related lesion in the left lower lobe of a 57-year-old female without a relevant history, shown in three orthogonal planes. Initially the lesion was interpreted to represent smoking-related changes in an emphysematous lung with several small nodular consolidations. A flurodeoxyglucose-positron emission tomography computed tomography obtained 6 weeks later (not shown) reported slight activity, most likely due to infectious origin. d, e) A follow-up computed tomography (CT) scan 9 months later showed an increase of the solid component, however, this was not acknowledged. The lesion was reported to be unchanged and irrelevant. 8 months later a CT scan was obtained after an ultrasound-guided biopsy of a progressive swelling in the neck showed metastatic disease. f, g) This CT scan showed an extensive increase in lesion size and confluent left hilar lymphadenopathy. In addition, mediastinal and supraclavicular lymphadenopathy, as well as abdominal and brain metastases, were present by that time (not shown).