

Abstract
Background
Canine atopic dermatitis (cAD) is an allergic skin disease affecting approximately 10% of dogs. allergen‐specific immunotherapy (ASIT) is currently the only treatment option able to induce tolerance to the causative allergens.
Objective
To retrospectively establish the efficacy of ASIT in atopic dogs.
Animals
Client‐owned (n = 664) dogs with cAD presented between 2008 and 2018 to two dermatology referral clinics.
Materials and Methods
Clinical records of atopic dogs were reviewed to obtain information including the results of the intradermal skin test and/or allergen‐specific immunoglobulin (Ig)E serological results, the allergens included in the ASIT, concurrent symptomatic medications, and ASIT efficacy after at least 9 months.
Results
Excellent (ASIT alone controlled clinical signs), good (≥50% reduction of clinical signs) and poor (<50% improvement) responses were seen in 31.5%, 28.5% and 40.1% of the dogs, respectively. No significant differences in efficacy were associated with breed, sex, age at initiation of ASIT, type of allergens in ASIT, and between clinics. Dogs re‐examined regularly responded significantly better to ASIT than dogs that did not (>50% improvement in 69.3% and 55.4% of the dogs, respectively). Dogs treated with ASIT and concomitant systemic glucocorticoids showed a significantly poorer response (success rate of >50% improvement of 38.5%).
Conclusions and clinical importance
In 59.9% of atopic dogs, subcutaneous ASIT can improve clinical signs by ≥50%. The beneficial effect of ASIT is higher if dogs are re‐examined regularly and if systemic long‐term corticosteroids are avoided, at least during the first 9 months of ASIT.
Background –Canine atopic dermatitis (cAD) is an allergic skin disease affecting approximately 10% of dogs. Allergen immunotherapy (AIT) is currently the only treatment option able to induce tolerance to the causative allergens. Objective – To retrospectively establish the efficacy of AIT in atopic dogs. Conclusions and clinical importance – In 59.9% of atopic dogs, subcutaneous AIT can improve clinical signs by ≥50%. The beneficial effect of AIT is higher if dogs are re‐examined regularly and if systemic long‐term corticosteroids are avoided, at least during the first 9 months of AIT.

Résumé
Contexte – La dermatite atopique canine (DAC) est une maladie cutanée allergique qui touche environ 10 % des chiens. L'immunothérapie allergénique (ASIT) est actuellement la seule option thérapeutique capable d'induire une tolérance aux allergènes responsables.
Objectif – Établir rétrospectivement l'efficacité de l'ASIT chez les chiens atopiques.
Animaux – Chiens de clients (n = 664) atteints de DAC présentés entre 2008 et 2018 à deux cliniques de référé en dermatologie.
Méthodes ‐ Les dossiers cliniques des chiens atopiques ont été examinés pour obtenir des informations, notamment les résultats du test cutané intradermique et / ou les résultats sérologiques de l'immunoglobuline (Ig) E spécifique d’allergène, les allergènes inclus dans l'ASIT, les médicaments symptomatiques concomitants et l'efficacité de l'ASIT après au moins neuf mois.
Résultats – Des réponses excellentes (signes cliniques contrôlés par l'ASIT seul), bonnes (réduction ≥ 50 % des signes cliniques) et médiocres (amélioration < 50 %) ont été observées chez 31,5 %, 28,5 % et 40,1 % des chiens, respectivement. Aucune différence significative d'efficacité n'a été associée à la race, au sexe, à l'âge au début de l'ASIT, au type d'allergènes dans l'ASIT et entre les cliniques. Les chiens réexaminés régulièrement ont répondu significativement mieux à l'ASIT que les chiens qui ne l'ont pas fait (amélioration > 50 % chez 69,3 % et 55,4 % des chiens, respectivement). Les chiens traités avec l'ASIT et des glucocorticoïdes systémiques concomitants ont montré une réponse significativement plus faible (taux de réussite > 50 % d'amélioration de 38,5 %).
Conclusions et importance clinique – Chez 59,9 % des chiens atopiques, l'ASIT sous‐cutanée peut améliorer les signes cliniques de ≥ 50 %. L'effet bénéfique de l'ASIT est plus élevé si les chiens sont réexaminés régulièrement et si les corticostéroïdes systémiques à long terme sont évités, au moins pendant les neuf premiers mois de l'ASIT.
Resumen
Introducción‐ la dermatitis atópica canina (cAD) es una enfermedad alérgica de la piel que afecta aproximadamente al 10 % de los perros. La inmunoterapia con alérgenos (ASIT) es actualmente la única opción de tratamiento capaz de inducir tolerancia a los alérgenos causantes.
Objetivo‐ establecer retrospectivamente la eficacia de ASIT en perros atópicos.
Animales‐ perros de propietarios particulares (n=664) con cAD presentados entre 2008 y 2018 a dos clínicas de referencia de dermatología.
Métodos‐ se revisaron las historias clínicas de los perros atópicos para obtener información, incluidos los resultados de la prueba cutánea intradérmica y/o los resultados serológicos de la inmunoglobulina (Ig)E específica para alérgenos, los alérgenos incluidos en el ASIT, los medicamentos sintomáticos concurrentes y la eficacia del ASIT después de al menos menos nueve meses.
Resultados‐ se observaron respuestas excelentes (la ASIT sola controló los signos clínicos), buenas (≥50 % de reducción de los signos clínicos) y malas (<50 % de mejora) en el 31,5 %, 28,5 % y 40,1 % de los perros, respectivamente. No se asociaron diferencias significativas en la eficacia con la raza, el sexo, la edad al inicio de la ASIT, el tipo de alérgenos en la ASIT y entre las clínicas. Los perros reexaminados con regularidad respondieron significativamente mejor a la ASIT que los perros que no lo hicieron (>50 % de mejora en el 69,3 % y el 55,4 % de los perros, respectivamente). Los perros tratados con ASIT y glucocorticoides sistémicos concomitantes mostraron una respuesta significativamente peor (tasa de éxito de >50 % de mejora del 38,5 %).
Conclusiones e importancia clínica – En el 59,9% de los perros atópicos, la ASIT subcutánea puede mejorar los signos clínicos en ≥50%. El efecto beneficioso de la ASIT es mayor si los perros se vuelven a examinar con regularidad y si se evitan los corticosteroides sistémicos a largo plazo, al menos durante los primeros nueve meses de la ASIT.
Zusammenfassung
Hintergrund – Die atopische Dermatitis des Hundes (cAD) ist eine allergische Hauterkrankung, die etwa 10% aller Hunde betrifft. Zurzeit ist die Allergen Immuntherapie (ASIT) die einzige Behandlungsoption, die eine Toleranz gegenüber den ursächlichen Allergenen induzieren kann.
Ziel – Eine Retrospektive, um die Wirksamkeit der ASIT bei atopischen Hunden zu erfassen.
Tiere – Es wurden Hunde in Privatbesitz (n = 664) mit cAD, die zwischen 2008 und 2018 in zwei dermatologischen Überweisungskliniken vorgestellt wurden, in die Studie aufgenommen.
Methoden – Die klinischen Daten von atopischen Hunden wurden durchgesehen, um Information in Bezug auf den Intradermaltest und/oder die Allergen‐spezifischen Immunglobulin (Ig) E serologischen Ergebnisse, die Allergene, die in der ASIT inkludiert wurden, gleichzeitig verabreichte symptomatische Medikation und ASIT Effektivität nach mindestens neun Monaten zu erhalten.
Ergebnisse – Es wurde eine exzellente (ASIT allein kontrollierte die klinischen Zeichen), eine gute (≥50% Reduktion der klinischen Zeichen) bzw schlechte (<50% Verbesserung) Antwort bei 31,5%, 28,5% bzw 40,1% der Hunde gesehen. Es konnten keine signifikanten Unterschiede der Wirksamkeit im Zusammenhang mit Rasse, Geschlecht, Alter am Beginn der ASIT, Allergentypen der ASIT und zwischen den Kliniken festgestellt werden. Hunde, bei denen regelmäßig Kontrolluntersuchungen durchgeführt wurden, reagierten signifikant besser auf die ASIT als Hunde, die nicht regelmäßig kontrolliert wurden (>50% Verbesserung bei 69,3% bzw 55,4% der Hunde). Hunde, die mit ASIT und gleichzeitig mit systemischen Glukokortikoiden behandelt wurden, zeigten eine signifikant geringere Antwort (Erfolgsrate von >50% Verbesserung auf 38,5%).
Schlussfolgerungen und klinische Bedeutung – Bei 59,9% der atopischen Hunde kann die subkutane ASIT die klinischen Zeichen um ≥50% verbessern. Der günstige Effekt der ASIT ist größer, wenn Hunde regelmäßig kontrolliert werden und wenn systemische Langzeit Steroide zumindest in den ersten neun Monaten der ASIT vermieden werden.
要約
背景 ‐ 犬アトピー性皮膚炎 (cAD) は、犬の約10%が罹患するアレルギー性皮膚疾患である。アレルゲン免疫療法 (ASIT) は現在、原因アレルゲンに対する耐性を獲得することができる唯一の治療法である。
目的 – 本研究の目的は、アトピー性皮膚炎の犬におけるASITの有効性をレトロスペクティブに検証することであった。
供試動物 ‐ 2008 年から 2018 年の間に 2 つの皮膚科紹介クリニックに来院した cAD を有するオーナー所有犬 (n = 664) 。
方法 ‐ アトピー犬の臨床記録をレビューし、皮内反応の結果および/またはアレルゲン特異的免疫グロブリン (Ig)E血清学的結果、ASITに含まれるアレルゲン、同時に投与した症候性薬剤、および少なくとも9か月後のASIT効果などの情報を入手した。
結果 優 (ASIT単独で臨床症状をコントロール) 、良 (臨床症状の50%以上の減少) 、不良 (50%未満の改善) の反応がそれぞれ31.5%、28.5%、40.1%の犬で見られた。有効性については、犬種、性別、ASIT開始年齢, ASITに含まれるアレルゲンの種類、診療所間で有意差はみられなかった。定期的な再検査を行った犬は、そうでない犬に比べて有意にASITに反応した (それぞれ69.3%と55.4%で50%以上の改善) 。ASITおよび全身性グルココルチコイドを併用した犬は、有意に悪い反応を示した (50%以上の改善の成功率38.5%) 。
結論と臨床的重要性 ‐ アトピー犬の59.9%において、皮下ASITは臨床症状を50%以上改善することができる。ASITの有益な効果は、犬が定期的に再検査を受け、少なくともASITの最初の9ヶ月間は、全身的な長期コルチコステロイドを避けた場合により高くなる。
摘要
背景‐犬特应性皮炎(cAD)是一种过敏性皮肤病, 影响约10%的犬。过敏原免疫治疗(ASIT)是目前唯一能够诱导对致病过敏原耐受的治疗选择。
目的‐回顾性确定ASIT在特应性犬中的有效性。2008年至2018年间, 私家cAD犬(n = 664)在两家皮肤科转诊诊所就诊。
方法‐审核特应性犬的临床记录, 以获得信息, 包括皮内皮肤试验结果和/或过敏原特异性免疫球蛋白(Ig)E血清学结果、ASIT中包含的过敏原、伴随对症用药和至少9个月后的ASIT疗效。
结果‐分别在31.5%、28.5%和40.1%的犬中观察到极佳 (仅ASIT控制了临床体征) 、良好 (临床体征减少≥50%) 和较差 (改善 < 50%) 反应。疗效的显著差异与品种、性别、ASIT开始时的年龄、ASIT中的过敏原类型和诊所之间无关。定期复查的犬对ASIT的反应明显优于未复查的犬 (分别有69.3%和55.4%的犬改善 > 50%) 。接受ASIT和伴随全身性糖皮质激素治疗的犬显示效果显著较差 (成功率 > 50%改善38.5%) 。
结论和临床重要性‐在59.9%的特应性犬中, 皮下ASIT可使临床体征改善≥50%。如果犬定期复查, 并且如果避免长期使用全身皮质类固醇, 至少在ASIT的前9个月内, ASIT的有益作用更高。
Resumo
Contexto – A dermatite atópica canina (DAC) é uma doença alérgica que afeta aproximadamente 10% dos cães. A imunoterapia alérgeno‐específica (ASIT) é atualmente a única opção terapêutica capaz de induzir tolerância aos alérgenos causadores.
Objetivo – Estabelecer retrospectivamente a eficácia da ASIT em cães atópicos.
Animais – Cães de proprietários (664) com DAC apresentados a duas clínicas de referência em dermatologia entre 2008 e 2018.
Métodos – Os prontuários dos cães atópicos foram revisados para se obter informações incluindo os resultados dos testes intradérmicos e/ou sorológicos para anticorpos (IgE) alérgeno‐específicos, os alérgenos incluídos na ASIT, medicações sintomáticas concomitantes, e a eficácia de ASIT após um mínimo de nove meses.
Resultados – Resposta excelente (ASIT controlou os sinais clínicos sozinha), boa (redução ≥50% nos sinais clínicos) e pobre (<50% de melhora) foi observada em 31,5%, 28,5% e 40,1% dos cães, respectivamente. Não foram observadas diferenças significativas na eficácia em relação a raça, gênero, idade à iniciação da ASIT, tipo de alérgenos na ASIT e entre as clínicas. Os cães reavaliados periodicamente responderam significativamente melhor à ASIT que cães que não foram reavaliados com frequência (>50% de melhora em 69,3% e 55,4% dos cães, respectivamente). Cães tratados com ASIT e glicocorticoides sistêmicos concomitantemente demonstraram uma resposta significativamente mais pobre (a taxa de sucesso >50% ocorreu em 38,5%).
Conclusões e importância clínica – Em 59,9% dos cães atópicos, ASIT subcutânea é capaz de melhorar os sinais clínicos em ≥50%. O efeito benéfico de ASIT foi maior se os cães fossem reavaliados regularmente e se corticoides sistêmicos a longo prazo fossem evitados, ao menos durante os primeiros meses de ASIT.
INTRODUCTION
Canine atopic dermatitis (cAD) is a genetically predisposed inflammatory and pruritic skin disease with characteristic clinical features, associated with the production of immunoglobulin (Ig)E against environmental allergens. 1 Canine AD has no pathognomonic clinical signs and a definitive diagnosis therefore is based on patient history, clinical examination and the exclusion of conditions that mimic cAD. 2 The exact aetiology of cAD remains the subject of debate, although it is clear that both the immune system and the skin barrier play important roles in the pathogenesis of the disease. 3 , 4 There are multiple symptomatic treatments available for cAD, yet the only current treatment that is able to alter the course of the disease is allergen immunotherapy (ASIT). 5 , 6 During subcutaneous ASIT, gradually increasing quantities of allergen extracts are administered subcutaneously with the aim of inducing long‐lasting tolerance to the causative allergens upon subsequent exposure. 5 Successful ASIT results in modulation of T‐ and B‐cell responses, increased numbers of regulatory T‐cells and skewing of specific‐antibody isotypes from IgE to IgG, as well as inhibition of migration of eosinophils, basophils and mast cells to tissues and release of their mediators. 7 , 8 , 9 , 10 Multiple studies on the efficacy of ASIT have been conducted, with study populations ranging from 53 to 186 dogs. 11 , 12 , 13 , 14 , 15 , 16 Published success rates of subcutaneous ASIT in atopic dogs range from 51% to 64%, success being described as ≥50% improvement of clinical signs of the dog. 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 The effects of concurrent medication during ASIT have not been thoroughly evaluated. 5 The aim of the present study was retrospectively to assess the efficacy of ASIT in atopic dogs and to identify whether concurrent systemic medications (glucocorticoids, ciclosporin and oclacitinib) influenced the success rate.
MATERIALS AND METHODS
Study design
This study was a retrospective study of privately owned atopic dogs.
Dogs
Dogs diagnosed with cAD between 2008 and 2018 at the dermatology departments of either Clinic A or Clinic B were identified using the patient management systems. 2 Inclusion criteria were that atopic dogs treated with ASIT had been diagnosed by veterinarians at either one of the two referral centres (clinic A or B) and that dogs did not suffer from possible (additional) food‐induced AD. Another inclusion criterion was that an intradermal skin test (IDT) and/or allergen‐specific IgE serological test had to have been performed. Exclusion criteria were that dogs had been treated with ASIT for less than 9 months, information about the course and results of ASIT was missing, dogs died during the first 9 months of ASIT or suffered from a disease other than cAD.
Signalment, IDT results, serological test results, allergens included in the ASIT, date of first ASIT injection, concurrent medication and number of re‐examinations during the first 9 months of ASIT and the efficacy of ASIT were registered using an Excel spreadsheet (Microsoft; Seattle, WA, USA. In case of missing information within the medical record of the dog, the owner was asked to complete a questionnaire via telephone or e‐mail (see Appendix S1). In case a questionnaire was taken, owners were asked at least two questions that had already been answered by reading the patient record. In case these questions were answered incorrectly, other answers to the questionnaire were considered unreliable. Thus, in these cases, the patient files were considered incomplete and the patients were excluded from the study. In any case where information about the 9 month follow‐up period could not be retrieved, the patient was excluded from the study.
Response to ASIT after 9 months was categorised primarily based on the owners' impression (level of pruritus at the start of ASIT and after 9 months), 19 use of systemic medications, and the clinician's impression: excellent (ASIT alone controlled clinical signs and no concurrent systemic medication was needed), good (≥50% reduction of clinical signs and concurrent systemic medication) or poor (<50% improvement of clinical signs and reduction of concurrent systemic medication) (Table 1).
TABLE 1.
Response to allergen immunotherapy after 9 months was scored as poor, good or excellent
| Response rate | Definition |
| Poor | The pruritus was unchanged or there was <50% improvement in clinical signs. |
| Good | ≥50% improvement in clinical signs and ≥ 50% reduction of dosage of systemic antipruritic medication if applicable. |
| Excellent | The atopic dermatitis was controlled by immunotherapy solely and the dog did not receive any concomitant systemic medication. |
Note: Usage of topical antipruritic medication was not evaluated.
The diagnosis of cAD was confirmed based on clinical criteria and by ruling out other possible causes of pruritic skin diseases, according to the current diagnostic guidelines. 2 Atopic patients had been subjected to an IDT (Artuvetrin; Lelystad, the Netherlands) and/or an allergen‐specific IgE serological test, manufactured by either Heska (Allercept, Heska; Loveland, CO, USA) (2008–2014, Clinic A), Greer (Aller‐g‐complete, Stallergenes Greer; Boston, MA, USA) (2014–2017, Clinic A; 2008–2017, Clinic B) and Alergovet (Alergovet; Madrid, Spain) (2018, clinics A and B).
An aqueous alum‐precipitated ASIT (Artuvetrin) was administered subcutaneously. Allergens were selected for inclusion in the ASIT based on positive reactions in the IDT and/or allergen‐specific IgE serological results combined with clinical relevance. After an induction phase in which doses and injection interval were progressively increased according to the protocol used at the designated clinic, dogs received a maintenance dosage of 1.0 mL every 3–4 weeks for a minimum of 9 months (Appendix S2). Injection frequency and dose of allergen extract were adjusted to the patient's requirements in <10% of all cases.
Grouping for statistical analyses
For the analysis including breeds, breeds were categorised into groups according to the Fédération Cynologique Internationale (FCI). For the analyses of associations with age at the initiation of ASIT, dogs were grouped into different age categories: <4‐year‐old, 4–8‐year‐old and >8‐year‐old. For the analysis on the influence of the types of allergens included in ASIT, different types of mites, grasses, weeds and trees were grouped and compared to each other (Table 2). The number of allergens included in ASIT also was included in the analysis. For this analysis, the number of allergens included was categorised into four groups (ASIT with n = 1–3, 4–6, 7–9 and >9 allergens included).
TABLE 2.
All mites and grass‐, weed‐ and tree‐pollens used in allergen‐specific immunoglobulin (Ig)E serological testing, intradermal testing and allergen immunotherapy were grouped together for statistical analysis
| Mites | Dermatophagoides farinae, Acarus siro, Tyrophagus putrescentiae, Lepidoglyphus destructor, Dermatophagoides pteronyssinus |
| Grasses | Dactylis glomerata, Phleum pratense, Lolium perenne, Poa pratensis, Cynodon dactylon, Holcus lanatus, Festuca pratensis, Anthoxanthum odoratum, Avena sativa, Secale cereale, Agrostis stolonifera, Festuca eliator, Agrostis alba |
| Weeds | Artemisia vulgaris, Solidago virgaurea, Chenopodium album, Rumex acetosella, Plantago lanceolata, Ambrosia artemisiifolia, Urtica dioica, Taraxacum officinale, Brassica napus, Parietaria officinalis |
| Trees | Corylus avellana, Fagus sylvatica, Betula pendula, Salix viminalis, Platanus occidentalis, Ulmus glabra, Ulmus americana, Acer pseudoplatanus, Alnus glutinosa, Pinus sylvestris, Olea europea, Quercus robur, Populus alba, Castanea sativa |
Dogs with known medication history receiving concurrent medication during ASIT were categorised into three groups: (i) dogs that received oclacitinib during the first 9 months of ASIT; (ii) dogs that received ciclosporin; and (iii) dogs that were administered systemic glucocorticoids during ASIT. Dogs that were treated with either one of these systemic medications and also received topical treatments, antibiotics or ear‐ointments were included in the medication groups. Dogs that received none or more than one of the three types of concurrent systemic medication were excluded from this analysis.
Statistical methods
The data were analysed in python 3.9.0 using the packages NumPy 1.21.1, pandas 1.3.3, SciPy 1.7.1 and statsmodels 0.13.0. Analysis code is available on GitHub (Appendix S6).
Mean rates and 95% confidence intervals (95% CI) for the various ASIT responses were computed by modelling these as a multinomial distribution, , following Goodman. 20 Here c is the number of distinct responses (poor, good or excellent), the response rate, and the corresponding number of patients in which the response was observed.
Association was investigated between the responses to ASIT (poor, good or excellent) and a number of predictors which each were analysed in univariable analyses. The response is an ordinal variable. In case of ordinal or dichotomous predictors a Kendall's tau‐b test was used. For other nominal variables a contingency table was constructed and a Pearson's chi‐square test was performed. The latter does not account for any ordering in the response; however, we confirmed that ordinal logistic regression produced qualitatively similar results. In addition, good and excellent responses also were analysed as a combined group to allow comparison to poor responses, in which case a Pearson's chi‐square test was performed. Associations with the following eight independent variables: breed, sex, age at initiation of ASIT, types (mites, grass‐, weed‐ or tree‐pollen) and number of allergens included in the ASIT, concurrent systemic medication, veterinary referral clinic and the number of re‐examinations. Results were considered significant for p‐values < 0.05. When for a particular independent variable multiple pairwise comparisons were performed, a Bonferroni correction was applied.
To correct for potential confounding, stratified analyses also were performed. In addition, a multivariate ordinal logistic regression analysis was performed.
RESULTS
Dogs
A total of 1082 atopic dogs were identified using a computer‐aided search. Two hundred and fifty‐two (23.3%) of the dogs did not complete 9 months of ASIT, for a variety of reasons such as the diagnosis of atopic‐like dermatitis (9.0%), successful usage of antipruritic medications or financial restrictions. Another 166 dogs (15.3%) were not included in the study as a consequence of incomplete data files and/or inability to contact the owners, whereas in 69 cases the questionnaire aided in completing the data. This resulted in a total of 664 dogs. From these 664 dogs, 54.2% (n = 360) were males and 45.8% (n = 304) were females; 45% (n = 162) of the males and 68.4% (n = 208) of the females were neutered. There were 19.9%(132 of 664) cross‐bred and 80.1% (532 of 664) pure‐bred dogs included (Appendix S3). Age at initiation of ASIT was available for 643 dogs and ranged from 6 months to 12 years, with a mean of 4.08 years, median of 3.66 years, and interquartile range [2.2–5.5] years. A Shapiro–Wilk test showed that age was not normally distributed. The 10 most prevalent dog breeds are listed in Table 3. The results of allergen‐specific IgE serological tests and IDT are presented in Table 4.
TABLE 3.
Most common breeds affected by canine atopic dermatitis (prevalence >2%) in the present study
| Breed | Number of dogs | Percentage of total (n = 550) |
|---|---|---|
| Labrador retriever | 108 | 19.6% |
| French bulldog | 34 | 6.2% |
| Golden retriever | 33 | 6.0% |
| German shepherd dog | 29 | 5.3% |
| Bull terrier | 19 | 3.5% |
| Jack Russell terrier | 19 | 3.5% |
| West Highland white terrier | 17 | 3.1% |
| American Staffordshire terrier | 16 | 2.9% |
| Boxer | 14 | 2.5% |
| Staffordshire bull terrier | 14 | 2.5% |
| Shih tzu | 12 | 2.2% |
Note: Only pure‐bred dogs are included in the table.
TABLE 4.
Allergens used in the intradermal skin test and in the allergen‐specific immunoglobulin (Ig)E serological testing, and the resulting number and percentage of positive reactions
| Allergen | Intradermal skin test | Allergen‐specific IgE serological results | ||
|---|---|---|---|---|
| No. of positive reactions of dogs tested | % positive | No. of positive reactions of dogs tested | % positive | |
| Dermatophagoides farinae | 420/645 | 65.1 | 569/661 | 86.1 |
| Acarus siro | 411/645 | 63.7 | 540/661 | 81.7 |
| Tyrophagus putrescentiae | 409/645 | 63.4 | 565/661 | 85.5 |
| Lepidoglyphus destructor | 350/645 | 54.3 | 357/661 | 56.7 |
| Dermatophagoides pteronyssinus | 136/645 | 21.1 | 248/661 | 37.5 |
| Grasses | 107/645 | 16.6 | 235/661 | 35.6 |
| Weeds | 105/645 | 16.3 | 191/661 | 28.9 |
| Trees | 72/645 | 11.2 | 119/661 | 18.0 |
| Flea | 2/48 | 4.2 | 3/48 | 6.3 |
| Malassezia | 18/137 | 13.1 | 32/137 | 23.4 |
Response rate to ASIT
In total, 31.5% (209 of 664, 95% CI 27.3%–35.9%) of the dogs that completed at least 9 months of ASIT showed an excellent response. A good response was seen in 28.5% (189 of 644, 95% CI 24.5%–32.8%) of the dogs and 40.1% (266 of 664, 95% CI 35.6%–44.7%) showed a poor response after 9 months of ASIT. Combining good and excellent responders, an overall of 59.9% (398 of 664, 95% CI 55.6%–64.1%) of the total population benefited from ASIT.
The efficacy of ASIT was not influenced by breed or breed group. The relationship between gender and the efficacy of ASIT was analysed and did not result in any statistically significant outcomes (Kendall's tau‐b). There was an association neither between age at initiation of ASIT and the efficacy (Kendall's tau‐b), nor between the number or types of allergens (mites, grass‐, weed‐ or tree‐pollen) included and the efficacy of ASIT (Pearson's χ2). Atopic dogs diagnosed and treated at Clinic B (511 of 664) did not respond significantly different from dogs that were diagnosed and treated at Clinic A (153 of 664) after correcting for the number of re‐examinations (Kendall's tau‐b).
The analysis revealed that atopic dogs that were presented for regular clinical examinations and evaluation of the therapy (at least once every 3 months; 218 of 664) responded significantly better (p < 0.0001) than dogs that did not have regular check‐ups (446 of 664) (Kendall's tau‐b). For the dogs that had regular examinations, 42.7% (93 of 218) showed an excellent response, 26.6% (58 of 218) showed a good response and 30.7% (67 of 218) showed a poor response. For the dogs that did not have regular check‐ups, 26.0% (116 of 446) showed an excellent response, 29.4% (131 of 446) showed a good response and 44.6% (199 of 446) showed a poor response to ASIT. Combining good and excellent responders, dogs that had regular follow‐up consults had a response rate of 69.3%, whereas dogs that did not had a significantly lower response rate of 55.4% (Figure 1, Appendix S4).
FIGURE 1.
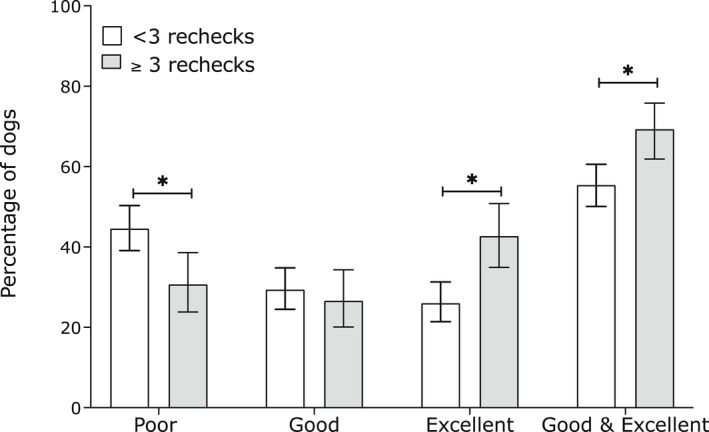
Response to allergen‐specific immunotherapy (ASIT) in atopic dogs in relation to the number of follow‐up visits during the first 9 months of ASIT. Grey columns represent dogs presented for fewer than three re‐examinations and white columns represent dogs presented for three or more rechecks. ASIT efficacy was scored poor (<50% improvement of clinical signs and reduction of concurrent medication), good (≥50% reduction of clinical signs and concurrent medication) or excellent (ASIT alone controlled clinical signs). 95% credible intervals are indicated with error bars. *p < 0.05
The type of concurrent systemic medication that had been administered during the course of ASIT significantly influenced the efficacy of ASIT (Pearson's χ2). Of the dogs that were treated with oclacitinib, 30.7% (74 of 241) showed an excellent response, 31.1% (75 of 241) showed a good response and 38.2% (92 of 241) showed a poor response. For dogs that were administered ciclosporin, 24.6% (15 of 61) showed an excellent response, 27.9% (17 of 61) showed a good response and 47.5% (29 of 61) showed a poor response. Most dogs in the glucocorticoid group, received systemic glucocorticoids for long‐term use: six dogs received glucocorticoids for less than 4 weeks, whereas the remaining 59 dogs received glucocorticoids more than 4 weeks. For the dogs that received glucocorticoids, during the first 9 months of ASIT, 10.8% (seven of 65) showed an excellent response, 27.7% (18 of 65) showed a good response and 61.5% (40 of 65) showed a poor response. Overall, the success rate for dogs that were treated with glucocorticoids of 38.5% (n = 149) was significantly lower than the success rate of 61.8% (n = 149) for the oclacitinib group, which was comparable to the overall success rate of 59.9% (p = 0.0002). The glucocorticoid group success rate also was significantly lower than the success rates of the ciclosporin and oclacitinib groups combined (p = 0.0004) (Figure 2, Appendix S5). However, the authors note that all of these effects weaken when controlling for the number of re‐examinations, because almost all patients in the glucocorticoid did not have regular re‐examinations. Analysing only patients without regular re‐examinations showed that the glucocorticoid group success rate also was still significantly lower than the success rates of the ciclosporin and oclacitinib groups combined, and not as significant as before (p = 0.04).
FIGURE 2.
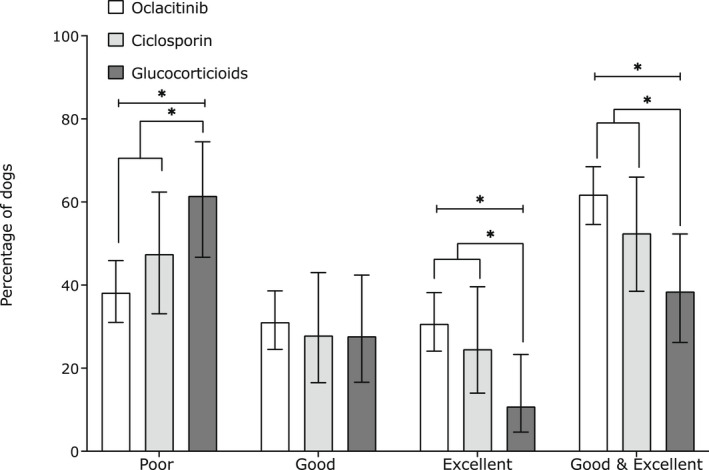
Response to allergen‐specific immunotherapy (ASIT) in atopic dogs that received concurrent systemic medication during the first 9 months of ASIT: oclacitinib, ciclosporin or glucocorticoids. ASIT efficacy was scored poor (<50% improvement of clinical signs and reduction of concurrent medication), good (≥50% reduction of clinical signs and concurrent medication) or excellent (ASIT alone controlled clinical signs). 95% credible intervals are indicated with error bars. *p < 0.05
Finally, in line with the results reported above, multivariate ordinal logistic regression showed that a model with two predictors (regular re‐examinations and concurrent systemic medication) was more strongly preferred based on the Akaike information criterion (AIC) over models with more parameters and slightly preferred over a model with only a single predictor (re‐examinations). This indicated that both re‐examinations and medication contribute to the efficiency of ASIT.
DISCUSSION
To the best of the authors' knowledge, this is the largest study investigating the efficacy of ASIT in atopic dogs. This long‐term retrospective study demonstrated that 59.9% of the atopic dogs that completed at least 9 months of ASIT showed a good or excellent response to ASIT. The 59.9% success rate is within the range of previous publications that reported success rates between 51% and 64%. 11 , 12 , 13 , 14 , 15 , 16 , 17 Concurrent administration of glucocorticoids was associated with a significantly poorer outcome of ASIT. Dogs that were presented for regular re‐examination and evaluation of the ASIT showed a significantly better response than dogs that were not.
For this study, patient records were used mainly to gather information. In 69 cases, however, patient records did not contain all of the necessary information. In these cases, the questionnaire was used to complete the data. Despite efforts to ensure the reliability of owners' answers, it is important to note that in some cases, owners might not accurately have remembered their answers to the questions in the questionnaire.
Three different groups were analysed to evaluate the effects of concurrent medication. The glucocorticoid and ciclosporin groups were relatively small when compared to the oclacitinib group. This is in part a consequence of the fact that glucocorticoids nowadays are rarely used as long‐term maintenance therapy, as there are more specific drugs available, with fewer adverse effects. In fact, 90.8% of the dogs in the glucocorticoid group commenced ASIT before 2014, which is the year in which oclacitinib became available in the Netherlands. The comparison between the oclacitinib group and the glucocorticoid group therefore included an inevitable time difference.
For ASIT to be successful, an early desensitisation of mast cells and basophils, a reduction of type 2 helper T‐cells and an induction of interleukin (IL)‐10‐secreting inducible regulatory T and B cells seems to be necessary. 7 Glucocorticoids might negatively influence the efficacy of ASIT in atopic dogs. The effects of concurrent glucocorticoid use during ASIT have not been evaluated in the dog before. 21 The significantly lower response rate for dogs that had been administered systemic glucocorticoids is therefore an important finding, especially because glucocorticoids are still one of the most effective treatments for severe cAD and often used during flares of cAD. 6 , 22 The results of the present study indicate that the use of glucocorticoids should be minimised in patients receiving ASIT whenever possible.
The success percentages of ASIT in atopic dogs treated with oclacitinib and ciclosporin were within the expected range of 51% to 64%. 11 , 12 , 13 , 14 , 15 , 16 , 17 Future prospective controlled studies are recommended to better clarify the influence of concomitant immunomodulatory medications on the efficacy of ASIT. In such studies, a control group receiving no concurrent (systemic) medication should be included to rule out any natural effects of the course of the disease. In the present study, no such control group was available owing to ethical reasons and the retrospective nature of the study. In future studies, a group receiving the recently introduced anti‐canine IL‐31 monoclonal antibody lokivetmab may be included as well. 23 , 24 Becuase lokivetmab has an even more targeted mode of action when compared to oclacitinib and ciclosporin, the immunomodulatory effects of lokivetmab and thus the influence on the efficacy of ASIT may be even more limited. 25 A limitation of the present study is that topical therapy was not taken into account. In a future prospective study, topical therapy may be included in the analysis as well, because topical therapies with antiseptics and glucocorticoids may improve the patients' symptoms considerably. 22
Dogs that were presented for regular re‐examination and evaluation of the therapy showed a significantly higher success rate. This is in accordance with a previous study by Nuttall and colleagues that reported a higher success rate in dogs that were re‐examined regularly at a referral clinic. 12 In human medicine, the level of patient satisfaction and efficacy of ASIT is closely related to the information provided regarding both the allergy as well as the treatment. Improved communication leads to increased patient knowledge, compliance and satisfaction. 26 , 27 Appropriate knowledge of the disease and its treatment is crucial for better compliance and efficacy of ASIT in atopic humans, 28 and the same may hold true for immunotherapy in cAD. Also, as in the study by Nuttall et al., re‐examinations were conducted by a referral clinician rather than by a regular veterinarian, which also may have contributed to the higher success rate. Other explanations for the observed difference beside communication and compliance might be adequate treatment of microbial infections, regular adjustment of the ASIT injection schedule and the selection of owners that wanted to continue visiting a referral clinic. 6 , 21
Three different IgE serological tests were used during the 10 year study period, which might have led to differences within the results and consequently the allergen compositions of the ASIT. However, in the last 5 years of the study the same IgE serological tests were used by both dermatology referral clinics. The influence of the different IgE serological tests therefore is assumed to have been minimal, especially because in most dogs (n = 644), both an IDT and a serological test were performed and the mixture of allergens included in ASIT was based on the results of the IDT and the IgE serological test in combination with the clinical history.
Besides mites, grass‐, tree‐ and weed allergens, flea and Malassezia allergens were included in the allergen tests in a relatively small proportion of the dogs in the present study (Table 4). Because of the small number of animals, statistical analysis could not be performed on these two allergens and they were therefore left out of the statistical analysis.
In the present study only three subjectively assessed categories were used to categorise the level of efficacy (poor, good and excellent), to ensure reliability of the efficacy scores. Efficacy was evaluated after 9 months of ASIT, which could have resulted in an underestimation of the response rate, because it may take up to 12 months before clinical improvement occurs. 5 , 6 However, two previous reports showed that virtually all dogs that respond well to immunotherapy do so within 9 months. 17 , 21 , 29
Another major limitation of this retrospective study is the fact that pruritus Visual Analog Score or the Canine Atopic Dermatitis Extent and Severity Index were not used consistently to score the clinical signs of cAD at the start of ASIT and after 9 months of immunotherapy. 19 The degree of response was based on a combination of the owners' and clinicians' impressions. 30
In summary, this study showed a response rate for ASIT that is in line with previously published response rates. A striking difference between this study and previous studies is the much higher number of dogs (664) included herein versus a maximum of 186 found in previous literature. 11 , 12 , 13 , 14 , 15 , 16 Approximately 60% of the atopic patients responded well to ASIT, and this percentage was significantly negatively influenced by the concurrent administration of glucocorticoids and positively influenced by regular follow‐up of the patient. Concurrent administration of glucocorticoids and poor follow‐up during ASIT were associated with poor response to immunotherapy. Successful immunotherapy thus seems to require regular follow‐up at a dermatological referral centre and the use of systemic glucocorticoids should ideally be minimised in order to achieve optimal effect of the ASIT.
Conflict of interest
No conflicts of interest have been declared.
AUTHOR CONTRIBUTIONS
Catharina M.M. van Damme:Conceptualization; data curation; formal analysis; investigation; methodology; visualization; writing – original draft. Yvette M. Schlotter: Data curation; writing – review and editing. Jacqueline D. Sinke: Data curation; writing – review and editing. Mieke H.G. Leistra: Data curation; writing – review and editing. Richard Tony Bartels: Formal analysis; writing – review and editing.
Supporting information
AppendixS1
AppendixS2
AppendixS3
AppendixS4
AppendixS5
AppendixS6
Fennis EE, van Damme CM, Schlotter YM, Sinke JD, Leistra MH, Bartels RT, et al. Efficacy of subcutaneous allergen immunotherapy in atopic dogs: A retrospective study of 664 cases. Vet Dermatol 2022;33:321–328. 10.1111/vde.13075
Evelien E. M. Fennis and Catharina M. M. van Damme contributed equally.
REFERENCES
- 1. Halliwell R. Revised nomenclature for veterinary allergy. Vet Immunol Immunopathol 2006;114:207–8. [DOI] [PubMed] [Google Scholar]
- 2. Hensel P, Santoro D, Favrot C, Hill P, Griffin C. Canine atopic dermatitis: detailed guidelines for diagnosis and allergen identification. BMC Vet Res 2015;11:196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Santoro D, Marsella R, Pucheu‐Haston CM, Eisenschenk MN, Nuttall T, Bizikova P. Review: Pathogenesis of canine atopic dermatitis: skin barrier and host‐micro‐organism interaction. Vet Dermatol 2015;26:84‐e25. [DOI] [PubMed] [Google Scholar]
- 4. Pucheu‐Haston CM, Bizikova P, Marsella R, Santoro D, Nuttall T, Eisenschenk MN. Review: Lymphocytes, cytokines, chemokines and the T‐helper 1‐T‐helper 2 balance in canine atopic dermatitis. Vet Dermatol 2015;26:124‐e32. [DOI] [PubMed] [Google Scholar]
- 5. Mueller RS. Update on Allergen Immunotherapy. Vet Clin North Am Small Anim Pract 2019;49:1–7. [DOI] [PubMed] [Google Scholar]
- 6. Olivry T, DeBoer DJ, Favrot C, Jackson HA, Mueller RS, Nuttall T, et al. Treatment of canine atopic dermatitis: 2015 updated guidelines from the International Committee on Allergic Diseases of Animals (ICADA). BMC Vet Res 2015;11:210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Akdis CA, Akdis M. Mechanisms of allergen‐specific immunotherapy and immune tolerance to allergens. World Allergy Organ J 2015;8:17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ozdemir C, Kucuksezer UC, Akdis M, Akdis CA. Mechanisms of aeroallergen immunotherapy: subcutaneous immunotherapy and sublingual immunotherapy. Immunol Allergy Clin North Am 2016;36:71–86. [DOI] [PubMed] [Google Scholar]
- 9. DeBoer DJ. The future of immunotherapy for canine atopic dermatitis: a review. Vet Dermatol 2017;28:25‐e6. [DOI] [PubMed] [Google Scholar]
- 10. Keppel KE, Campbell KL, Zuckermann FA, Greeley EA, Schaeffer DJ, Husmann RJ. Quantitation of canine regulatory T cell populations, serum interleukin‐10 and allergen‐specific IgE concentrations in healthy control dogs and canine atopic dermatitis patients receiving allergen‐specific immunotherapy. Vet Immunol Immunopathol 2008;123:337–44. [DOI] [PubMed] [Google Scholar]
- 11. Mueller RS, Bettenay SV. Long‐term immunotherapy of 146 dogs with atopic dermatitis – a retrospective study. Aust Vet Practit 1996;26:128–32. [Google Scholar]
- 12. Nuttall TJ, Thoday KL, van den Broek AH, Jackson HA, Sture GH, Halliwell RE. Retrospective survey of allergen immunotherapy in canine atopy. Vet Rec 1998;143:139–42. [DOI] [PubMed] [Google Scholar]
- 13. Park S, Ohya F, Yamashita K, Nishifuji K, Iwasaki T. Comparison of response to immunotherapy by intradermal skin test and antigen‐specific IgE in canine atopy. J Vet Med Sci 2000;62:983–8. [DOI] [PubMed] [Google Scholar]
- 14. Saevik BK, Thoresen SI, Kristensen F. A retrospective study of hyposensitization in canine atopy based on a polyclonal ELISA test. Vet Res Commun. 2002;26:613–24. [DOI] [PubMed] [Google Scholar]
- 15. Schnabl B, Bettenay SV, Dow K, Mueller RS. Results of allergen‐specific immunotherapy in 117 dogs with atopic dermatitis. Vet Rec 2006;158:81–5. [DOI] [PubMed] [Google Scholar]
- 16. Nesbitt GH. Canine allergic inhalant dermatitis: a review of 230 cases. J Am Vet Med Assoc 1978;172:55–60. [PubMed] [Google Scholar]
- 17. Willemse A, Van den Brom WE, Rijnberk A. Effect of hyposensitization on atopic dermatitis in dogs. J Am Vet Med Assoc 1984;184:1277–80. [PubMed] [Google Scholar]
- 18. Zur G, White SD, Ihrke PJ, Kass PH, Toebe N. Canine atopic dermatitis: a retrospective study of 169 cases examined at the University of California, Davis, 1992‐1998. Part II. Response to hyposensitization. Vet Dermatol 2002;13:103–11. [DOI] [PubMed] [Google Scholar]
- 19. Rybnícek J, Lau‐Gillard PJ, Harvey R, Hill PB. Further validation of a pruritus severity scale for use in dogs. Vet Dermatol. 2009;20:115–22. [DOI] [PubMed] [Google Scholar]
- 20. Goodman LA. On simultaneous confidence intervals for multinomial proportions. Technometrics 1965;7:247–54. [Google Scholar]
- 21. Griffin CE, Hillier A. The ACVD task force on canine atopic dermatitis (XXIV): allergen‐specific immunotherapy. Vet Immunol Immunopathol 2001;81:363–83. [DOI] [PubMed] [Google Scholar]
- 22. Olivry T, DeBoer DJ, Favrot C, Jackson HA, Mueller RS, Nuttall T, et al. Treatment of canine atopic dermatitis: 2010 clinical practice guidelines from the International Task Force on Canine Atopic Dermatitis. Vet Dermatol 2010;21:233–48. [DOI] [PubMed] [Google Scholar]
- 23. Michels GM, Walsh KF, Kryda KA, Mahabir SP, Walters RR, Hoevers JD, et al. A blinded, randomized, placebo‐controlled trial of the safety of lokivetmab (ZTS‐00103289), a caninized anti‐canine IL‐31 monoclonal antibody in client‐owned dogs with atopic dermatitis. Vet Dermatol 2016;27:505‐e136. [DOI] [PubMed] [Google Scholar]
- 24. Souza CP, Rosychuk RAW, Contreras ET, Schissler JR, Simpson AC. A retrospective analysis of the use of lokivetmab in the management of allergic pruritus in a referral population of 135 dogs in the western USA. Vet Dermatol 2018;29:489‐e164. [DOI] [PubMed] [Google Scholar]
- 25. Moyaert H, Van Brussel L, Borowski S, Escalada M, Mahabir SP, Walters RR, et al. A blinded, randomized clinical trial evaluating the efficacy and safety of lokivetmab compared to ciclosporin in client‐owned dogs with atopic dermatitis. Vet Dermatol. 2017;28:593‐e145. [DOI] [PubMed] [Google Scholar]
- 26. Chivato T, Álvarez‐Calderón P, Panizo C, Abengozar R, Alías C, Al‐Baech A, et al. Clinical management, expectations, and satisfaction of patients with moderate to severe allergic rhinoconjunctivitis treated with SQ‐standardized grass‐allergen tablet under routine clinical practice conditions in Spain. Clin Mol Allergy 2017;15:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Marple BF, Fornadley JA, Patel AA, Fineman SM, Fromer L, Krouse JH, et al. Keys to successful management of patients with allergic rhinitis: focus on patient confidence, compliance, and satisfaction. Otolaryngol Head Neck Surg. 2007;136:S107–24. [DOI] [PubMed] [Google Scholar]
- 28. Canonica GW, Cox L, Pawankar R, Baena‐Cagnani CE, Blaiss M, Bonini S, et al. Sublingual immunotherapy: World Allergy Organization position paper 2013 update. World Allergy Organ J 2014;7:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. DeBoer DJ. Survey of intradermal skin testing practices in North America. J Am Vet Med Ass 1989;195:1357–63. [PubMed] [Google Scholar]
- 30. Olivry T, Saridomichelakis M, Nuttall T, Bensignor E, Griffin CE, Hill PB, et al. Validation of the Canine Atopic Dermatitis Extent and Severity Index (CADESI)‐4, a simplified severity scale for assessing skin lesions of atopic dermatitis in dogs. Vet Derm 2014;25:77–85. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
AppendixS1
AppendixS2
AppendixS3
AppendixS4
AppendixS5
AppendixS6