

Abstract
Aims
To investigate Group B Streptococcus (GBS) colonization in pregnancy; adherence to antenatal GBS screening and adherence to the intrapartum antibiotics protocol within two models of care (midwifery and non‐midwifery led).
Design
This retrospective quantitative study has employed a descriptive design using administrative health data.
Methods
Data from five maternity hospitals in metropolitan and regional Western Australia that included 22,417 pregnant women who gave birth between 2015 and 2019 were examined, applying descriptive statistics using secondary data analysis.
Results
The study revealed an overall GBS colonization rate of 21.7% with similar rates in the different cohorts. A lower adherence to screening was found in the midwifery led model of care (MMC, 68.76%, n = 7232) when compared with the non‐midwifery led model of care (NMMC, 90.49%, n = 10,767). Over the 5 years, screening rates trended down in the MMC with stable numbers in the counterpart. Adherence in relation to intrapartum antibiotic prophylaxis revealed discrepant findings between the study groups.
Conclusion
Adherence to screening and management guidelines of maternal GBS colonization in pregnancy is lower within the MMC when compared with the NMMC.
Impact
This is the first cohort study to describe the adherence to the recommended Western Australian GBS screening guidelines in the two different models of care. Findings may assist in the guidance and improvement of clinical protocols as well as the planning of clinical care in relation to GBS screening to reduce the risk of neonatal GBS infection.
Keywords: adherence, Group B Streptococcus, intrapartum antibiotic prophylaxis, midwifery led model of care, midwives, neonatal early‐onset Group B Streptococcus disease, pregnancy, screening guidelines
1. INTRODUCTION
Group B Streptococcus (GBS) is a fast‐growing gram‐positive bacterium which commonly colonizes the upper respiratory tract, as well as the gastrointestinal and genitourinary tract of approximately 30% of asymptomatic adults (Murray et al., 2016). During pregnancy, GBS can increase the risk of urinary tract infection, chorioamnionitis, endometritis and sepsis, featuring as a risk factor for miscarriage, preterm labour and stillbirth (Steer et al., 2020). Typically colonizing a pregnant woman's intestinal and/or genitourinary tract, GBS can spread to the amniotic fluid, placenta, cervix or vagina (Heath & Jardine, 2014). The foetus can then acquire the bacteria either in‐utero via vertical transmission during labour (even with membranes intact) or during vaginal birth (Steer et al., 2020). Invasive Early‐Onset Group B Streptococcus Disease (EOGBSD), which occurs from 0 to 7 days of life, can result leading to serious complications for neonates including meningitis, pneumonia and neonatal sepsis, where it continues to be a major cause of morbidity and mortality among term and preterm neonates (HogenEsch et al., 2020). Neonates who survive a GBS infection can suffer from long‐term effects and permanent problems, for example blindness, deafness, moderate‐to‐severe neurological impairments and cerebral palsy (World Health Organization, 2017). Seale et al. (2017) have reported a global disability rate of greater than 10,000 incidents of neurological development disorders annually caused by GBS meningitis in infants. Worldwide, an estimated 150,000 stillbirths and neonatal deaths each year are attributed to GBS infection (World Health Organization, 2017). In several European countries, for example the United Kingdom, Ireland, Italy and the Netherlands, an increase of early‐onset GBS infections have been described for the last decades (De Luca et al., 2016; O'Sullivan et al., 2019). A large retrospective analysis of data collected from multiple hospitals in Australia and New Zealand has reported an EOGBSD rate of 0.43/1000 live births with a mortality rate of 11% (Singh et al., 2019). Preterm neonates are at significantly increased risk, amounting to 3% for infection rates and up to 30% of mortality rates (Heath & Jardine, 2014).
1.1. Background
Universal GBS screening has been an effective tool for tackling neonatal sepsis, where it includes rectovaginal culture swabs between 35 and 37 weeks of gestation to identify women who are colonized with GBS, who then receive intrapartum antibiotic prophylaxis (IAP) (Hasperhoven et al., 2020). This preventative strategy has led to a significant reduction in EOGBSD globally and is considered more effective than a risk‐based approach where intrapartum antibiotics are administered on determination of certain risk factors for EOGBSD including, prolonged rupture of membranes (≥18 h), a previous neonate with EOGBSD, GBS bacteriuria or maternal fever (≥38°C) (Hasperhoven et al., 2020). Compelling evidence demonstrates the negative impact of low uptake of GBS screening on neonatal infection rates (Hasperhoven et al., 2020). In Western Australia (WA), the risk of GBS disease in pregnancy has primarily been managed through recommendations of universal screening at 35 and 37 weeks' gestation, with the administration of prophylactic antibiotics in labour if the screening result returns positive for GBS colonization or if membranes have ruptured before labour begins (Homer et al., 2014).
Various models of maternity care are available for Western Australian women, including public hospital care, care from a general practitioner, private midwife or private obstetrician, shared care and midwife led care (WA Department of Health, 2019). While there has been international research regarding adherence to antenatal GBS screening guidelines (Dalmartello et al., 2019; De Luca et al., 2016; Gopal Rao, Nartey, et al., 2017; HogenEsch et al., 2020; Kunze et al., 2015; Yamaguchi & Ohashi, 2018), as well as two Australian studies (Braye et al., 2019; Moorhead et al., 2019), only one has been identified with a focus on adherence to GBS screening guidelines specifically within the midwifery led model of care (MMC) (Yamaguchi & Ohashi, 2018). Knowledge is limited regarding the comparison of adherence to GBS screening between pregnant women cared for in different care models, particularly under the MMC, and those cared for under the non‐midwifery led model of care (NMMC). Likewise, to date the comparison of screening results between these two models has not been examined. The objective of this study was therefore to investigate the adherence to GBS screening and management guidelines including GBS colonization rates, in these two models of maternity care in Western Australia. In this paper, maternity care facilitated by midwives as primary caregivers is referred to as the ‘midwifery led model of care’ while all other care options are referred to as ‘non‐midwifery led model of care’.
2. THE STUDY
2.1. Aims
The overall aim of this study was to investigate the adherence to the recommended prevention strategy for early‐onset neonatal GBS infection in Western Australia in pregnant women of the MMC and the NMMC and was guided by the following objectives:
To determine the overall and population specific rate of GBS colonization in pregnancy in all groups under study
To examine the prevalence of antenatal GBS screening adherence specific to the MMC group, the NMMC group and subgroups including Midwifery Group Practice (MGP), the Community Midwifery Programme (CMP), and the group of Private Midwives (PM) using electronic administrative birth data
To examine the adherence to IAP in all groups under study when antenatal GBS screening showed a GBS positive result
2.2. Design
Using secondary data analysis, descriptive statistics will be presented to systematically examine and identify the patterns and trends of Group B Streptococcus screening and management adherence in midwifery and NMMC.
2.3. Sample
No participants were involved in this study since the data used were obtained from electronic health datasets. The population of interest for this study was pregnant women whose pregnancy resulted in a live birth at term (from 37 weeks gestation) and who received antenatal care in Western Australia from midwifery led and non‐midwifery led care providers. The women's age ranged from 13 to 53 years, representing 169 different countries of birth. Other demographics included the number of pregnancies, which ranged from 1 to 20 as well as the number of previous livebirths ranging from 0 to 12. Included births occurred in five metropolitan and regional hospitals, a birth centre and at home, between 1 January 2015 and 31 December 2019. As given in Table 1, the study population of Hospital 1 included both MMC and NMMC, while the study population of Hospitals 2, 3 and 4 comprised the MMC only. The rationale behind this related to the enormous number of births of the NMMC group at Hospital 1 (15,268 vs. 11,140 of the total number of MMC group of all five hospitals). Data from Hospital 5 contained birth records from both models of care as MGP commenced only in 2017. We excluded women who gave birth before 37 weeks gestation or had an elective Caesarean section.
TABLE 1.
Details of the sample (received data sets, January 2015 – December 2019)
| Source | Midwifery led model of care | Non‐midwifery led model of care |
|---|---|---|
| Hospital 1 | 7074 | 15,268 |
| Hospital 2 | 2608 | ‐ |
| Hospital 3 | 554 | ‐ |
| Hospital 4 | 833 | ‐ |
| Hospital 5 | 48 | 23 |
| Subtotal | 11,117 | 15,291 |
| Total: 26,408 | ||
2.4. Data collection
Electronic health data (26,408 data sets) containing information about pregnancy and birth were extracted from the database Stork. Stork is the clinical perinatal database used by all Western Australian public health maternity services, including homebirth providers, to record point‐of‐care details related to care during pregnancy, birth and the postnatal period (WA Department of Health, 2016). It is mandatory for caregivers to enter information related to GBS screening in pregnancy.
Data included maternal age, gravity, parity, country of birth of the mother, GBS test result and administration of appropriate antibiotic prophylaxis. The GBS status was assigned as positive, negative or pending based on the antenatal GBS culture screening or as not tested where the screening test was not performed and/or declined by the woman.
2.5. Data analysis
The GBS colonization and adherence rates of antenatal GBS screening among all women, main and subgroups were identified, where distribution and central tendency was investigated. It was examined whether trending characteristics exist regarding GBS screening adherence in both models of care (midwifery and non‐midwifery led) over the 5‐year period. Further, it was investigated if the dependent variable (GBS test result) varied according to subgroups (MGP, CMP, PM). Using the same analytic methods, the adherence to IAP was examined. Adequate IAP was defined as the initiation of a recommended dose of antibiotic intravenously at least 4 h prior to birth (Morgan et al., 2020). Maternal demographics such as women's country of birth, maternal age distribution, gravidity and parity in the two models of care were included in the analysis. Outcomes were measured and reported numerically as percentages and counts and displayed in bar and line graphs to demonstrate proportional differences.
Data quality assessment, cleaning and preparation were conducted in numerous steps resulting in a new database with a final sample size of 22,417 data sets using the software programmes Microsoft Excel and SPSS Version 26. This involved the development of specific variables to identify non‐midwifery and midwifery led care groups and their subgroups. A detailed description of the data quality assessment, cleaning and preparation process can be sighted on request.
2.6. Validity, reliability and rigour
The exhaustive process of data cleaning, preparing and primary analysis in this study ensured that only appropriate variables were utilized and that the analysis was valid. Descriptive validity is a relatively new but increasingly popular means of determining the rigour of a research project (Bergin, 2018). This type of validity refers to a provision of detailed and accurate descriptions of how data were collected and analysed, which also can assist in replicating the methods and results in future research (Bergin, 2018). This study offers a comprehensive description of the data collection and analysis processes ensuring its robustness and rigour. This process has been clearly detailed in the research report, providing a trail for any future research to follow and arrive at the same results using this database, further demonstrating the reliability of the work. This transparency, as Rotelli (2015) advocates, is an important requirement for establishing strong reliability in retrospective analysis of administrative healthcare data.
3. RESULTS
3.1. Data distribution
The sample of this study comprised data of the two models of care across five hospitals in metropolitan and regional Western Australia. The proportion of women receiving midwifery led care was slightly smaller (46.92%, n = 10,519) compared with 53.08% (n = 11,898) of women receiving non‐midwifery led care. Importantly, the vast majority of data were derived from Hospital 1 with 83.19% (n = 18,648). The rate for Hospital 2 was 10.71% (2400), which was substantially higher than for Hospital 3 with 2.40% (n = 539) and Hospital 4 with 3.39% (n = 759). The smallest proportion of data with 0.32% (n = 71) was identified for Hospital 5. Hospital 1 comprised the two different models, with 36.33% (n = 6773) of women in the midwifery led care group and a higher proportion of women receiving non‐midwifery led care (63.67%, n = 11,875). It was the only hospital representing other subgroups of the midwifery led care model which included the MGP as the largest group among them (81.60%, n = 5527), the CMP with 14.88% (n = 1008), and the group of PM with a small proportion of 2.49% (n = 168). Seventy records (1.03%) were not analysed across these subgroups as they genuinely involved two or more subgroup provider types. This means that 27 records reported women receiving shared care by the MGP and CMP, while 35 women received care by MGP and PM, seven women were cared for by the CMP and PM. One woman was provided maternity care from all three care providers. As presented in Figure 1, apart from Hospital 1 and 5, data received from all other institutions referred to midwifery led care exclusively, with Hospital 5 providing less than half of their pregnant population (n = 23/71) non‐midwifery led care.
FIGURE 1.
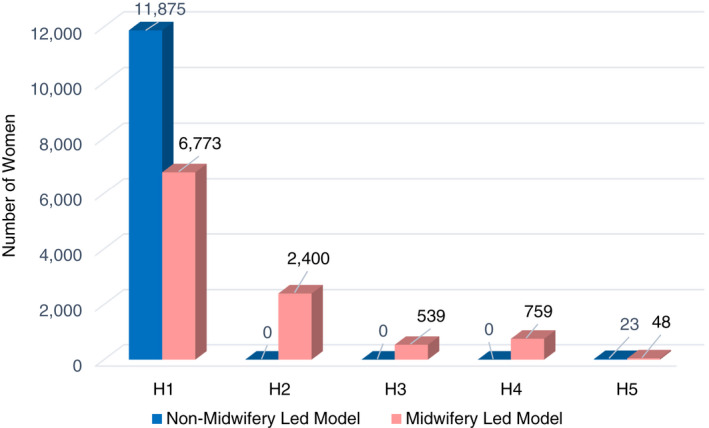
Overview of sample by model and data source
3.2. Maternal demographics
These data were generated from a diverse cohort of pregnant women representing 169 different countries of birth with just over half of the women having been born in Australia (55.52%, n = 12,445). The various countries were grouped into six geographic regions according to the WHO's recommendation (WHO, 2021). The African region represented 1039 women (4.63%), the Eastern Mediterranean region 912 (4.07%), the European region 2807 (12.52%), the region of Americas 603 (2.69%), the South‐East Asia region 1859 (8.29%) and the Western Pacific region the highest number of 15,186 women (67.74%). For 10 women (0.04%), the country of birth was not available. On comparison, the majority of women of both care models were born in countries of the Western Pacific region with 70.85% (n = 74.54) of women of the MMC group and 65% (n = 7732) of the NMMC group. There was little difference with some divergence in women having been born in the South‐East Asian region (11.57%, n = 1376 vs. 4.59%, n = 483) and European region (16.38%, n = 1723 vs. 9.11%, n = 1084). Even smaller was the difference for women with their birth country grouped in the regions of Americas with 3.27% (n = 344) for the MMC and 2.18% (n = 259) for the NMMC. The percentage of women having been born in the African region was comparable in both groups with 3.37% (n = 355) in the MMC and 5.75% (n = 684) in the NMMC. A small contrast was identified when comparing women with the country of birth in the Eastern Mediterranean region with a low 1.47% (n = 155) in the MMC group versus 6.36% (n = 757) in the NMMC cohort. The women's ages ranged from 13 to 53 years (M = 30.1). The electronic database did not provide reliable information in relation to the socioeconomic status of the women, such as educational attainment, income, occupation and financial security. A comparison of the maternal age distribution, gravidity and parity in the two models of care revealed no differences.
3.3. Group B Streptococcus colonization
The GBS colonization rate within this whole Western Australian pregnant cohort who received GBS screening was found to be 21.70% (n = 3907). Comparable rates of GBS colonization were identified in the two care models (Table 2). A small percentage was detected with GBS results still pending at the time of birth (3.53%, n = 792).
TABLE 2.
Prevalence of GBS colonization
| Study population | Women tested | GBS positive | |
|---|---|---|---|
| n | n | % | |
| Whole population | 17,999 | 3907 | 21.70 |
| Midwifery led model of care | 7234 | 1470 | 20.32 |
| Non‐midwifery led model of care | 10,765 | 2437 | 22.63 |
Abbreviation: GBS, Group B Streptococcus.
3.4. Prevalence of adhering to antenatal GBS screening
The vast majority of all pregnant women under study had the GBS screening test administered (80.29%, n = 17,999), indicating that 19.71% of all women (n = 4418) did not receive the screening test. When comparing the two models of care, remarkable differences were discovered. In the MMC population (n = 10,519), a low rate of adherence to GBS screening was found (68.76%, n = 7232) compared with a much higher rate of 90.49% (n = 10,767) in the group of pregnant women cared for by the NMMC (n = 11,898). This means that 31.24% (n = 3287) of pregnant women in the midwifery led care model were not tested for GBS colonization in pregnancy, in contrast to 9.50% (n = 1131) in the NMMC.
Evaluation of the screening trends in antenatal GBS screening characteristics over the 5 years for both care provider groups was conducted (Figures 2 and 3). This revealed a notable increase in the rate of the midwifery led women not tested for GBS colonization. In contrast, in the non‐midwifery led care model, the rate of women not tested was low, revealing an unremarkable rise. The GBS positive rate was found trending low over the years from 15.60% (n = 255) to 12.61% (n = 294) in the midwifery led care models, and from 21.81% (n = 577) to 18.46% (n = 419) in the non‐midwifery led care group. The rate of women tested GBS negative was notably declining in the midwifery led models of care while remaining relatively stable in this time period in the non‐midwifery care model. When the pending results were analysed, a stable rate was observed in the midwifery led group, whereas a slight uptrend over the years was found in the non‐midwifery led cohort.
FIGURE 2.
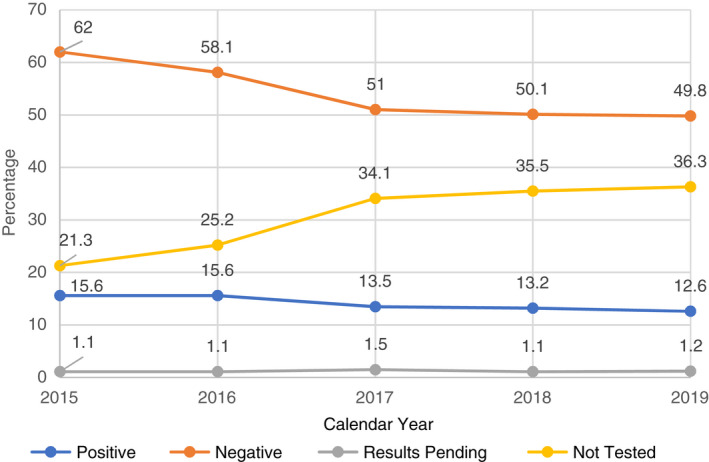
Trends of GBS screening adherence in the midwifery led model of care (including screening details). GBS, Group B Streptococcus
FIGURE 3.
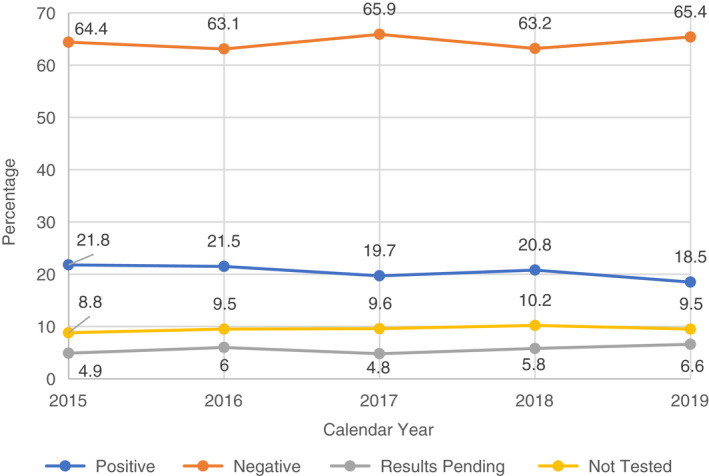
Trends of GBS screening adherence in the non‐midwifery led model of care (including screening details). GBS, Group B Streptococcus
The exploration of results among the different subpopulations was of particular importance as vast differences became apparent. All five hospitals provided the MGP model of care. Among these MGP groups, the GBS adherence rates and screening details were examined and contrasted. As this is one midwifery led care provider type, it is surprising that the results of screening adherence varied vastly ranging from 57.28% (n = 3166) to 96.19% (n = 730). For Hospital 1 with the largest number of women in the MGP model (n = 5527), the lowest rate of GBS screening adherence was discovered. This was followed by a similarly low rate in the small population of Hospital 5. A much higher proportion of pregnant women were tested for GBS colonization in the MGP group of Hospital 3. Among all five MGP groups, Hospital 2 and Hospital 4 ranged the highest (all details are presented in Figure 4).
FIGURE 4.
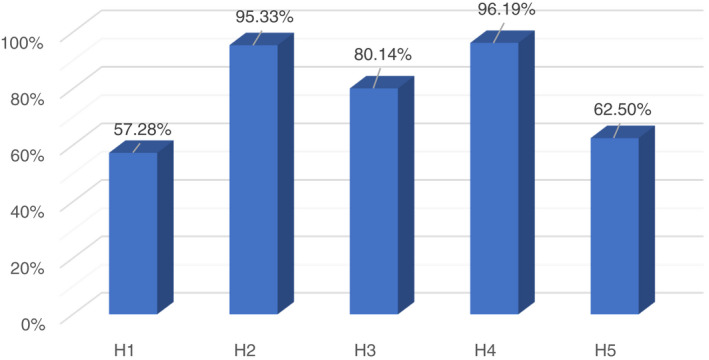
Prevalence of adherence to GBS screening in midwifery group practice. GBS, Group B Streptococcus
Among the three subgroups of the MMC (MGP, CMP, and PM) at Hospital 1, an interesting trend emerged. The adherence rate to screening in the MGP group was found to be remarkably low (57.28%, n = 3166), indicating that close to one half of the proportion of pregnant women (42.72%, n = 2361) were not tested for GBS colonization. However, when these results were compared with the groups of CMP and PM, they were the highest for the GBS screening adherence. In the CMP cohort, only 48.51% (n = 489) of women underwent GBS testing with 51.49% (n = 519) receiving no GBS test in their pregnancy. Notably, an even lower rate of adherence was identified in the PM population (44.05%, n = 74), which means that more than a half of this group (55.95%, n = 94/168) missed out on screening for GBS colonization (Figure 5).
FIGURE 5.
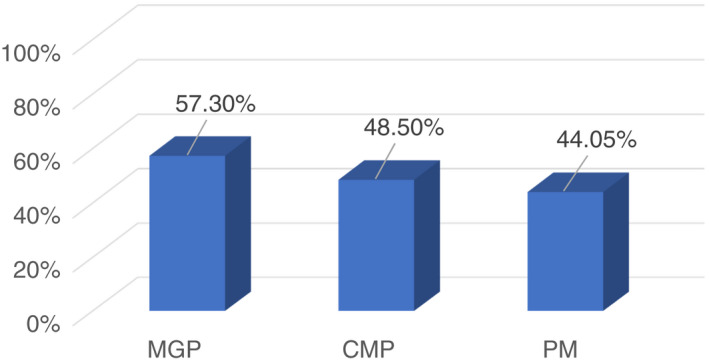
Prevalence of GBS screening adherence among subgroups. GBS, Group B Streptococcus
Comparing GBS screening adherence rates between the hospitals it was found that in the midwifery led models of care rates were the highest in Hospital 4 (96.19%, n = 730) with only 3.81% (n = 29) of women not tested. Similarly, high rates were identified among women of Hospital 2 (95.33%, n = 2288), indicating that a small 4.67% (n = 112) group of women did not receive GBS screening. While 80.14% (n = 432) in Hospital 3 was the third highest GBS screening adherence rate with 19.86% (n = 107) of women not tested, data revealed a much lower rate for women cared for in Hospital 5 (62.50%, n = 30) with more than a third of women not receiving the GBS screen (37.50%, n = 18). Surprisingly, the lowest rate of adherence to GBS screening in this care model was found in Hospital 1 (57.28%, n = 3166), indicating that over 40% of this cohort was not tested (42.72%, n = 2361). In the non‐midwifery led population, a high 90.51% (n = 10,748) of pregnant women in Hospital 1 received GBS screening with 9.49% (n = 1127) not tested, whereas corresponding findings did emerge for the population of Hospital 5 in this model of care (82.61%, n = 19 and 17.39%, n = 4 not tested). For these two hospitals, the group average was nearly identical (H1—73%, H5—72.55%) (Figure 6).
FIGURE 6.
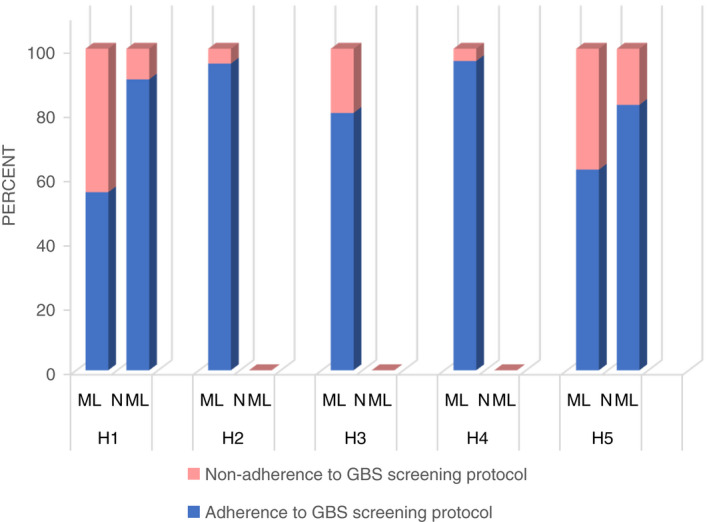
Adherence to GBS screening based on model of care and setting. GBS, Group B Streptococcus
3.5. Adherence to IAP
Among all women under study, 3907 (21.70%) women had an indication for IAP due to a GBS positive test result. Investigations of adherence to IAP revealed that 73.68% (n = 2879) women were provided with it. When adherence rates to IAP were compared between the two models of care on the numbers of GBS colonized women in each group (MMC n = 1470, NMMC n = 2437), the results revealed a low adherence rate in the MMC group (65.51%, n = 963). This means, 34.49% (n = 507) of women did not receive antibiotic prophylaxis in labour. In contrast, in the NMMC cohort, 78.62% (n = 1916) of women were given IAP, leaving 21.38% (n = 521) without prophylactic treatment.
When adherence rates to IAP were compared among the GBS colonized women of the MGP population of all five hospitals (n = 1341), enormous differences were revealed with all findings below 70%. The GBS positive‐tested MGP women in Hospital 1 (n = 698) were administered IAP in 67.33% (n = 470), indicating that 32.66% (n = 228) women did not receive it. In comparison, remarkably close results were revealed for the 428 MGP women with GBS colonization in Hospital 2, of whom 68.45% (n = 293) received IAP with 31.55% (n = 135) of women not being treated. In contrast, the adherence rates for Hospital 3 were much lower with just over half of all GBS positive tested MGP women (n = 72) receiving IAP (59.72%, n = 43) with similar findings among the 136 women in Hospital 4 who were treated with prophylactic antibiotics in 53.67% (n = 73). This means that nearly half of the proportion of women were not administered IAP in the MGP groups of Hospital 3 and 4 (H3 40.28%, n = 29; H4 46.33%, n = 63). The adherence rate for Hospital 5 with seven GBS positive tested women was extremely low at 28.57% (n = 2), indicating that the majority of these women missed out on IAP (71.42%, n = 5) (Figure 7).
FIGURE 7.
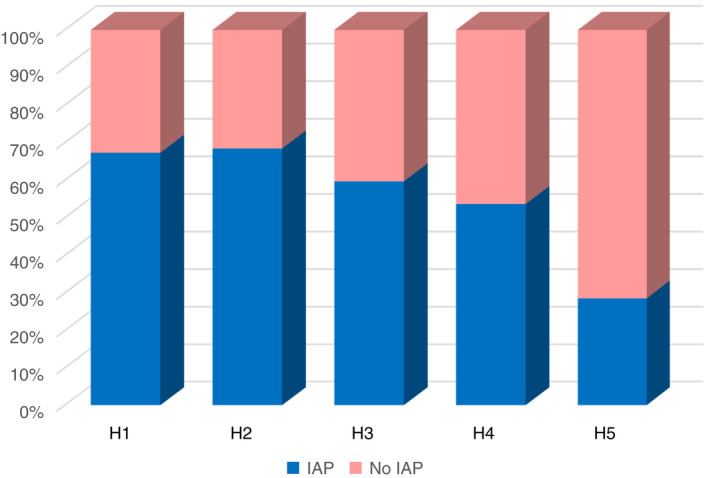
Adherence to intrapartum antibiotic prophylaxis among midwifery group practice groups
On further examination, the results of subgroups of the MMC in Hospital 1 in relation to adherence to IAP were compared and revealed varying findings. The highest rate was found in the MGP cohort with 67.33% (n = 470/698) with 32.66% (n = 228) not covered with antibiotics followed by 63.72%, n = 65) in the group of CMP which included 102 GBS colonized women, indicating that 36.28% (n = 37) of women did not receive prophylactic antibiotics. In stark contrast, in only half of the group of women tested GBS positive in the PM population (n = 19), IAP was adhered to (52.63%, n = 10) while 47.37% (n = 9) were not provided with antibiotic prophylaxis.
4. DISCUSSION
This retrospective study has presented a structured investigation of characteristics of GBS screening adherence plus intrapartum management with antibiotics in two major target groups of pregnant women in Western Australia. To the researchers' knowledge, no study has examined the comparison between the midwifery led and the non‐midwifery led models of care in this context.
4.1. GBS colonization
The examination of GBS colonization data across the five hospitals revealed an overall rate of 21.70% which was similar to average rates in international research (Edwards et al., 2019; Jisuvei et al., 2020; Ramesh Babu et al., 2017; Szylit et al., 2020) and consistent with results of previous Australian studies (Braye et al., 2019; Furfaro et al., 2019; Moorhead et al., 2019). No studies were located to relate findings of the current study in relation to the different models of care (non‐ and midwifery led care). However, differences in GBS colonization rates in the present study between the two care models, and also between each hospital across the large geographical area of Western Australia, were observed, mirroring variations between countries (Kwatra et al., 2016; Shabayek & Spellerberg, 2018). These findings indicate that variations occurred in different ethnic populations across the world with the highest GBS colonization rate among African women and the lowest in the pregnant population of Asia and the Middle East (Gopal Rao et al., 2019; Shabayek & Spellerberg, 2018). Population differences suggest varying natural immunity of pregnant women to GBS along with factors such as lifestyle, swab collection methods and laboratory techniques which can also contribute to different GBS colonization rates (Ashary et al., 2020; Furfaro et al., 2019; Lao, 2019). Underlying population differences in the natural immunity of pregnant women to GBS may explain the different GBS colonization rates in the current study. Various factors may affect the maternal immune system including anthropometric measures and racial background (Lao, 2019). Different immune responses occur in women of high‐income countries, compared with women from non‐industrialized population groups, over the course of pregnancy, including pro and anti‐inflammatory processes possibly due to contrasting immunological demands in pregnancy between these ecologically distinct population groups (Anderson et al., 2020).
4.2. Adherence to antenatal GBS screening
The current study found that the adherence rate to antenatal GBS screening guidelines was high in the whole population cohort, which corroborated previous Australian (Braye et al., 2019; Moorhead et al., 2019) and international findings (Berardi et al., 2017). The differences of adherence rates between the two models of care, as well as the unexpected findings of the discrepancies between the MGP groups when compared separately for each hospital, were surprising and not comparable to literature due to the lack thereof. This study's results corroborate previous findings in that GBS adherence rates among pregnant women in the MMC were low (Yamaguchi & Ohashi, 2018). Further, an examination of the 5‐year trend in the current study indicated a decrease in the GBS screening rate of women in the midwifery led model, when compared with a stable proportion in the non‐midwifery led care group. This decreased testing raises important questions as to possible reasons for this trend. There could be potential professional determinants, such as midwife knowledge and perspectives, differences in hospital specific acknowledgement of clinical guidelines, non‐standardized educational material for pregnant women, or factors that include women's knowledge and perceptions as well as controversial opinions in regard to prevention strategies to avoid neonatal early‐onset GBS disease.
4.2.1. Midwives' knowledge and perspectives
Midwives, as the lead professional care provider in the MMC, play a critical role when it comes to adherence to clinical guidelines. Among midwives in this model of care, autonomous practice and women‐centred care are highly regarded (Sheehy et al., 2019). Midwives are the highest ranked source of information for pregnant women followed by medical personnel and media (McQuaid, Pask, et al., 2016). By providing information, education and counselling, a midwife supports women to make informed decisions and promotes woman‐centred care during pregnancy, birth and the postnatal period (Hunter et al., 2017). This is an important consideration when examining adherence to GBS screening guidelines in pregnancy, because the information the woman receives from the midwife can significantly contribute to her decision making for or against the test. Consequently, a midwife's knowledge and approach to GBS screening remarkably affects and guides a woman's decision. Knowledge about GBS in pregnancy among midwives can differ, as highlighted by one group of parents that stated that health professionals did not seem well informed about this topic (McQuaid, Jones, et al., 2016). Considering the low adherence rate to GBS screening in the MMC in the current study, possible specific education of midwives to improve adherence to the recommended GBS screening guidelines in Western Australia may be an effective intervention. In this regard, Pangerl et al. (2021) in their review of the literature have demonstrated that implementing educational measures into the clinical practice of health professionals can result in an increase in antenatal GBS screening rates. The knowledge and perspectives of midwives in relation to GBS screening guidelines might also be impacted by their backgrounds.
The midwifery workforce in Western Australia comprises of midwives from all around the world. Midwives possess vastly different backgrounds including variations in midwifery qualifications, scope of practice, midwife to women ratios, professional autonomy, culture and practice differences (Philip et al., 2019). The specific imprint of work experience in the country of qualification may influence clinical practice in Western Australia. For example, midwives trained in the United Kingdom, where antenatal GBS screening is not common practice, may have different viewpoints as compared with midwives from countries with GBS screening guidelines such as the USA. Further, the recognition of clinical GBS practice guidelines by midwives is integral in providing quality care with the aim of best health outcomes for women and their newborns.
4.2.2. Recognition of clinical guidelines
The current study does not provide direct evidence as to differences in how clinical guidelines have been recognized at each hospital. However, it is possible that adherence to clinical guidelines may explain discrepancies in adhering to GBS screening guidelines in the present study. Evidence‐based clinical guidelines ensure best practice and optimal quality of clinical care for maternal and neonatal health; therefore, adherence to these standards is an essential part in the scope of practice of health professionals (Millington et al., 2020). Notably, adherence rates to GBS screening guidelines in the MGP cohort in the current study were lowest at a tertiary hospital, where Western Australia GBS screening guidelines were initiated and found the highest in the hospital furthest away from metropolitan Western Australia. These findings are inconsistent with an analysis of adherence to other clinical guidelines in a multi‐centre study (Millington et al., 2020). It is possible that the importance of the recommended Western Australia GBS screening guidelines was acknowledged and interpreted differently in each hospital, which may be rooted in the personal commitment of midwives to professional accountability and ownership (Sherman & Cohn, 2019).
Professional accountability in health care requires compliance with workplace protocols and ethical standards. Differences in practice patterns of health professionals may be explained by a lack of understanding of workplace protocols and procedures (Sherman & Cohn, 2019). Further, adherence to clinical protocols may be evaluated more or less consistently at various hospitals and possibly with different levels of standards for accountability, responsibility and ownership of clinical guidelines, which may be influenced by the leadership or management of the specific health care facility (Hegarty et al., 2019). The current study's adherence rates to GBS screening guidelines dwindled further when subgroups of the midwifery led care model (MGP, CMP, PM) were examined separately, indicating that the more the care was detached from hospital environments, the lower the screening rate. It can be speculated that explanations offered above may have influenced the findings. In addition to the recognition of clinical guidelines, different educational strategies informing pregnant women about GBS in pregnancy may influence maternity care.
4.2.3. Educational strategies during antenatal visits
The provision of non‐standardized education material and methods across the different population groups might be another contributing factor to dissimilar screening adherence rates in the present study. Antenatal care is provided in various settings including hospitals, outpatient care centres and at home by midwives and obstetricians using differing educational strategies to inform pregnant women, aiming for the best maternal and neonatal health outcomes. Multiple formats for conveying antenatal education to pregnant women can be utilized such as explanatory booklets, face‐to‐face information, group information sessions, videos and health apps. Admittedly, it can be challenging for health professionals to communicate the same information in all the different formats. For example, parents who were affected by GBS infection previously, voiced the importance of adequate antenatal education in relation to GBS, as they felt it was not provided to themselves (McQuaid, Pask, et al., 2016). In the current multi‐centre study, antenatal care was conducted in multiple ways and settings. While it could not be evidenced from the data, it is reasonable to assume that different methods were used, resulting in different GBS screening rates. Therefore, a standardized and regulated antenatal education system, providing women with equal opportunities for a well‐informed decision may need to be developed. Further, pregnant women's knowledge and perceptions are important in relation to adherence to GBS screening.
4.2.4. Women's knowledge and perceptions
Women's knowledge and perceptions in relation to GBS screening should be considered. In contemporary Western culture, women understand pregnancy and childbirth rather subjectively, incorporating their individual circumstances and unique situations including level of education, previous childbearing experiences and place of residence (Lee et al., 2019). Empirical evidence suggests that the knowledge of women concerning GBS in pregnancy and the associated risk of neonatal infection is generally poor (Alshengeti et al., 2020; McQuaid, Jones, et al., 2016; McQuaid, Pask, et al., 2016). Differences in knowledge between women in their first pregnancy compared with women with previous pregnancies have been observed (McQuaid, Jones, et al., 2016), which may have contributed to variations in GBS screening adherence in the present study. Furthermore, controversial views among maternity care professionals may explain the observed differences.
4.2.5. Controversial opinions and contrasting views
The discrepancies in findings of the current study about adherence to recommended prevention guidelines may be a result of different views among health professionals, reflecting a long ongoing debate about which prevention approach should be adopted (Rao & Khanna, 2020). Various observational studies have examined and compared the effectiveness of both prevention strategies, finding a significant reduction of neonatal early‐onset GBS disease when the universal GBS screening approach is used (Al Luhidan et al., 2019; Gopal Rao, Townsend, et al., 2017; O'Sullivan et al., 2019; Shabayek & Spellerberg, 2018). Importantly, the discontinuation of antenatal GBS screening was found to be significantly associated with an increase in rates of neonatal early‐onset GBS disease (Al Luhidan et al., 2019). Further, health care providers adopting the GBS screening approach have argued that approximately 50% of women whose neonates developed early‐onset GBS disease did not display any risk factors including GBS bacteriuria, neonatal early‐onset GBS disease following previous births, prolonged rupture of membranes, preterm labour or pyrexia in labour, decreasing the potential effect of the risk‐based approach (Gopal Rao, Townsend, et al., 2017; Hasperhoven et al., 2020). This is a significant number of women without risk factors whose neonates developed early‐onset GBS disease, indicating that a large number of neonatal infections could not be prevented using the risked‐based approach. In contrast, results from findings in other studies have shown that the risk‐based approach can be effective in reducing neonatal early‐onset GBS disease or keeping these rates stable (Braye et al., 2019; Chen et al., 2019).
Practitioners favouring the antenatal GBS screening approach highlight the high quality of counselling of women who are GBS colonized, whereby the screening approach allows adequate time to discuss implications and options for management as opposed to the risk‐based approach (Steer et al., 2020). Further, as there are scarcely time constrains when screening for GBS between 35 and 37 weeks gestation, susceptibility testing in case of a penicillin allergy can be conducted in women with a positive test result (Steer et al., 2020). The diagnosis with GBS colonization may cause dissonance for many women and affect their whole experience of pregnancy, labour and birth (Sharpe et al., 2015). In this regard, concerns of women and their partners have included: aspects of the woman's and neonate's health; potential risks, as well as implications of birth plans; the normal concept of birth within the MMC; and even the unease regarding the competence of midwives (Sharpe et al., 2015). When women were interviewed about the way the GBS positive result was communicated, the group of women who were given the information by the midwife via telephone indicated their worry and fear and stated that these feelings could have been avoided with the provision of the test result in person (Sharpe et al., 2015). Those findings suggest that the antenatal screening approach allows sufficient time for discussing the GBS topic and its implications, which is crucial for women in making an informed decision. Another factor that invoked controversial debate was limitations regarding universal culture screening in relation to the intermittent nature of GBS (Plainvert et al., 2017).
Some women who tested GBS positive in the third trimester were not colonized with GBS at the time of birth, indicating that they needlessly received prophylactic antibiotics (Plainvert et al., 2017). Other women did not receive intrapartum prophylactic antibiotics as a result of a GBS negative result in pregnancy, while antibiotics were required because the GBS status changed to positive at birth (Virranniemi et al., 2019). To minimize this problem, the Centers for Disease Control and Prevention (CDC) adjusted their recommendations of the time of the screening from 35–37 to 36–37 weeks and 6 day's gestation to avoid a decrease of the predictive value of the test (CDC, 2020). A further disadvantage of antenatal screening relates to long laboratory processes, taking approximately 72 h to yield a result, which may result in GBS‐colonized women not having antibiotics administered if preterm labour occurs (Carrillo‐Ávila et al., 2018). In recent years, international research has examined the development of a more efficient method for timely detection of GBS, resulting in trialling rapid Polymerase Chain Reaction test methods, which is hoped to provide a faster alternative (Carrillo‐Ávila et al., 2018; Fullston et al., 2019).
4.3. Adherence to IAP
Across the entire population of the current study, close to three quarters of women were administered IAP where it was indicated by a positive GBS screening result, which is comparable to previous research (Braye et al., 2019; Gopal Rao, Nartey, et al., 2017; Moorhead et al., 2019). The discrepancies in adherence rates to IAP guidelines between the two models of care, MGP groups at each hospital and subgroups, were again not able to be related to contemporary literature due to lack of existing studies. However, these findings reflect variations in international studies with relatively high adherence rates (Braye et al., 2019; Gopal Rao, Nartey, et al., 2017; Kunze et al., 2015; Moorhead et al., 2019) and opposed findings of low rates (Yamaguchi & Ohashi, 2018). While adherence rates in the current study were higher in the NMMC when compared with the MMC, remarkably low rates were identified in the groups of the CMP and PM, and the lowest in a MGP cohort of one regional hospital. This finding is consistent with research undertaken in the MMC by Yamaguchi and Ohashi (2018). Whereas these results cannot show contextual influences, possible reasons for this may include missed opportunities, knowledge gaps, and, as discussed above, controversial views among midwives in the MMC. Further, concerns regarding overuse of antibiotics and their possible adverse effects on the neonatal microbiome are contemporary issues that are discussed below.
4.3.1. The question of overusing antibiotics and its adverse effects
Health professionals continue to argue that antibiotics should be used wisely, particularly in the light of the growing concern of antibiotic resistance globally. In the context of invasive neonatal GBS infection, intrapartum antibiotic administration has been shown to reduce this risk by approximately 80% when combined with the antenatal screening approach (Morgan et al., 2020). Against this background, health professionals need to balance the risks of women receiving prophylactic antibiotics with the GBS screening strategy, compared with a risk‐based approach of refraining from the provision of antibiotics, to determine which approach should be implemented. In this regard, a wide range of evidence should be considered, such as the meta‐analysis by Hasperhoven et al. (2020), who found no association between using the screening approach and an increased use of antibiotics.
The literature has reported a clear risk of adverse effects including alterations to the foetal microbiome and antimicrobial resistance following antibiotic exposure (Seedat et al., 2017). However, consideration should be given to evidence suggesting that while antibiotic use can decrease the count of healthy Bifidobacterium in the microbiome of the neonate within the first 7 days of life, this count normalizes at 4 weeks (Corvaglia et al., 2016). Furthermore, long‐term effects, such as increased body mass index in early childhood, were not found to be associated with the use of GBS‐specific antibiotic prophylaxis (Metz et al., 2020). Another concern is the adverse effect of antibiotic resistance (Seedat et al., 2017). With intravenous penicillin as the first line of antibiotics followed by cefazolin and vancomycin (in cases of adverse reactions to penicillin) to prevent neonatal early‐onset GBS disease (Morgan et al., 2020), reports of microbial resistance particularly to the latter two antibiotic types have been documented (Hayes et al., 2020; Seki et al., 2015). While penicillin‐resistant GBS have been detected in Japanese patients' respiratory isolates, they were not isolated in maternal or neonatal GBS strains (Seki et al., 2015). Until now, GBS is susceptible to penicillin however, it cannot be predicted if and when GBS develops resistance to penicillin, highlighting the importance of microbiological stewardship (Hayes et al., 2020). To date, information about adverse effects following intrapartum GBS prophylaxis appears conflicted. Further research is required to examine the different positions and investigate effects in longitudinal studies.
4.4. Limitations
This study was limited to descriptive statistics and did not examine correlations between specific demographic characteristics, GBS colonization and adherence rates. Further, due to the lack of information it could not be established whether the GBS swab collection and laboratory techniques were performed adequately across all maternity settings, which could have been a contributing factor to variations of GBS colonization rates between the study cohorts.
5. CONCLUSION
This study revealed that adherence to the recommended clinical practice guidelines in Western Australia to prevent invasive neonatal GBS infection is lower among pregnant women cared for within the MMC when compared with pregnant women in the NMMC. This also includes the adherence to the protocol of administering IAP when indicated by a positive GBS screening result. Thus, it may be proposed that the MMC may reflect differing knowledge and perspectives of midwives which may impact on the adherence to GBS screening and management guidelines. Further, it appears that the concern of medicalisation of birth—in particular in the low‐risk pregnancy population—is an influencing factor in this regard. Additionally, it seems that pregnant women lack knowledge in relation to implications of GBS colonization in pregnancy, which may be a result of non‐standardized antenatal education across maternity care providers in Western Australia. Further conclusions can be drawn regarding growing concerns of antibiotic overuse and possibly resulting adverse effects impacting GBS screening adherence. Furthermore, specific GBS screening and management protocols may be recognized differently in their importance between maternity hospitals and are evaluated to a greater or lesser extent.
It is recommended that multifaceted educational interventions that are aimed at improving adherence to GBS screening guidelines and clinical practice for midwives are implemented. These may include regular handover meetings, on‐line learning modules, workshops or webinars targeted at optimizing specific knowledge in relation to GBS in pregnancy and strengthening communication skills for obtaining an informed consent for routine antenatal GBS screening. Regular evaluation of adherence to GBS screening guidelines in maternity care settings could be the follow‐up strategy to maintain improved adherence levels.
It is recommended that antenatal education in relation to GBS in pregnancy be standardized for all maternity care providers across Western Australia. Standardized educational material has the advantage of offering a coherent and complete set of information to every pregnant woman and may include the provision of equal sources of information such as pamphlets, posters and face‐to‐face sessions. Standardized antenatal GBS education will ensure that pregnant women receive the same information for making an informed decision in relation to antenatal GBS screening for the prevention of neonatal infection. This strategy could inform clinical practice guidelines across Western Australian maternity care providers to ensure effective implementation.
Further research in a qualitative capacity is needed to examine possible reasons why adherence rates are low in the MMC.
ETHICAL CONSIDERATIONS
Research protocols were forwarded to apply for multi‐centre ethical approval, governance and site authorisation as well as data custodian permission. The study was approved by a university's (REMS 2019‐01008) and the relevant Western Australian Human Research Ethics Committee (RGS0000003723). Obtained datasets were de‐identified and all data were handled following the requirements of the National Health and Medical Research Council (NHMRC) published in the National Statement on Ethical Conduct in Human Research 2007 (updated 2018). Confidentiality of organizations was preserved using numerical identifiers. Parental consent was not required.
CONFLICT OF INTEREST
The authors report no conflict of interest in this work.
AUTHOR CONTRIBUTIONS
Sabine Pangerl, Deborah Sundin, and Sadie Geraghty: Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. Involved in drafting the manuscript or revising it critically for important intellectual content; given final approval of the version to be published; each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1111/jan.15249.
5.1. ACKNOWLEDGEMENTS
Open access publishing facilitated by The University of Notre Dame Australia, as part of the Wiley ‐ The University of Notre Dame Australia agreement via the Council of Australian University Librarians. [Correction added on 19 May 2022, after first online publication: CAUL funding statement has been added.]
Pangerl, S. , Sundin, D. & Geraghty, S. (2022). Adherence to screening and management guidelines of maternal Group B Streptococcus colonization in pregnancy. Journal of Advanced Nursing, 78, 3247–3260. 10.1111/jan.15249
DATA AVAILABILITY STATEMENT
Data available on request from the authors.
REFERENCES
- Al Luhidan, L. , Madani, A. , Albanyan, E. A. , Al Saif, S. , Nasef, M. , AlJohani, S. , Madkhali, A. , Al Shaalan, M. , & Alalola, S. (2019). Neonatal Group B Streptococcal infection in a tertiary care hospital in Saudi Arabia: A 13‐year experience. The Pediatric Infectious Disease Journal, 38(7), 731–734. 10.1097/inf.0000000000002269 [DOI] [PubMed] [Google Scholar]
- Alshengeti, A. , Alharbi, A. , Alraddadi, S. , Alawfi, A. , & Aljohani, B. (2020). Knowledge, attitude and current practices of pregnant women towards Group B Streptococcus screening: Cross‐sectional study, Al‐Madinah, Saudi Arabia. BMJ Open, 10(2), e032487. 10.1136/bmjopen-2019-032487 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson, A. S. , Trumble, B. C. , Hové, C. , Kraft, T. S. , Kaplan, H. , Gurven, M. , & Blackwell, A. D. (2020). Old friends and friendly fire: Pregnancy, hookworm infection, and anemia among tropical horticulturalists. American Journal of Human Biology, 32(2), e23337. 10.1002/ajhb.23337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashary, N. , Singh, A. , Chhabria, K. , & Modi, D. (2020). Meta‐analysis on prevalence of vaginal Group B Streptococcus colonization and preterm births in India. The Journal of Maternal‐Fetal & Neonatal Medicine, 33, 1–9. 10.1080/14767058.2020.1813705 [DOI] [PubMed] [Google Scholar]
- Berardi, A. , Rossi, C. , Bacchi Reggiani, M. L. , Bastelli, A. , Capretti, M. G. , Chiossi, C. , Fiorini, V. , Gambini, L. , Gavioli, S. , Lanari, M. , Memo, L. , Papa, I. , Pini, L. , Rizzo, M. V. , Zucchini, A. , Facchinetti, F. , & Ferrari, F. (2017). An area‐based study on intrapartum antibiotic prophylaxis for preventing Group B Streptococcus early‐onset disease: Advances and limitations. The Journal of Maternal‐Fetal & Neonatal Medicine, 30(14), 1739–1744. 10.1080/14767058.2016.1224832 [DOI] [PubMed] [Google Scholar]
- Bergin, T. (2018). In Seaman J. (Ed.), An introduction to data analysis (1st ed.). Sage Publications Ltd. [Google Scholar]
- Braye, K. , Foureur, M. , de Waal, K. , Jones, M. , Putt, E. , & Ferguson, J. (2019). Group B Streptococcal screening, intrapartum antibiotic prophylaxis, and neonatal early‐onset infection rates in an Australian local health district: 2006–2016. PLoS One, 14(4), 1–15. 10.1371/journal.pone.0214295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carrillo‐Ávila, J. A. , Gutiérrez‐Fernández, J. , González‐Espín, A. I. , García‐Triviño, E. , & Giménez‐Lirola, L. G. (2018). Comparison of qPCR and culture methods for Group B Streptococcus colonization detection in pregnant women: Evaluation of a new qPCR assay. BMC Infectious Diseases, 18(1), 305–313. 10.1186/s12879-018-3208-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC . (2020). Prevention of Group B Streptococcal early‐onset disease in newborns. Centers for Disease Control and Prevention. https://www.acog.org/clinical/clinical‐guidance/committee‐opinion/articles/2020/02/prevention‐of‐group‐b‐streptococcal‐early‐onset‐disease‐in‐newborns [Google Scholar]
- Chen, J. C. , Jenkins‐Marsh, S. , Flenady, V. , Ireland, S. , May, M. , Grimwood, K. , & Liley, H. G. (2019). Early‐onset Group B Streptococcal disease in a risk factor‐based prevention setting: A 15‐year population‐based study. Australian and New Zealand Journal of Obstetrics and Gynaecology, 59(3), 422–429. 10.1111/ajo.12891 [DOI] [PubMed] [Google Scholar]
- Corvaglia, L. , Tonti, G. , Martini, S. , Aceti, A. , Mazzola, G. , Aloisio, I. , Di Gioia, D. , & Faldella, G. (2016). Influence of intrapartum antibiotic prophylaxis for Group B Streptococcus on gut microbiota in the first month of life. Journal of Pediatric Gastroenterology and Nutrition, 62(2), 304–308. 10.1097/MPG.0000000000000928 [DOI] [PubMed] [Google Scholar]
- Dalmartello, M. , Parazzini, F. , Pedron, M. , Pertile, R. , Collini, L. , La Vecchia, C. , & Piffer, S. (2019). Coverage and outcomes of antenatal tests for infections: A population based survey in the province of Trento, Italy. The Journal of Maternal‐Fetal & Neonatal Medicine, 32(11), 2049–2055. 10.1080/14767058.2018.1424822 [DOI] [PubMed] [Google Scholar]
- De Luca, C. , Buono, N. , Santillo, V. , Licameli, A. , Straface, G. , Scambia, G. , & De Santis, M. (2016). Screening and management of maternal colonization with Streptococcus agalactiae: An Italian cohort study. The Journal of Maternal‐Fetal & Neonatal Medicine, 29(6), 911–915. 10.3109/14767058.2015.1023188 [DOI] [PubMed] [Google Scholar]
- Edwards, J. M. , Watson, N. , Focht, C. , Wynn, C. , Todd, C. A. , Walter, E. B. , Heine, R. P. , & Swamy, G. K. (2019). Group B Streptococcus (GBS) colonization and disease among pregnant women: A historical cohort study. Infectious Diseases in Obstetrics and Gynecology, 2019, 2–6. doi: 10.1155/2019/5430493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fullston, E. F. , Doyle, M. J. , Higgins, M. F. , & Knowles, S. J. (2019). Clinical impact of rapid polymerase chain reaction (PCR) test for Group B Streptococcus (GBS) in term women with ruptured membranes. Irish Journal of Medical Science, 188(4), 1269–1274. 10.1007/s11845-019-01977-x [DOI] [PubMed] [Google Scholar]
- Furfaro, L. L. , Chang, B. J. , & Payne, M. S. (2019). Detection of Group B Streptococcus during antenatal screening in Western Australia: A comparison of culture and molecular methods. Journal of Applied Microbiology, 127(2), 598–604. 10.1111/jam.14331 [DOI] [PubMed] [Google Scholar]
- Gopal Rao, G. , Hiles, S. , Bassett, P. , & Lamagni, T. (2019). Differential rates of Group B Streptococcus (GBS) colonization in pregnant women in a racially diverse area of London, UK: A cross‐sectional study. BJOG: An International Journal of Obstetrics & Gynaecology, 126(11), 1347–1353. 10.1111/1471-0528.15648 [DOI] [PubMed] [Google Scholar]
- Gopal Rao, G. , Nartey, G. , McAree, T. , O'Reilly, A. , Hiles, S. , Lee, T. , Wallace, S. , Batura, R. , Khanna, P. , Abbas, H. , Tilsed, C. , Nicholl, R. , Lamagni, T. , & Bassett, P. (2017). Outcome of a screening programme for the prevention of neonatal invasive early‐onset Group B Streptococcus infection in a UK maternity unit: An observational study. BMJ Open, 7(4), 1–7. 10.1136/bmjopen-2016-014634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gopal Rao, G. , Townsend, J. , Stevenson, D. , Nartey, G. , Hiles, S. , Bassett, P. , Lamagni, T. , & Nicholl, R. (2017). Early‐Onset Group B Streptococcus (EOGBS) infection subsequent to cessation of screening‐based intrapartum prophylaxis: Findings of an observational study in West London, UK. BMJ Open, 7(11), 1–6. 10.1136/bmjopen-2017-018795 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasperhoven, G. F. , Al‐Nasiry, S. , Bekker, V. , Villamor, E. , & Kramer, B. (2020). Universal screening versus risk‐based protocols for antibiotic prophylaxis during childbirth to prevent early‐onset Group B Streptococcal disease: A systematic review and meta‐analysis. BJOG: An International Journal of Obstetrics and Gynaecology, 127, 1–12. 10.1111/1471-0528.16085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes, K. , O'Halloran, F. , & Cotter, L. (2020). A review of antibiotic resistance in Group B Streptococcus: The story so far. Critical Reviews in Microbiology, 46(3), 253–269. 10.1080/1040841X.2020.1758626 [DOI] [PubMed] [Google Scholar]
- Heath, P. T. , & Jardine, L. A. (2014). Neonatal infections: Group B Streptococcus. BMJ Clinical Evidence, 0323, 1–9. https://www.ncbi.nlm.nih.gov/pubmed/24580886 [PMC free article] [PubMed] [Google Scholar]
- Hegarty, J. , Murphy, S. , Creedon, S. , Wills, T. , Savage, E. , Barry, F. , Smiddy, M. , Coffey, A. , Burton, A. , O'Brien, D. , Horgan, S. , Nibhuachalla, C. , Brennan, C. , Agreli, H. , & Drennan, J. (2019). Leadership perspective on the implementation of guidelines on healthcare‐associated infections. BMJ Leader, 3(2), 43–51. 10.1136/leader-2018-000111 [DOI] [Google Scholar]
- HogenEsch, E. , De Mucio, B. , Haddad, L. B. , Vilajeliu, A. , Ropero, A. M. , Yildirim, I. , & Omer, S. B. (2020). Differences in maternal Group B Streptococcus screening rates in Latin American countries. Vaccine, 39, B3–B11. 10.1016/j.vaccine.2020.10.082 [DOI] [PubMed] [Google Scholar]
- Homer, C. S. , Scarf, V. , Catling, C. , & Davis, D. (2014). Culture‐based versus risk‐based screening for the prevention of Group B Streptococcal disease in newborns: A review of national guidelines. Women and Birth, 27(1), 46–51. 10.1016/j.wombi.2013.09.006 [DOI] [PubMed] [Google Scholar]
- Hunter, A. , Devane, D. , Houghton, C. , Grealish, A. , Tully, A. , & Smith, V. (2017). Woman‐centred care during pregnancy and birth in Ireland: Thematic analysis of women’s and clinicians’ experiences. BMC Pregnancy and Childbirth, 17(1). 10.1186/s12884-017-1521-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jisuvei, S. C. , Osoti, A. , & Njeri, M. A. (2020). Prevalence, antimicrobial susceptibility patterns, serotypes and risk factors for Group B Streptococcus rectovaginal isolates among pregnant women at Kenyatta National Hospital, Kenya: A cross‐sectional study. BMC Infectious Diseases, 20(1), 302. 10.1186/s12879-020-05035-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kunze, M. , Zumstein, K. , Markfeld‐Erol, F. , Elling, R. , Lander, F. , Prömpeler, H. , Berner, R. , & Hufnagel, M. (2015). Comparison of pre‐ and intrapartum screening of Group B Streptococci and adherence to screening guidelines: A cohort study. European Journal of Pediatrics, 174(6), 827–835. 10.1007/s00431-015-2548-y [DOI] [PubMed] [Google Scholar]
- Kwatra, G. , Cunnington, M. C. , Merrall, E. , Adrian, P. V. , Ip, M. , Klugman, K. P. , Tam, W. H. , & Madhi, S. A. (2016). Prevalence of maternal colonization with Group B Streptococcus: A systematic review and meta‐analysis. The Lancet Infectious Diseases, 16(9), 1076–1084. 10.1016/s1473-3099(16)30055-x [DOI] [PubMed] [Google Scholar]
- Lao, T. T. (2019). Epidemiological factors impact Group B Streptococcus carriage. BJOG: An International Journal of Obstetrics & Gynaecology, 126(11), 1353. 10.1111/1471-0528.15871 [DOI] [PubMed] [Google Scholar]
- Lee, S. , Holden, D. , Webb, R. , & Ayers, S. (2019). Pregnancy related risk perception in pregnant women, midwives and doctors: A cross‐sectional survey. BMC Pregnancy and Childbirth, 19(1), 335. 10.1186/s12884-019-2467-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McQuaid, F. , Jones, C. , Stevens, Z. , Plumb, J. , Hughes, R. , Bedford, H. , Voysey, M. , Heath, P. T. , & Snape, M. D. (2016). Factors influencing women's attitudes towards antenatal vaccines, Group B Streptococcus and clinical trial participation in pregnancy: An online survey. BMJ Open, 6(4), 1–9. 10.1136/bmjopen-2015-010790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McQuaid, F. , Pask, S. , Locock, L. , Davis, E. , Stevens, Z. , Plumb, J. , & Snape, M. D. (2016). Attitudes towards antenatal vaccination, Group B Streptococcus and participation in clinical trials: Insights from focus groups and interviews of parents and healthcare professionals. Vaccine, 34(34), 4056–4061. 10.1016/j.vaccine.2016.06.024 [DOI] [PubMed] [Google Scholar]
- Metz, T. D. , McKinney, J. , Allshouse, A. A. , Knierim, S. D. , Carey, J. C. , & Heyborne, K. D. (2020). Exposure to Group B Streptococcal antibiotic prophylaxis and early childhood body mass index in a vaginal birth cohort. The Journal of Maternal‐Fetal & Neonatal Medicine, 33(19), 3318–3323. 10.1080/14767058.2019.1571575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Millington, S. , Arstall, M. , Dekker, G. , Magarey, J. , & Clark, R. (2020). Adherence to clinical practice guidelines for south Australian pregnant women with cardiac conditions between 2003 and 2013. PLoS One, 15(3), 1–19. 10.1371/journal.pone.0230459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moorhead, R. , Daley, A. J. , Lee, L.‐Y. , Gorelik, A. , & Garland, S. M. (2019). Compliance with screening for and recommended management of maternal Group B Streptococcus carriage in pregnancy. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 59(6), 837–842. 10.1111/ajo.12977 [DOI] [PubMed] [Google Scholar]
- Morgan, J. A. , Zafar N., & Cooper D.B. (2020). Group B Streptococcus and pregnancy. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482443/ [PubMed] [Google Scholar]
- Murray, P. R. , Rosenthal, K. S. , & Pfaller, M. A. (2016). Medical microbiology (8th ed.). Elsevier. [Google Scholar]
- National Health and Medical Research Council . (2018). National statement on ethical conduct in human research (2007) ‐ updated 2018. National Health and Medical Research Council, The Australian Research Council and Universities Australia. https://www.nhmrc.gov.au/about‐us/publications/national‐statement‐ethical‐conduct‐human‐research‐2007‐updated‐2018 [Google Scholar]
- O'Sullivan, C. P. , Lamagni, T. , Patel, D. , Efstratiou, A. , Cunney, R. , Meehan, M. , Ladhani, S. , Reynolds, A. J. , Campbell, R. , Doherty, L. , Boyle, M. , Kapatai, G. , Chalker, V. , Lindsay, D. , Smith, A. , Davies, E. , Jones, C. E. , & Heath, P. T. (2019). Group B Streptococcal disease in UKand Irish infants younger than 90 days, 2014–15: A prospective surveillance study. The Lancet Infectious Diseases, 19(1), 83–90. 10.1016/S1473-3099(18)30555-3 [DOI] [PubMed] [Google Scholar]
- Pangerl, S. , Sundin, D. , & Geraghty, S. (2021). Group B Streptococcus screening guidelines in pregnancy: A critical review of compliance. Maternal Child Health Journal, 25(2), 257–267. 10.1007/s10995-020-03113-z [DOI] [PubMed] [Google Scholar]
- Philip, S. , Woodward‐Kron, R. , Manias, E. , & Noronha, M. (2019). Overseas qualified Nurses' (OQNs) perspectives and experiences of intraprofessional and nurse‐patient communication through a community of practice lens. Collegian (Royal College of Nursing, Australia), 26(1), 86–94. 10.1016/j.colegn.2018.04.002 [DOI] [Google Scholar]
- Plainvert, C. , El Alaoui, F. , Tazi, A. , Joubrel, C. , Anselem, O. , Ballon, M. , Frigo, A. , Branger, C. , Mandelbrot, L. , Goffinet, F. , & Poyart, C. (2017). Intrapartum Group B Streptococcus screening in the labor ward by Xpert® GBS real‐time PCR. European Journal of Clinical Microbiology & Infectious Diseases, 37(2), 265–270. 10.1007/s10096-017-3125-2 [DOI] [PubMed] [Google Scholar]
- Ramesh Babu, S. , McDermott, R. , Farooq, I. , Le Blanc, D. , Ferguson, W. , McCallion, N. , Drew, R. , & Eogan, M. (2017). Screening for Group B Streptococcus (GBS) at labour onset using PCR: Accuracy and potential impact ‐ A pilot study. Journal of Obstetrics & Gynaecology, 37(6), 1–6. 10.1080/01443615.2017.1328490 [DOI] [PubMed] [Google Scholar]
- Rao, G. G. , & Khanna, P. (2020). To screen or not to screen women for Group B Streptococcus (Streptococcus agalactiae) to prevent early onset sepsis in newborns: Recent advances in the unresolved debate. Therapeutic Advances in Infectious Disease, 7, 1–7. 10.1177/2049936120942424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rotelli, M. D. (2015). Ethical considerations for increased transparency and reproducibility in the retrospective analysis of health care data. Therapeutic Innovation & Regulatory Science, 49(3), 342–347. 10.1177/2168479015578155 [DOI] [PubMed] [Google Scholar]
- Seale, A. C. , Bianchi‐Jassir, F. , Russell, N. J. , Kohli‐Lynch, M. , Tann, C. J. , Hall, J. , Madrid, L. , Blencowe, H. , Cousens, S. , Baker, C. J. , Bartlett, L. , Cutland, C. , Gravett, M. G. , Heath, P. T. , Ip, M. , Le Doare, K. , Madhi, S. A. , Rubens, C. E. , Saha, S. K. , ..., & Lawn, J. E. (2017). Estimates of the burden of Group B Streptococcal disease worldwide for pregnant women, stillbirths, and children. Clinical Infectious Diseases, 65(suppl_2), 200–219. 10.1093/cid/cix664 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seedat, F. , Stinton, C. , Patterson, J. , Geppert, J. , Tan, B. , Robinson, E. R. , McCarthy, N. D. , Uthman, O. A. , Freeman, K. , Johnson, S. A. , Fraser, H. , Brown, C. S. , Clarke, A. , & Taylor‐Phillips, S. (2017). Adverse events in women and children who have received intrapartum antibiotic prophylaxis treatment: A systematic review. BMC Pregnancy and Childbirth, 17(1), 247. 10.1186/s12884-017-1432-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seki, T. , Kimura, K. , Reid, M. E. , Miyazaki, A. , Banno, H. , Jin, W. , Wachino, J. , Yamada, K. , & Arakawa, Y. (2015). High isolation rate of MDR Group B Streptococci with reduced penicillin susceptibility in Japan. Journal of Antimicrobial Chemotherapy, 70(10), 2725–2728. 10.1093/jac/dkv203 [DOI] [PubMed] [Google Scholar]
- Shabayek, S. , & Spellerberg, B. (2018). Group B Streptococcal colonization, molecular characteristics, and epidemiology. Frontiers in Microbiology, 9, 437. 10.3389/fmicb.2018.00437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharpe, M. , Dennis, K. , Cates, E. C. , Kehler, S. , & McGrath, K. (2015). Deconstructing dissonance: Ontario midwifery clients speak about their experiences of testing Group B Streptococcus‐positive. Canadian Journal of Midwifery Research & Practice, 14(2), 18–33. http://ezproxy.ecu.edu.au/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=122432303&site=ehost‐live&scope=site [Google Scholar]
- Sheehy, A. , Smith, R. M. , Gray, J. E. , & Homer, C. S. E. (2019). Midwifery pre‐registration education and mid‐career workforce participation and experiences. Women and Birth, 32(2), 182–188. 10.1016/j.wombi.2018.06.014 [DOI] [PubMed] [Google Scholar]
- Sherman, R. , & Cohn, T. (2019). Promoting professional accountability and ownership. American Nurse Today, 14(2), 24–26. https://www.myamericannurse.com/wp‐content/uploads/2019/02/ant2‐Accountability‐117.pdf [Google Scholar]
- Singh, T. , Barnes, E. H. , & Isaacs, D. (2019). Early‐onset neonatal infections in Australia and New Zealand, 2002–2012. Archives of Disease in Childhood ‐ Fetal and Neonatal Edition, 104(3), 248–252. 10.1136/archdischild-2017-314671 [DOI] [PubMed] [Google Scholar]
- Steer, P. J. , Russell, A. B. , Kochhar, S. , Cox, P. , Plumb, J. , & Gopal Rao, G. (2020). Group B Streptococcal disease in the mother and newborn‐a review. European Journal of Obstetrics & Gynecology and Reproductive Biology, 252, 526–533. 10.1016/j.ejogrb.2020.06.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szylit, N. A. , Malburg, F. L. , Piccinato, C. , de Paula Ferreira, L. A. , Podgaec, S. , & Zlotnik, E. (2020). Prevalence of rectovaginal colonization by Group B Streptococcus in pregnant women seen at prenatal care program of a health organization. Einstein (São Paulo), 18, 1–6. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1679‐45082020000100217&nrm=iso [DOI] [PMC free article] [PubMed] [Google Scholar]
- Virranniemi, M. , Raudaskoski, T. , Haapsamo, M. , Kauppila, J. , Renko, M. , Peltola, J. , Risteli, L. , & Laatio, L. (2019). The effect of screening‐to‐labor interval on the sensitivity of late‐pregnancy culture in the prediction of Group B Streptococcus colonization at labor: A prospective multicenter cohort study. Acta Obstetricia et Gynecologica Scandinavica, 98(4), 494–499. 10.1111/aogs.13522 [DOI] [PubMed] [Google Scholar]
- WA Department of Health . (2016). Midwives notification system – Data validation manual ‐ WA Health . https://healthywa.wa.gov.au/~/media/Files/Corporate/general%20documents/Data%20collection/PDF/MNS_Validation_Manual_2016_WA_Health.pdf
- WA Department of Health . (2019). Pregnancy care. Australian Government Department of Health. https://www.health.gov.au/resources/pregnancy‐care‐guidelines [Google Scholar]
- WHO . (2017). Immunizations, vaccines and biologicals. World Health Organization. https://www.who.int/immunization/newsroom/press/news_group_b_strep_stillbirths_infant_deaths_2017/en/ [Google Scholar]
- WHO . (2021). Health statistics and information systems ‐ Definition of regional groupings. World Health Organization. https://www.who.int/healthinfo/global_burden_disease/definition_regions/en/#:~:text=WHO%20regions%3A%20WHO%20Member%20States,each%20spreadsheet%20for%20more%20information [Google Scholar]
- Yamaguchi, K. , & Ohashi, K. (2018). Management of Group B Streptococcus‐positive pregnant women at maternity homes in Japan: A questionnaire survey of compliance among midwives. Maternal Health, Neonatology and Perinatology, 4(1), 1–6. 10.1186/s40748-017-0069-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data available on request from the authors.