
Figure 1. Surgical annotation captures canonical pituitary cell classes in post-natal pituitary gland.
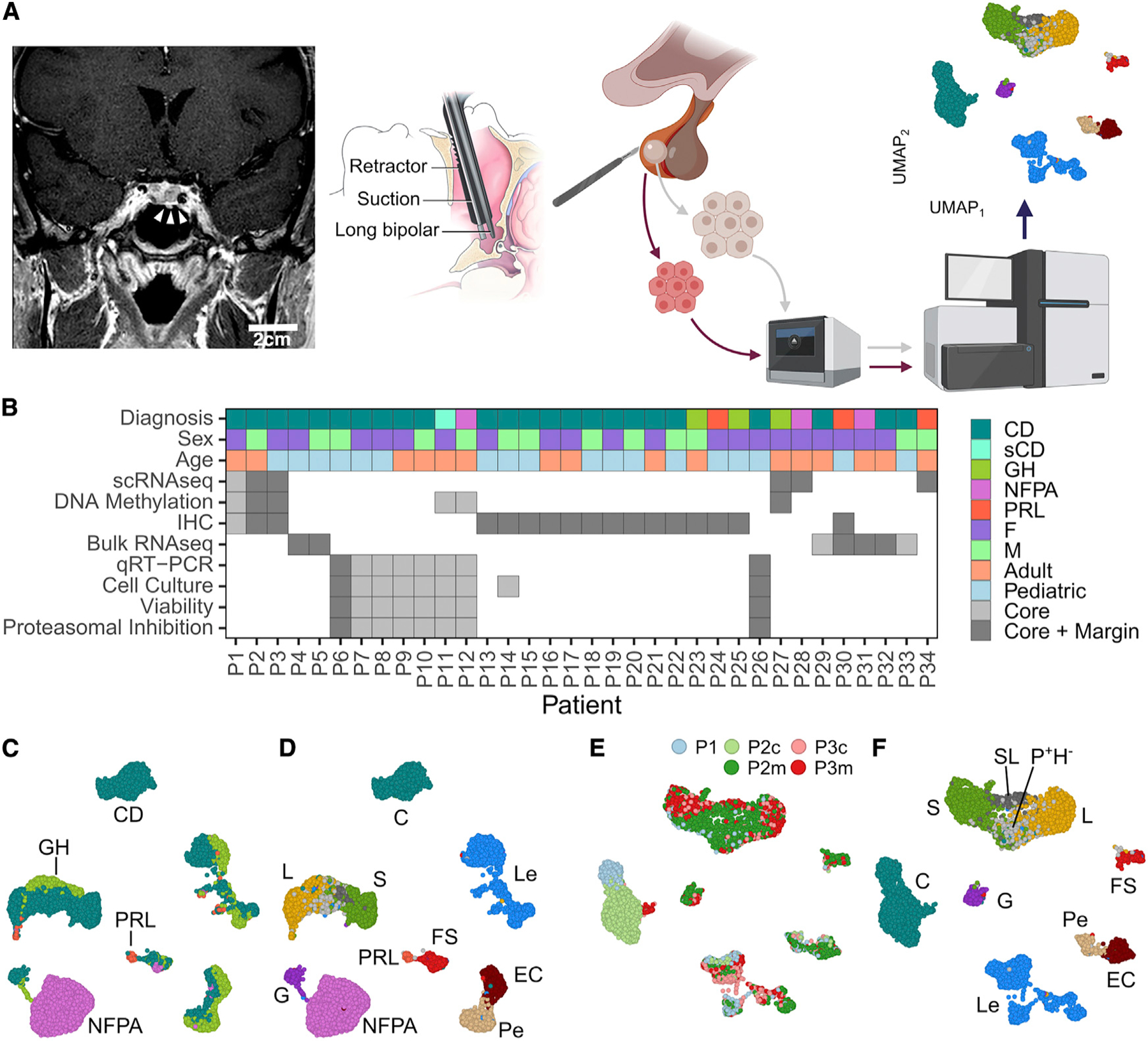
(A) A sublabial transsphenoidal approach was used for resection of microadenomas (white arrowheads) in patients with Cushing’s disease (CD). Coronal, post-gadolinium contrast enhanced magnetic resonance image from patient P1. Adenoma and adjacent normal pituitary gland were separately annotated during surgery and dissociated into a single-cell suspension, followed by GEM embedding, sequencing, and computational analysis. Scale bar: 2 cm.
(B) Summary of demographic data and analysis for patients included in the study.
(C) UMAP embedding of cells from the 6 patient samples with CD, GH, NFPA, and PRL adenomas used in scRNA-seq analysis. Cells cluster according to dominant secretory phenotype.
(D) UMAP embedding showing the cell-type identities cells from the 6 patient samples.
(E) UMAP embedding showing CD sample identity for cells from patients P1, P2, and P3.
(F) UMAP plot showing CD patient cells clustering by cell-type identity. Cell types: leukocytes (Les), endothelial cells (ECs), pericytes (Pes), folliculostellate cells (FSs), corticotrophs (Cs), gonadotroph (Gs), somatotrophs (Ss), lactotrophs (Ls), ambiguous/somato-lactotrophs (SLs), and POU1F1-positive, hormone-negative (P+H−) cells. GH, growth hormone; NFPA, non-functioning pituitary adenoma; PRL, prolactinoma.