
FIGURE 1.
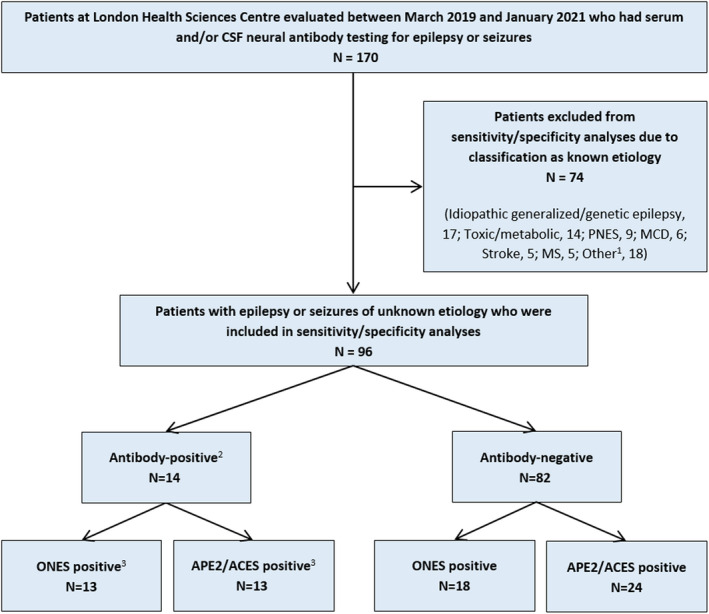
Identification of patients for inclusion in specificity/sensitivity analyses and their classifications. 1Other known etiologies included Rasmussen encephalitis (n = 3), vasculitis (n = 2), neurodegenerative (n = 2), infectious (n = 2), developmental/epileptic encephalopathy (n = 2), posterior reversible encephalopathy syndrome (n = 2), posttraumatic (n = 1), cavernous malformation (n = 1), glioma (n = 1), delayed radiation‐induced leukoencephalopathy (1), and chronic‐appearing frontal lesion not otherwise specified (n = 1). 2Only patients with true‐positive neural antibody results (see text) were classified as neural antibody‐positive for sensitivity/specificity analyses. True‐positive neural antibody results consisted of anti‐leucine‐rich glioma‐inactivated 1 (n = 5), anti‐glutamic acid decarboxylase 65 (GAD65; n = 3), anti‐myelin oligodendrocyte glycoprotein (n = 2), anti‐contactin‐associated protein‐like 2 (CASPR2; n = 2), anti‐N‐methyl‐D‐aspartate receptor (n = 1), and unclassified neural‐specific antibody (n = 1). False‐positive neural antibody results (classified as neural antibody‐negative for sensitivity/specificity analyses) consisted of isolated weak serum positivity for anti‐CASPR2 (n = 2). 3One anti‐GAD65 patient who was negative by both the “Obvious” indications for Neural antibody testing in Epilepsy or Seizures (ONES) checklist and the Antibody Prevalence in Epilepsy and Encephalopathy (APE2)/Antibodies Contributing to Focal Epilepsy Signs and Symptoms (ACES) reflex score is described in the text. CSF, cerebrospinal fluid; MCD, malformation of cortical development; MS, multiple sclerosis; PNES, psychogenic nonepileptic seizures