
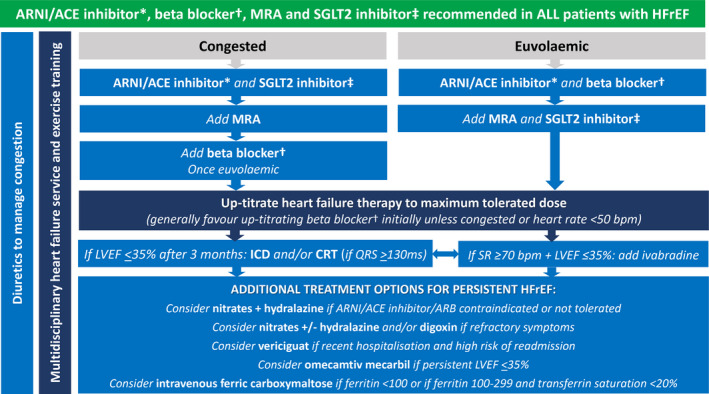
ACE = angiotensin‐converting enzyme; ARNI = angiotensin receptor neprilysin inhibitor; CRT = cardiac resynchronisation therapy; HFrEF = heart failure with reduced ejection fraction; ICD = implantable cardioverter defibrillator; LVEF = left ventricular ejection fraction; MRA = mineralocorticoid receptor antagonist; SGLT2 = sodium–glucose cotransporter 2; SR = sinus rhythm.
The key overarching theme (green background) is to commence all patients on the four destination therapies of ARNI/ACE inhibitor*, beta blocker†, MRA and SGLT2 inhibitor‡ as soon as clinically possible, given their early morbidity and mortality benefit.
* ARNI preferred. ACE inhibitor can be considered as an alternative if problematic hypotension, and consider switching to ARNI later. † Use beta blocker with outcome trial proven HFrEF efficacy (ie, carvedilol, bisoprolol, metoprolol succinate or nebivolol). ‡ Use SGLT2 inhibitor with outcome trial proven HFrEF efficacy (ie, dapagliflozin or empagliflozin).