

Abstract
Background:
As of July 2018, 45 United States (US) states and the District of Columbia have enacted an overdose Good Samaritan law (GSL). These laws, which provide limited criminal immunity to individuals who request assistance during an overdose, may be of importance in the current wave of the overdose epidemic, which is driven primarily by illicit opioids including heroin and fentanyl. There are substantial differences in the structures of states’ GSL laws which may impact their effectiveness. This study compared GSLs which have legal provisions protecting from arrest and laws which have more limited protections.
Methods:
Using national county-level overdose mortality data from 3109 US counties, we examined the association of enactment of GSLs with protection from arrest and GSLs with more limited protections with subsequent overdose mortality between 2013–2018. Since GSLs are often enacted in conjunction with Naloxone Access Laws (NAL), we examined the effect of GSLs separately and in conjunction with NAL. We conducted these analyses using hierarchical Bayesian spatiotemporal Poisson models.
Results:
GSLs with protections against arrest enactment in conjunction with a NAL were associated with 7% lower rates of all overdose deaths (rate ratio (RR): 0.93% Credible Interval (CI): 0.89–0.97), 10% lower rates in opioid overdose deaths (RR: 0.90; CI: 0.85–0.95) and 11% lower rates of heroin/synthetic overdose mortality (RR: 0.89; CI: 0.82–0.96) two years after enactment, compared to rates in states without these laws. Significant reductions in overdose mortality were not seen for GSLs with protections for charge or prosecution.
Conclusion:
GSLs with more expansive legal protections combined with a NAL, were associated with lower rates of overdose deaths, although these risk reductions take time to manifest. Policy makers should consider enacting and implementing more expansive GSLs with arrest protections to increase the likelihood people will contact emergency services in the event of an overdose.
Keywords: Opioids, Fentanyl, Overdose, Good Samaritan Laws, Naloxone Access Laws
Introduction
For the past two decades, overdose deaths in the United States (US) have been on a precipitous rise, with little sign of abatement (Hedegaard, Miniño, & Warner, 2020a). According to the US National Center for Health Statistics 71,148 people died of an overdose in 2019 and initial data during 2020 suggests the problem is only increasing (Ahmad, Rossen, & Sutton, 2020; CDC Health Alert Network, 2020). The steepest increase in overdose deaths has occurred in the last decade, primarily beginning in 2013 when fentanyl, a synthetic opioid, became increasingly more prevalent the US illicit opioid supply (Hedegaard et al., 2020a; Scholl, Seth, Kariisa, Wilson, & Baldwin, 2018). The age adjusted rate of overdose deaths involving synthetic opioids, mostly illicitly manufactured fentanyl and fentanyl analogs, increased from 1.0 per 100,000 people in 2013 to 11.4 per 100,000 people in 2019 (Hedegaard, Miniño, & Warner, 2020b).
The rise in fentanyl overdose during the most recent wave of the epidemic has posed a substantial challenge for policymakers. Laws to address the opioid overdose epidemic broadly fall into two categories: (1) those that attempt to control the supply of, or access to licit and illicit drugs, and (2) those that attempt to reduce the harms of licit or illicit substances (Cerda, Krawczyk, Hamilton, Rudolph, Friedman, Keyes, 2020). With the exception of laws that criminalize the use and sale of some drugs (the “War on Drugs”), which are largely accepted as having failed to reduce drug-related harm (Beletsky & Davis, 2017), most drug supply or drug access laws primarily target prescription drugs (e.g. prescription drug monitoring programs, pain management clinics (Cerdá et al., 2021; Pacula & Powell, 2018)). Given that the current wave of the epidemic has been driven by illicit opioids (primarily fentanyl and heroin), and evidence which suggests laws intended to decrease inappropriate opioid prescribing increase harm related to illicit opioids (Martins et al., 2019), harm reduction policies may have greater potential to address this current opioid crisis (Pitt, Humphreys, & Brandeau, 2018).
Among the harm reduction laws that have been implemented over the past decade across the US are overdose Good Samaritan laws (GSLs). These laws provide limited protection from certain crimes for an individual who seeks help for someone who experienced an overdose, and sometimes protects the person who overdosed as well. The specific provisions of GSLs vary by state, with some providing protection from arrest, and others providing protection from prosecution or charge or other lesser protections like sentence mitigation.
The current evidence-base on the effectiveness of GSLs is mixed. Individual level studies suggest that, where people are trained on GSLs, they are more likely to call 911 (Jakubowski, Kunins, Huxley-Reicher, & Siegler, 2018; Watson et al., 2018). However, other studies have found that knowledge of GSLs is often limited among both people who seek assistance for an overdose (Evans, Hadland, Clark, Green, & Marshall, 2016; Latimore & Bergstein, 2017) and police and paramedic first responders (Banta-Green, Beletsky, Schoeppe, Coffin, & Kuszler, 2013). Three US population-level analyses of GSL impacts on fatal overdoses have been conducted, two of which found no significant impacts of GSLs (Atkins, Durrance, & Kim, 2019; Rees, Sabia, Argys, Latshaw, & Dave, 2017) and one which found a 15% reduction in fatal overdose (McClellan et al., 2018).
Two potential challenges to developing a better understanding of the impact of GSLs on overdose mortality are that: (1) state GSLs have different legal protections; and (2) GSLs may take time to become effective. GSL legal protections typically only apply to low-level drug offenses such as possession of drugs and drug paraphernalia (PDAPS, 2018b). Different states offer different types of legal protection from low-level drug offenses in cases of bystander intervention, ranging from protection from arrest, to charge or prosecution, to limited sentence mitigation. Different levels of legal protections may influence bystander decisions to call for help in overdose incidents. Only one study has examined the differences in legal provisions, and found no significant differences in their impact on overdose death rates; however, there were substantially fewer states with protections from arrest during this study’s analytic time period (2002–2014) and the fentanyl epidemic only began in approximately 2013 (McClellan et al., 2018).
To observe population-level impacts of GSLs it is also necessary that a substantial proportion of the population whose behavior would be impacted by the GSL is aware of these laws and willing to respond to an overdose. Dissemination of information regarding GSLs and sufficient trust that they will be applied fairly is unlikely to be instantaneous. Therefore, examining their impacts over time is essential to understanding the impact of GSL enactment on overdose mortality.
In this study, we explore the differential impacts that GSLs that protect the person who calls for assistance from arrest, versus GSLs that provide more limited protections (i.e., from charge, prosecution, or that only provide mitigation at sentencing), have on overdose rates. GSL provisions are examined in conjunction with, and separate from, another key type of harm reduction law: Naloxone Access Laws (NALs). Naloxone is a medication that quickly and effectively reverses the effects of opioids (Kerensky & Walley, 2017; Giglio, Li, & DiMaggio, 2015; McClellan et al., 2018; Smart, Pardo, & Davis, 2020; Word Health Organization, 2014). NALs have often been enacted simultaneously or in quick succession with overdose Good Samaritan laws, making it difficult to separate the impact of GSLs from NALs. The impacts of different GSL legal provisions, with and without NALs, are examined for the years 2013–2018, when there was a sharp increase in overdoses related to synthetic, primarily fentanyl-driven, opioids in the US (Hedegaard et al., 2020b).
Methods
Outcome data
National Center for Health Statistics’ multiple cause-of-death mortality files were used to produce three outcome variables: the primary outcome variable: (1) all overdose mortality; and two secondary outcomes: (2) all opioid overdose mortality and (3) all heroin or synthetic opioid overdose mortality (National Center for Health Statistics, 2018). The primary model included International Classification of Disease Tenth Edition (ICD-10) codes to account for any kind of overdose including X40–44 (accidental poisoning by and exposure to noxious substances, including analgesics), X60–64 (intentional self-poisoning by and exposure to drugs, including narcotics and psychodysleptics), X85 (assault by drugs, medicaments, and biologic substances), and Y10–14 (events of undetermined intent, including poisoning by and exposure to narcotics, psychodysleptics, not elsewhere classified, undetermined intent). We also used multiple cause of death data, limiting cause-of-death mortality to only those deaths where ICD-10 codes identified fatal poisoning by (1) any opioid using codes T40.0-T40.4 and T40.6; (2) prescription opioids, including natural and semi-synthetic opioids using code T40.2 and (3) methadone using code T40.3; (4) heroin using code T40.1 and (5) synthetic opioids other than methadone using code T40.4.
Annual counts of overdose deaths were aggregated in 2013–2018 at the county level in 3190 counties in 49 states and DC1. The time frame of 2013–2018 was specifically selected for analysis as 2013 has been identified as the start of the third wave of the overdose epidemic, where mortality was primarily driven by synthetic opioids like fentanyl, causing a sharp increase in overdose death rates. July 2018 provides the most recent data available on state GSL policies (Centers for Disease Control, 2021; PDAPS, 2018b). Although the primary exposure is measured at the state level (see below), county level outcome data was selected since we expected substantial county level variability in overdose rates, and did not want to create an aggregation bias by averaging out overdose mortality to the state level.
Primary and Secondary Exposures
The primary exposure examined in these analyses was the enactment of different forms of state-level GSLs. Data on GSLs were collected from the Prescription Drug Abuse Policy System’s (PDAPS) repository on GSLs for each state between the years of 2013 - July 2018 (PDAPS, 2018b). GSLs were stratified by those that protect the person who calls for assistance from arrest (hereafter called GSL arrest protections), and GSLs that protect the caller from downstream criminal justice consequences including being charged, prosecuted, or some other lesser level of protection. GSLs were considered enacted in a given year if they were in place for at least 7 of months of the year.
NALs were included in the models as a secondary harm reduction-oriented exposure. Naloxone access law data were accessed from PDAPS from 2013-July 2017 (PDAPS, 2017), and 2018 data was imputed from the 2017 values.2 Like GSLs, NALs can have a variety of provisions that vary from state to state (Davis & Carr, 2017). However, since the goal of this paper is to understand the impact of the key provisions of GSLs, a dichotomous measure for enactment of any naloxone access law was used). Both GSL and NAL variables, and indeed all the laws included as covariates described below, are based on laws enacted at the state level as this was the smallest unit of analysis for laws available (there is no county-level GSL national data set).
Because NALs and GSLs are frequently enacted simultaneously or in quick succession (21 states in the same year, 8 within two years), we modeled these variables in combination and separately as follows: (1) state-years where there was a GSL with protection from arrest and a NAL; and (2) state-years where there was a GSL with protections from charge, prosecution or other protections and a NAL, (3) state-years where there was any GSL but no NAL and (4) state-years where there was a NAL but no GSL (arrest or charge). For the any GSL but no NAL measure, we modelled the different GSL provisions together as very few (N =6) states had any GSL prior to a NAL and most for only approximately a year in the years 2013–2018.
Other Covariates
We accounted for a number of demographic and law covariates in the analyses. Models accounted for the following county-level demographic characteristics derived from annual Geolytics data: age (% 0–19, 20–44, 45–64, 65+), race/ethnicity (% non-Hispanic white, % non-Hispanic Black, % Hispanic), gender (% male), socio-economic measures (% of families in poverty, median household income, and % unemployment), and population density (thousands of people per square mile) (Geolytics Inc., 2018).
Law covariates included in the model were two measures of state Prescription Drug Monitoring Programs (PDMPs): a dichotomous variable for if the state had any PDMP law, and a dichotomous variable for whether a state had a PDMP law where the provider was required to query the electronic PDMP system prior to providing a prescription for an opioid (Horwitz, Davis, McClelland, Fordon, & Meara, 2020). The model also controlled for whether or not a state had a Pain Management Clinic law in effect in a given year (PDAPS, 2018a) and whether or not a state had medical cannabis law in effect each year (Britannica ProCon.org, 2020).
Analysis
Although the laws studied all operated at the state level, both licit and illicit drug availability can vary greatly across localities. To allow for intra-state variability in overdose rates, we adopted a multi-level approach. Annual fatal overdose outcomes were measured with sociodemographic covariates and random effects operating at the county level. Conversely, law covariates were modeled at the state level, with state random effects to model between-state variation in overdose risk related to factors such as unmeasured policies and variation in mortality data collection standards. All three outcomes of county-year mortality counts were modeled with hierarchical Bayesian spatiotemporal Poisson models, accounting for county population as the offset (Bernardinelli et al., 1995; Besag, York, & Mollié, 1991; Blangiardo & Cameletti, 2015). Similar to differences-in-difference analyses, each state’s pre-law overdose mortality rates act as a comparison group for its post-law overdose mortality rates. Further, to account for non-linear secular trends in overdose rates across the country, the model included dummy variables for each study year.
A spatiotemporal modeling approach that modeled overdoses at the county level provided three key benefits. First, the models include a conditional autoregressive random effect (CAR) to account for spatial autocorrelation at the county level. Uncontrolled, such spatial autocorrelation can lead to underestimated standard errors of model parameters. Positive spatial autocorrelation was likely to be severe in the current study given that drugs obtained in one county will often contribute to overdose deaths in neighboring counties (either within or between states). Specifications that account for spatial autocorrelation have been shown to reduce small-area effects while also controlling for over-dispersion (Waller & Gotway, 2004). Second, the models included a county-level random slope, which allowed for different mixtures of growth patterns that could better explain the likelihood of states enacting GSLs and NAL combinations. Prior research has documented substantial variation in the overdose trends across the United States (Cooper et al., 2020). Of particular importance to this analysis, heroin and fentanyl markets spread from distribution hub cities out to rest the country (DEA, 2019; O’Connor, 2018). Specifying a county-level random slope allowed us to obtain unbiased estimates in the context of heterogeneous treatment effects across counties, thus avoiding aggregation bias (Gibbons, Suárez Serrato & Urbancic, 2018). This allowed us to directly model different growth patterns within and across states, thus obviating the need for a parallel trends assumption.
We hypothesize that it takes time to see the impact of enactment because GSLs rely on law enforcement and the general public to become informed of the new law and modify their behavior accordingly. To account for this potential delay in policy uptake, year of and two years of linear-distributed lags (three years of observations) were included in the models for the measure of (1) GSL arrest with an active NAL, and (2) GSL charge or other protections and a NAL. Only two years of lags after year of enactment were included in the models as this was the maximum number of years we could follow the law’s impact with sufficient numbers of states to be well supported within the model. Distributed lags were not included in measuring the effect of any GSL in the absence of a NAL because only one state had this combination for over two years between 2013–2018. NAL was the secondary exposure of this analysis so for model parsimony, we also did not include distributed lags for states which had a NAL but no GSL. The covariates detailed in the section above were all modeled as concurrent predictors of overdose deaths.
All models present estimated posterior medians and credible intervals (CI), and estimates are interpreted as adjusted relative rates based on the exponentiated medians and CI (DiMaggio, 2014). All model parameters were assigned non-informative priors, centered on zero but with very high variance. We present the model’s mathematical formula, and details of how it was specified, in the supplemental materials. The models were run using the R-INLA packages within R (Rue, 2020).
Sensitivity Analyses
We conducted two sensitivity analyses on all three fatal overdose outcomes. First, we conducted our analyses excluding states that exceeded a threshold of 5% absolute difference in reported versus imputed opioid overdose rates based on Ruhm’s (2017) study that created corrected rates based on imputed county-level overdose rates when no specific drug was identified (i.e., Alabama, Indiana, Louisiana, and Pennsylvania). This sensitivity test was used to examine the bias deriving from misidentified or unidentified type of overdose based on ICD-10 coded death certificate data. Second, we ran our models excluding two states that had GSLs with more limited legal protections than charge or prosecution: Utah and Virginia. In these two states the legal protections offered “an affirmative defense” for an allegation of an offense committed in course of contacting emergency services (PDAPS, 2018b). This analysis addressed the potential bias of including these weaker protections along with protections from charge or prosecution.
Results
By July 2018, 45 states and DC had a Good Samaritan law, 22 of which provided protection against arrest and 24 of which protected against charge, prosecution or other protections, and all states had a NAL. Of the 46 jurisdictions with GSLs, 36 enacted the GSL during the 2013–2018 period. The vast majority of states began the 2013–2018 period with either no GSL or only GSLs that protected from charge or other protections. Between 2013 and 2018 states typically enacted their GSL within two years of enacting a NAL (21 states enacted within a year, 8 within 2 years). Where GSLs and NALs were enacted in different years, most states enacted their NAL first; only 2% of the total state-years between 2013–2018 had a GSL but no NAL, mostly comprised of states that had a GSL but no NAL for less than a full calendar year. Supplementary Table S1 presents the dates of enactment for all GSL with arrest protections, GSL within charge or other protection and any NAL (PDAPS, 2017; PDAPSb, 2018).
We present descriptive statistics for these models in Table 1. During the 2013- July 2018 time period, on average, 18.5 people died of an any kind of overdose per county (with counties ranging from 0–1337 deaths). For the secondary outcomes of opioid overdoses and heroin or synthetic overdoses, there were on average 12 opioid overdoses per county and 8.5 overdoses per county attributed to heroin or synthetic overdoses. The addition of the CAR random effect proved very important in all three models as 92% of residual error (RE) variance was due spatial autocorrelation in the all fatal overdose model, 91% in the opioid overdose model, and 86% in the heroin/synthetics.
Table 1:
Descriptive summary of county-level demographic characteristics and mortality outcomes, 2013–2018, n =3109 counties
| Mean | SD* | Min | Max | |
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Percent age 0–19 years | 27.8 | 5.6 | 0.0 | 71.4 |
| Percent age 20–24 years | 6.9 | 1.0 | 0.0 | 14.9 |
| Percent age 25–44 years | 24.1 | 3.3 | 0.0 | 48.8 |
| Percent age 45–64 years | 23.9 | 3.5 | 0.0 | 41.1 |
| Percent male | 49.4 | 2.2 | 30.3 | 100.0 |
| Percent White | 71.0 | 20.9 | 0.0 | 98.5 |
| Percent Black | 8.6 | 15.3 | 0.0 | 91.7 |
| Percent Hispanic | 7.9 | 13.9 | 0.0 | 95.3 |
| Percent families in poverty | 14.2 | 7.5 | 0 | 61.3 |
| Median household income (x $10,000) | 4.8 | 1.4 | 1.9 | 13.3 |
| Percent unemployed | 6.4 | 5.1 | 0.0 | 67.3 |
| Population density (thousands per sq. mile) | 0.2 | 1.3 | 0.0 | 50.9 |
| All mortality (per 1000 population) | 9.0 | 3.8 | 0 | 125 |
| Overdose Mortality Outcomes | ||||
| All overdose deaths | 18.5 | 60.36 | 0.0 | 1337 |
| Opioid overdose deaths | 12.01 | 42.9 | 0.0 | 1145.0 |
| Heroin and synthetic overdose deaths | 8.0 | 34.3 | 0.0 | 1022 |
Standard deviation
Effects of Good Samaritan Laws and Naloxone Access Laws on Overdose Mortality
Table 2 presents the estimated impact of GSLs, in conjunction with and separate of NALs, on overdose mortality. Results are presented as adjusted relative rates of overdose compared to if the state had not enacted a given law/combination of laws. Enactment of a GSL with protection against arrest (in combination with a NAL) was not associated with a reduction in overdose rates during the year of enactment, but was associated with significant reductions in rates of overdose mortality one year after enactment (3% decrease in rates; rate ratio (RR): 0.97, CI: 0.93–0.99) and two years after enactment (7% decrease in rates; RR: 0.93, CI: 0.89–0.97). This trend of increasingly lower rates of overdose was also apparent in both secondary outcome analyses. GSLs with arrest protections in combination with NALs were associated with an increase in opioid overdose mortality rates during the year of enactment (RR: 1.05, 95% CI: 1.00–1.09); however, in each subsequent year the relative rates of overdose decreased and became significantly protective in year two after enactment where all opioid overdose mortality rates had decreased by 10% (RR: 0.90; 95% CI: 0.84–0.96). Similarly in the combined heroin and synthetic opioid overdose mortality was associated with an 11% rate reduction in heroin and synthetic overdose mortality (RR: 0.89; 95% CI: 0.82–0.96) by two years after enactment.
Table 2:
Estimated adjusted relative rate of county-level overdose deaths given state enactment of Good Samaritan laws and Naloxone Access laws
| All Drug Overdose | All Opioid Overdose | All Heroin and/or Synthetic Overdose | |||||||
|---|---|---|---|---|---|---|---|---|---|
| RR | LCI | UCI | RR | LCI | UCI | RR | LCI | UCI | |
| Good Samaritan Laws Arrest Protections + Naloxone Access Law | |||||||||
| Enactment Year | 1.00 | 0.97 | 1.03 | 1.05^ | 1.0 | 1.09 | 1.06 | 0.99 | 1.12 |
| 1 Year Post-Enactment | 0.97* | 0.934 | 0.99 | 0.97 | 0.92 | 1.02 | 0.97 | 0.91 | 1.03 |
| 2 Years Post-Enactment | 0.93* | 0.89 | 0.97 | 0.90* | 0.85 | 0.95 | 0.89* | 0.82 | 0.96 |
| Good Samaritan Laws Charge or Other Protections + Naloxone Access | |||||||||
| Enactment Year | 0.98 | 0.95 | 1.01 | 0.99 | 0.95 | 1.03 | 0.97 | 0.92 | 1.02 |
| 1 Year Post-enactment | 0.97 | 0.94 | 1.01 | 1.00 | 0.95 | 1.05 | 0.98 | 0.92 | 1.05 |
| 2 Years Post-enactment | 0.97 | 0.93 | 1.01 | 1.01 | 0.96 | 1.07 | 0.99 | 0.92 | 1.08 |
| Good Samaritan Law without Any Naloxone Access Law | |||||||||
| Enactment Year | 0.84* | 0.80 | 0.88 | 0.89* | 0.84 | 0.96 | .72* | .65 | .78 |
| Naloxone Access Laws without Any Good Samaritan Law | |||||||||
| Enactment Year | 0.98 | 0.95 | 1.00 | 1.02 | 0.99 | 1.06 | 0.98 | 0.94 | 1.03 |
| Residual Error (RE) due to Spatial Autocorrelation | |||||||||
| Overall model | 0.92 | 0.91 | 0.86 | ||||||
Significant decrease in relative rates of overdose
significant increase in relative rates of overdose. Rates are estimated in the year of enactment and two subsequent years (2013–2018). Models adjusted for demographic covariates and law covariates (Prescription Drug Monitoring Programs, Pain Management Clinic Laws, medical cannabis laws).
GSLs with protections from charge, prosecution, or that only provide mitigation at sentencing were not associated with overdose mortality in the year of enactment or in the subsequent two years. This finding was confirmed in the secondary analyses for opioid overdose deaths and heroin and synthetic opioid overdose deaths. The trends comparing GSLs with arrest protections combined with a NAL and GSLs with charge or other protections combined with a NAL are represented graphicly in Figures A–C.
Figures A-C.
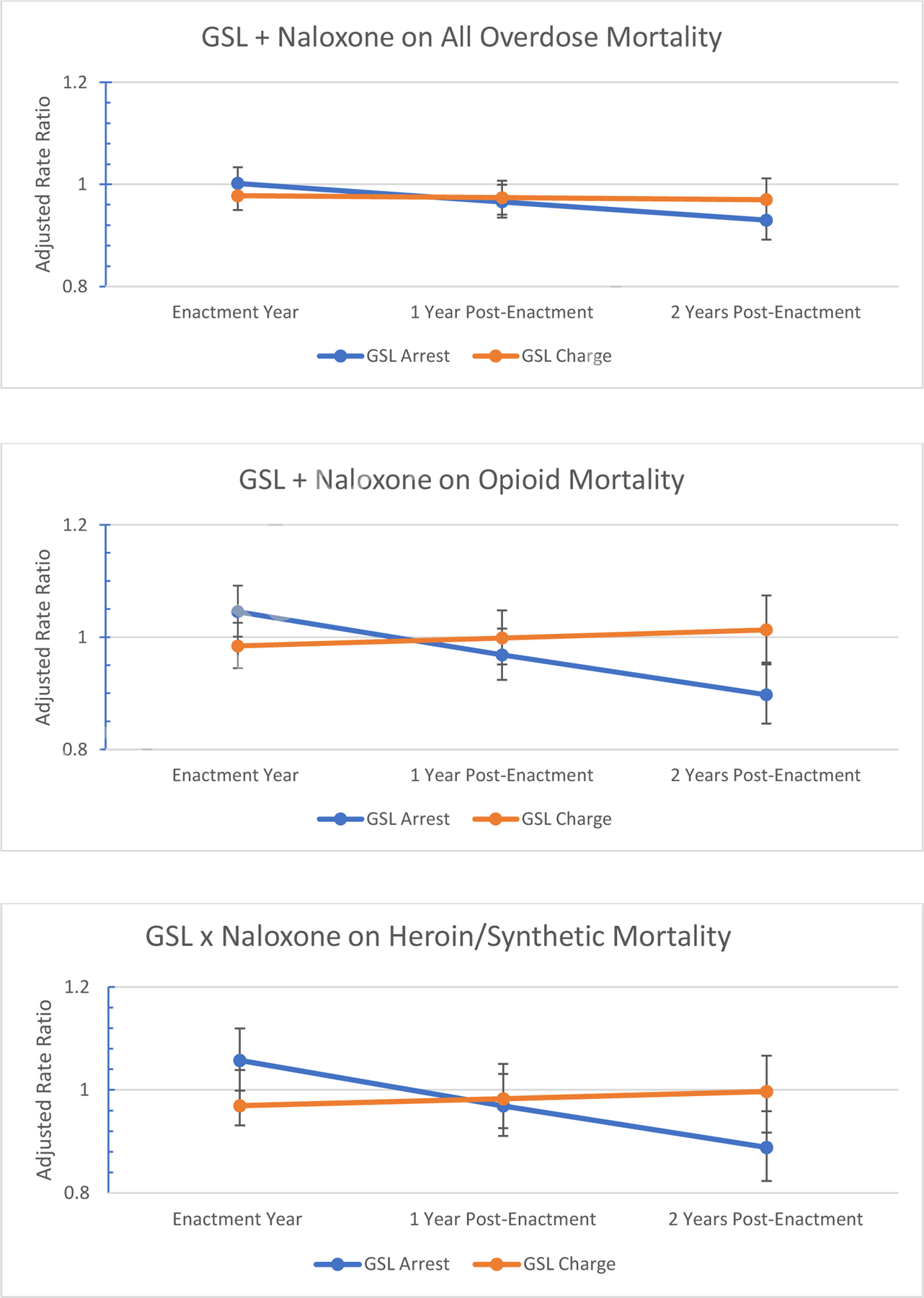
(A) Impact of GSL protection level (with an active NAL) on all overdose mortality over 3 years (2013–2018)
(B) Impact of GSL protection level (with an active NAL) on opioid overdose mortality over 3 years (2013–2018)
(C) Impact of GSL protection level (with an active NAL) on heroin and/or synthetic overdose mortality over 3 years (2013–2018)
Enactment year refers to the first year the GSL policy was in place for at least 7 months of the year. Model estimates are adjusted for both demographic and law covariates.
GSLs with either arrest or more limited protections independent of NALs were also associated with significantly lower rates of overdose deaths (RR: 0.84 :95% CI: 0.80–0.88), opioid overdose deaths (RR: 0.90 :95% CI: 0.84–0.96), and heroin and synthetic opioid overdose deaths (RR: 0.71 :95% CI: 0.65–0.78).
Sensitivity Analyses
Both sensitivity analyses produced substantively similar results to our primary and secondary analyses. Results from the first sensitivity test are presented in Supplementary Table S2. Removal of four states where there were substantial underestimates in drug type identification in fatal overdoses were mostly unchanged from the primary and secondary analyses. Results from the second sensitivity test removing two states which had very limited GSL legal protections were also largely unchanged (see Supplementary Table S3).
Discussion
This study suggests two main conclusions regarding the impact of overdose Good Samaritan laws on fatal overdoses. First, the type of legal protections offered by a GSL matter and second, the impacts of GSLs generally do not appear until one to two years after enactment. By two years after enactment, GSLs with protections from arrest in conjunction with a NAL were associated with a 7% lower rates for all overdose fatalities. Secondary analyses examining opioid fatalities and heroin and synthetic opioid fatalities specifically had even larger reductions in rates of overdose associated with this combination of laws as compared to had the state not enacted this particular combination of laws. Although GSLs (including either arrest or charge protections) did appear to have an impact separate from NALs, very few states had a GSL but not an NAL, and typically they transitioned to having both a NAL and GSL within approximately one year. Given the limits of this measure, this GSL-only finding should be interpreted cautiously.
The findings that legal protections from arrest have a significant 2-year lagged impact on overdose deaths, but legal protections from charge, prosecution, or mitigation at sentencing do not, may help us understand the mixed results of previous national-level analyses (Atkins et al., 2019; McClellan et al., 2018; Rees et al., 2017). Two of these previous studies did not find significant effects of GSLs on overdose mortality but they did not include legal protection or time effects in their analyses (Atkins et al., 2019; Rees et al., 2017). The McClellan and colleagues study did examine legal protections, but found no significant differences between laws with the two types of protection; however, they did not examine lagged effects, and their analysis period ended in 2014, right as the fentanyl epidemic was beginning and before many states had enacted GSLs with arrest protections (McClellan et al., 2018).
GSLs that protect from arrest (as opposed to protection from charge/prosecution or mitigation at sentencing) may be more effective in reducing fear about contacting emergency services and may facilitate salutatory interactions with emergency medical personnel or with police who see their priority in an overdose as providing urgent care, as opposed to law enforcement. Fear of law enforcement is common among people who use drugs (Baca & Grant, 2007; Pollini et al., 2006). One study of Colorado’s GSL during the years when it only protected from prosecution, found that people who were trained on overdose response would rarely call for emergency assistance because they felt that they would end up arrested based on other reasons (violations of supervision/outstanding warrants etc.) and felt that local law enforcement was often very aggressive in their interactions with people who use drugs (Koester, Mueller, Raville, Langegger, & Binswanger, 2017). Further comparative studies that examine the differences in experiences of people who contact emergency services in jurisdictions that have GSLs protecting from arrest and GSLs that do not are warranted to better understand the mechanisms by which this difference in legal protections may impact overdose responses.
The delayed nature of the decreasing rates of overdose is supported by previous regional studies which found that most people are not aware of, or have limited knowledge of, their local GSL (Evans et al., 2016; Latimore & Bergstein, 2017; Schneider, Park, Allen, Weir, & Sherman, 2020). GSL effectiveness relies on the public and emergency service buy-in. The first step of this is ensuring that people know and understand the scope of their state GSL. Other studies have shown that after overdose rescue training and education, including on GSLs, people are more likely to contact emergency services (Jakubowski et al., 2018). Secondly, the implementation of GSLs need to be consistent with the law to build trust among the people who may be in the position where they need to respond to an overdose. Previous analysis of state GSLs have found that police did not always implement GSLs consistent with their states’ laws (Banta-Green et al., 2013; Koester et al., 2017). Current GSLs, even those that provide protection from arrest, are still quite limited, which may make even people who know about them hesitant to call for assistance, as they may still be arrested or charged for other offenses or outstanding warrants (Koester et al., 2017). As most GSLs provide extremely limited protections from arrest and charge/prosecution, it is possible that further broadening their scope may also improve their effectiveness. Future research on strategies for increasing the speed and scope of dissemination of GSL information, and fostering community trust in GSLs could prove useful in decreasing overdose fatalities.
This study also found that GSLs without a NAL appeared to reduce overdose; however, this was based on a very small (2%) portion of state-years, deriving from six states (DE, FL, CO, IN, LA, MD), most of which only had this law combination for less than one calendar year. More in-depth examination of the state contexts (scope of fentanyl crisis, other components of local GSL laws, or other policies, etc.) during the years where there was only a GSL in effect, could be helpful in identifying why this law was ostensibly related to lower rates of overdose. One possible explanation is that all of the state-years with only a GSL were concentrated around the start of the fentanyl epidemic, prior to the sharpest curve of the epidemic which is largely attributed to fentanyl. Only two of six states saw a significant increase in overdose deaths during the time where they had only a GSL, and this was only the case for approximately half a year (Rudd, Aleshire, Zibbell, & Gladden, 2016). Only one of these states (MD) had a statistically significant increase in overdose deaths specifically attributed to synthetic opioid overdose in these years, again only for just over half a year (Scholl et al., 2018).
This study is not without limitations. Overdose death data rely on ICD-10 code classification of reason for death, which may mean some data is misclassified or under-identified within the dataset (Ruhm, 2017). However, the consistent patterns across all overdose, opioid overdose and heroin/synthetic opioid overdoses suggest robustness of these findings. Furthermore, these models were consistent with the sensitivity analysis removing the four states with the poorest quality data (Alabama, Indiana, Louisiana, and Pennsylvania). Second, as an observational study, these findings are correlative, although attempts were made to control for major county-level characteristics and key policies with the potential to impact opioid overdoses. Third, this study only examined one key provision of GSLs: legal protections. GSLs have other dimensions of heterogeneity that may impact their effectiveness, and their ‘on the ground’ implementation may also impact their effectiveness. Further research is needed on the impact of existing provisions, and on state-specific implementation of GSLs. GSLs with arrest protections are relatively new, and as such, we were only able to examine three years of law maturation (year of enactment and two years afterward). Extending this time period may provide more detailed information on how mature GSL policies may influence overdose rates.
In conclusion, GSLs that have legal protections from arrest in combination with NALs are associated with lower overdose mortality rates by two years after enactment for all overdoses, opioid-related overdoses and heroin/synthetic opioid-related overdoses. While further research is needed to understand how to increase GSL effectiveness, GSLs with arrest protections appear to be a more effective means of decreasing overdose fatality rates, and specifically overdose fatalities associated with the fentanyl epidemic, than those with less broad legal protections. In the current wave of the opioid crisis, where many more overdose deaths are attributed to illicit supply opioids including heroin and fentanyl, effective use of these harm reduction-oriented policies appears to be a helpful strategy in combatting preventable overdose mortality.
Supplementary Material
Funding:
This work was supported by the National Institute on Drug Abuse [R01DA045872]
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of interests: none
Alaska was excluded from the analysis due to multiple changes in county boundaries during the study time frame.
By July 1 2017, all states had some form of NAL in effect, and the authors confirmed that no states removed their NAL in 2018.
Bibliography
- Ahmad F, Rossen L, & Sutton P (2020). NVSS- Vital Statistics Rapid Release - Provisional Drug Overdose Death Counts. Retrieved October 14, 2020, from National Center for Health Statistics website: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
- Atkins DN, Durrance CP, & Kim Y (2019). Good Samaritan harm reduction policy and drug overdose deaths. Health Services Research, 54(2), 407–416. 10.1111/1475-6773.13119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baca CT, & Grant KJ (2007). What heroin users tell us about overdose. Journal of Addictive Diseases, 26(4), 63–68. 10.1300/J069v26n04_08 [DOI] [PubMed] [Google Scholar]
- Banta-Green CJ, Beletsky L, Schoeppe JA, Coffin PO, & Kuszler PC (2013). Police officers’ and paramedics’ experiences with overdose and their knowledge and opinions of Washington state’s drug overdosenaloxonegood samaritan law. Journal of Urban Health, Vol. 90, pp. 1102–1111. 10.1007/s11524-013-9814-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beletsky L, & Davis CS (2017). Today’s fentanyl crisis: Prohibition’s Iron Law, revisited. International Journal of Drug Policy, 46, 156–159. 10.1016/j.drugpo.2017.05.050 [DOI] [PubMed] [Google Scholar]
- Bernardinelli L, Clayton D, Pascutto C, Montomoli C, Ghislandi M, & Songini M (1995). Bayesian analysis of space—time variation in disease risk. Statistics in Medicine, 14(21–22), 2433–2443. 10.1002/sim.4780142112 [DOI] [PubMed] [Google Scholar]
- Bertrand M, Duflo E, & Mullainathan S (2004). How much should we trust differences-in-differences estimates? The Quarterly Journal of Economics, 119(1), 249–275. 10.1162/003355304772839588 [DOI] [Google Scholar]
- Besag J, York J, & Mollié A (1991). Bayesian image restoration, with two applications in spatial statistics. Annals of the Institute of Statistical Mathematics, 43(1), 1–20. 10.1007/BF00116466 [DOI] [Google Scholar]
- Blangiardo M, & Cameletti M (2015). Spatial and Spatio-temporal Bayesian Models with R - INLA | Wiley. [Google Scholar]
- Britannica ProCon.org. (n.d.). Legal Medical Marijuana States and DC - Medical Marijuana. Retrieved December 10, 2020, from https://medicalmarijuana.procon.org/legal-medical-marijuana-states-and-dc/#Alaska
- CDC Health Alert Network. (2020). HAN00438. Retrieved from https://emergency.cdc.gov/han/2020/han00438.asp
- Cerdá M, Krawczyk N, Hamilton L, Rudolph KE, Friedman SR, & Keyes KM (2021). A critical review of the social and behavioral contributions to the overdose Epidemic. Annual Review of Public Health, 42(1). 10.1146/annurev-publhealth-090419-102727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper RL, Thompson J, Edgerton R, Watson j., MacMaster SA, Kalliny M, Huffman MN, Juarez P, Mathews-Juarez P, Tabatabai M, Singh KP (2020). Modeling dynamics of fatal opioid overdose by state and across time.Preventive Medicine Reports. doi: 10.1016/j.pmedr.2020.101184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis C, & Carr D (2017, April 1). State legal innovations to encourage naloxone dispensing. Journal of the American Pharmacists Association, Vol. 57, pp. S180–S184. 10.1016/j.japh.2016.11.007 [DOI] [PubMed] [Google Scholar]
- Drug Enforcement Agency. (2019). National Drug Threat Assessment. Retrieved from https://www.dea.gov/sites/default/files/2020-01/2019-NDTA-final-01-14-2020_Low_Web-DIR-007-20_2019.pdf
- DiMaggio C (2014). Spatial Epidemiology Notes Applications and Vignettes in R.
- Evans TI, Hadland SE, Clark MA, Green TC, & Marshall BDL (2016). Factors associated with knowledge of a Good Samaritan Law among young adults who use prescription opioids non-medically. Harm Reduction Journal, 13(1), 24. 10.1186/s12954-016-0113-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geolytics Inc. (2018). Geolytics Estimates Premium [data DVD]. East Bruswick, NJ. [Google Scholar]
- Giglio RE, Li G, & DiMaggio CJ (2015). Effectiveness of bystander naloxone administration and overdose education programs: a meta-analysis. Injury Epidemiology, 2(1), 1–9. 10.1186/s40621-015-0041-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedegaard H, Miniño AM, & Warner M (2020a). Drug Overdose Deaths in the United States, 1999–2018 Key findings Data from the National Vital Statistics System, Mortality. Retrieved from https://www.cdc.gov/nchs/products/index.htm.
- Hedegaard H, Miniño AM, & Warner M (2020b). Drug Overdose Deaths in the United States, 1999–2019. Retrieved from https://www.cdc.gov/nchs/products/index.htm. [PubMed]
- Horwitz JR, Davis C, McClelland L, Fordon R, & Meara E (2020). The importance of data source in prescription drug monitoring program research. Health Services Research, 1475-6773.13548. 10.1111/1475-6773.13548 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jakubowski A, Kunins HV, Huxley-Reicher Z, & Siegler A (2018). Knowledge of the 911 Good Samaritan Law and 911-calling behavior of overdose witnesses. Substance Abuse, 39(2), 233–238. 10.1080/08897077.2017.1387213 [DOI] [PubMed] [Google Scholar]
- Kerensky T, & Walley AY (2017, December 19). Opioid overdose prevention and naloxone rescue kits: What we know and what we don’t know. Addiction Science and Clinical Practice, Vol. 12, p. 4. 10.1186/s13722-016-0068-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koester S, Mueller SR, Raville L, Langegger S, & Binswanger IA (2017). Why are some people who have received overdose education and naloxone reticent to call Emergency Medical Services in the event of overdose? International Journal of Drug Policy, 48, 115–124. 10.1016/j.drugpo.2017.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Latimore AD, & Bergstein RS (2017). “Caught with a body” yet protected by law? Calling 911 for opioid overdose in the context of the Good Samaritan Law. International Journal of Drug Policy, 50, 82–89. 10.1016/j.drugpo.2017.09.010 [DOI] [PubMed] [Google Scholar]
- Martins SS, Ponicki W, Smith N, Rivera-Aguirre A, Davis CS, Fink DS, … Cerdá M (2019). Prescription drug monitoring programs operational characteristics and fatal heroin poisoning. International Journal of Drug Policy, 74, 174–180. 10.1016/j.drugpo.2019.10.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClellan C, Lambdin BH, Ali MM, Mutter R, Davis CS, Wheeler E, … Kral AH (2018). Opioid-overdose laws association with opioid use and overdose mortality. Addictive Behaviors, 86, 90–95. 10.1016/j.addbeh.2018.03.014 [DOI] [PubMed] [Google Scholar]
- National Center for Health Statistics. (2018). Detailed Mortality- All county files 2013–2018 as compiled from data provided by the 57 vital statistics jursidictions through the Vital Statistics Cooperative Program.
- O’Connor S (2018). Fentanyl Flows from China: An Update since 2017. U.S.-China Economic and Security Commission. Retieved from https://www.uscc.gov/sites/default/files/Research/Fentanyl%20Flows%20from%20China.pdf
- Pacula RL, & Powell D (2018). A supply-side perspective on the opioid crisis. Journal of Policy Analysis and Management, 37(2), 438–446. 10.1002/pam.22049 [DOI] [Google Scholar]
- PDAPS. (2018a). Prescription Drug Abuse Policy System:Pain Management Clinic Laws. Retrieved September 23, 2020, from http://pdaps.org/datasets/pain-management-clinic-laws
- PDAPS. (2018b). Prescription Drug Abuse Policy System: Good Samaritan Overdose Prevention Laws. Retrieved May 1, 2020, from http://pdaps.org/datasets/good-samaritan-overdose-laws-1501695153
- PDAPS. (2017). Prescription Drug Abuse Policy System: Naloxone Overdose Prevention Laws. Retrieved May 1, 2020, from http://pdaps.org/datasets/laws-regulating-administration-of-naloxone-1501695139
- Pitt AL, Humphreys K, & Brandeau ML (2018). Modeling health benefits and harms of public policy responses to the US opioid epidemic. American Journal of Public Health, 108(10), 1394–1400. 10.2105/AJPH.2018.304590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollini RA, McCall L, Mehta SH, Celentano DD, Vlahov D, & Strathdee SA (2006). Response to overdose among injection drug users. American Journal of Preventive Medicine, 31(3), 261–264. 10.1016/j.amepre.2006.04.002 [DOI] [PubMed] [Google Scholar]
- Rees D, Sabia J, Argys L, Latshaw J, & Dave D (2017). With a little help from my friends: The effects of Naloxone Access and Good Samaritan Laws on opioid-related deaths. National Bureau of Economic Research. 10.3386/w23171 [DOI] [Google Scholar]
- Rudd RA, Aleshire N, Zibbell JE, & Gladden RM (2016). Increases in Drug and Opioid Overdose Deaths — United States, 2000–2014. Morbidity and Mortality Weekly Report (MMWR), 64(50), 1378–1382. Retrieved from https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6450a3.htm#tab [DOI] [PubMed] [Google Scholar]
- Rue H (2020). The R-INLA project. Retrieved September 22, 2020, from http://www.r-inla.org/
- Ruhm CJ (2017). Geographic variation in opioid and heroin involved drug poisoning mortality rates. American Journal of Preventive Medicine, 53(6), 745–753. 10.1016/j.amepre.2017.06.009 [DOI] [PubMed] [Google Scholar]
- Schneider KE, Park JN, Allen ST, Weir BW, & Sherman SG (2020). Knowledge of Good Samaritan Laws and beliefs about arrests among persons who inject drugs a year after policy change in Baltimore, Maryland. Public Health Reports, 135(3), 393–400. 10.1177/0033354920915439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scholl L, Seth P, Kariisa M, Wilson N, & Baldwin G (2018). Drug and Opioid-Involved Overdose Deaths — United States, 2013–2017. MMWR. Morbidity and Mortality Weekly Report, 67(5152), 1419. 10.15585/mmwr.mm675152e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smart R, Pardo B, & Davis CS (2020). Systematic review of the emerging literature on the effectiveness of naloxone access laws in the United States. Addiction, add.15163. 10.1111/add.15163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waller LA, & Gotway CA (2004). Applied Spatial Statistics for Public Health Data. 10.1002/0471662682 [DOI]
- Watson DP, Ray B, Robison L, Huynh P, Sightes E, Walker LS, … Duwve J (2018). Lay responder naloxone access and Good Samaritan law compliance: Postcard survey results from 20 Indiana counties. Harm Reduction Journal, 15(1). 10.1186/s12954-018-0226-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Word Health Organization. (2014). Community management of opioid overdose. Retrieved from https://www.who.int/publications/i/item/9789241548816 [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.