
Figure 4.
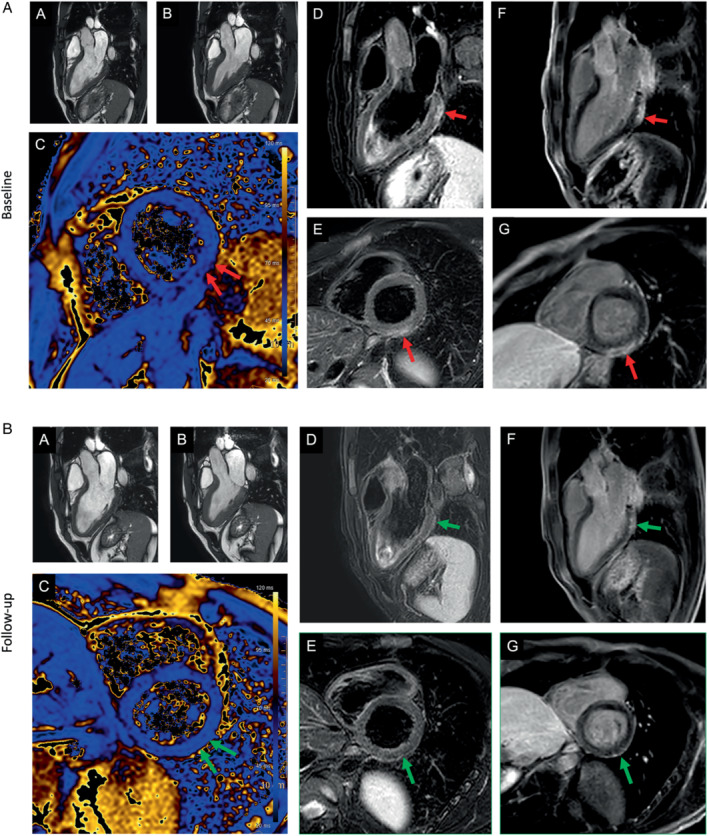
(A) Patient with signs of a myocarditis after mRNA SARS‐CoV‐2 vaccination with Comirnaty (Pfizer‐BioNTech). Three days after the second dose of the vaccine, the patient presented to the emergency room of a referring hospital with chest pain and discomfort, shortness of breath, and decreased exercise capacity. High‐sensitivity troponin T level was elevated at 380 ng/L; N‐terminal pro‐B‐type natriuretic peptide 250 ng/L (<88). Cardiac magnetic resonance (CMR) demonstrated normal left and right ventricular ejection fraction (A, B), with reduced global longitudinal strain. T2‐weighted images indicated a regional oedema inferior/inferolateral (basal) (in D, E) with corresponding elevated quantitative myocardial T2‐mapping parameters (C) and corresponding subepicardial focal late gadolinium enhancement (F, G). (B) The findings at baseline (indicated by red arrow) resolved almost completely (small epicardial fibrosis inferolateral basal) at 4‐month CMR follow‐up (second figure – green arrow). Full description of this case can be found in Jahnke et al. 65