
Figure 5.
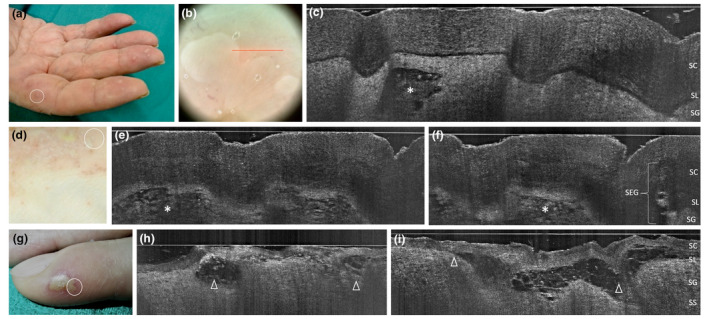
Palmoplantar pustulosis in two women aged 58 (a‐c) and 39 years (d‐f): clinical, dermoscopic and LC‐OCT appearance of early developed lesions of the fingers; LC‐OCT examination of a tiny recently developed pustule demonstrates an upper‐epidermal area with well‐defined borders and hyper‐reflective roundish structures corresponding to neutrophils (c, asterisk), while examination of 7‐days pustules of the plantar surface demonstrate multilocular spongiform hyporeflective areas with less‐defined borders, filled with neutrophils (e,i, asterisks) and preserved SEG. Comparison with an herpetic whitlow case of a 45‐year‐old female (g‐i): multilobated vesico‐pustules are subcorneal, with cleavage level at SL (h,i, triangles), borders are ill‐defined, and the content is not homogenous (hyper‐reflective ridge made of branches of intercellular material, floating little roundish structures corresponding to necrotic keratinocytes) as a result of viral cytopathic effect. [SC, stratum corneum; SL, stratum lucidum; SG, stratum granulosum; SEG, sweat eccrine gland. The red line inside polarized dermoscopy 15× (b) corresponds to the LC‐OCT vertical frame].