
Figure 7.
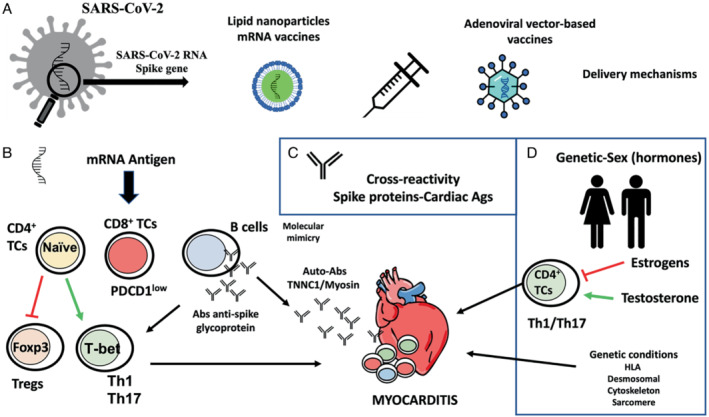
Potential molecular mechanisms for the development of myocarditis following vaccines against COVID‐19. (A) COVID‐19 vaccines are developed from the modified SARS‐CoV‐2 Spike gene. The mRNA vaccines are introduced via lipid nanoparticles, while the adenoviral vector‐based vaccines deliver the Spike sequence as a codon‐optimized DNA. (B) The mRNA can act as an antigen, so it can be recognized by the immune system and activate specific responses of the adaptive immune system. Some of these responses are capable of activating cardiotropic clones of T and B cells triggering cardiac inflammation. (C) Molecular mimicry between Spike glycoprotein and myosin heavy chain or troponin C1, may trigger cross‐reactivity between IgM antibodies against SARS‐CoV‐2 Spike glycoprotein and cardiac autoantigens and potentially induce myocardial inflammation. (D) Development of SARS‐CoV‐2 vaccine myocarditis is associated with young men, suggesting a role for sex hormones. Testosterone activates specific T helper cell responses, whereas oestrogen inhibits pro‐inflammatory T‐cell responses. In addition, viral myocarditis is associated with genetic variants of genes encoding for different HLA factors and structural proteins of the heart.