
Figure 2: Acute left central retinal artery occlusion (CRAO) secondary to a left internal carotid artery stenosis.
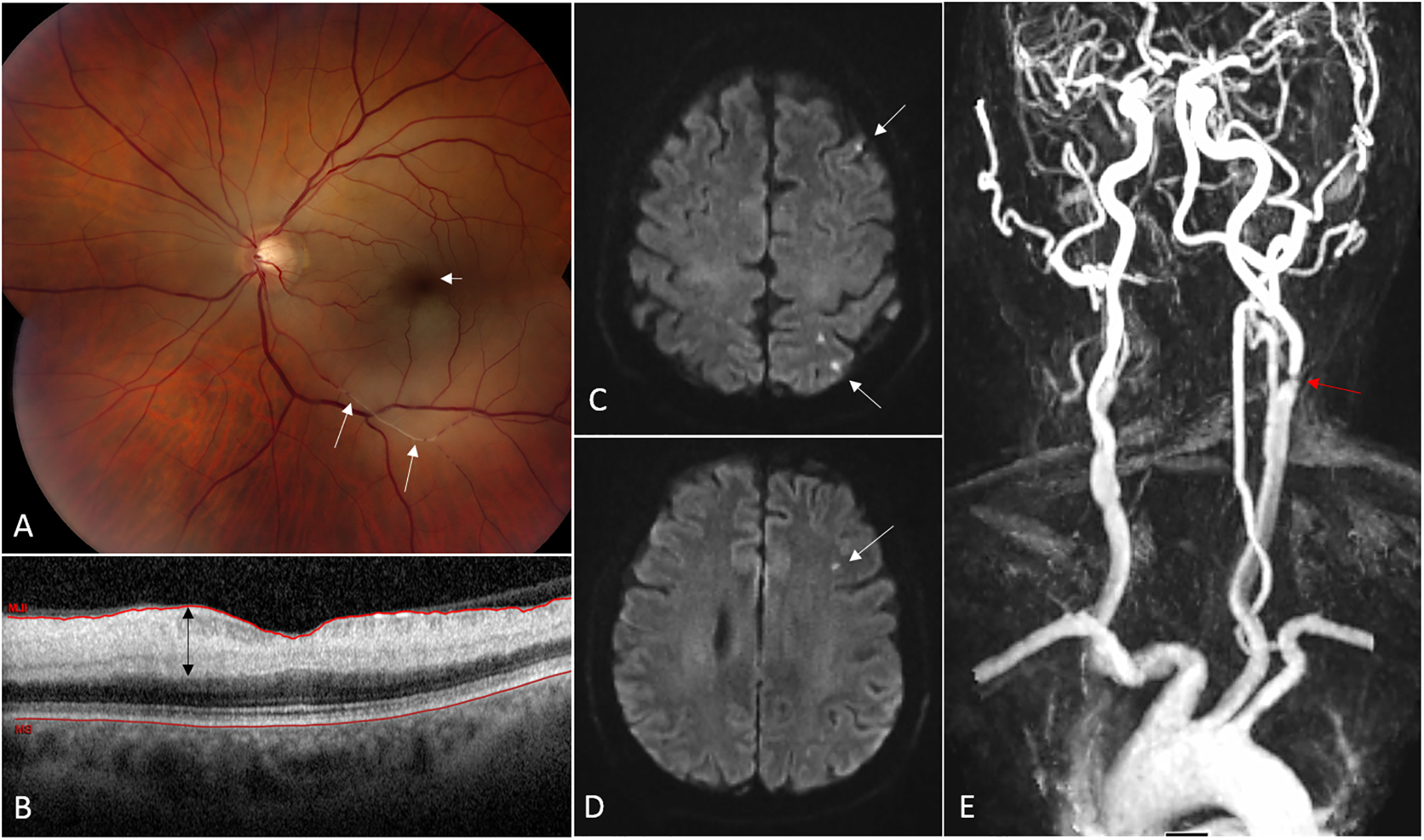
(A) Fundus photograph from a 68 year-old man with acute CRAO in the left eye. The ischemic retina appears whitish and the normally perfused fovea (from the choroidal circulation) is dark red in contrast, consistent with a so-called “cherry-red spot” (short arrow). Platelet-fibrin emboli are seen migrating in the inferior branches of the central retinal artery (long arrows). (B) Optical coherence tomography (OCT) of the macula showing a cut through the fovea. The ischemic inner retinal layers are thickened (black arrow) whereas the outer retinal layers are normal. (C, D) Brain MRI (axial cuts, diffusion-weighted images) performed 24 hours after onset of visual loss demonstrates multiple small acute areas of infarction as small hypersignals in the left hemisphere (arrows). (E) Magnetic resonance imaging (MRA) of the neck and great vessels shows a severe atheromatous stenosis at the origin of the left internal carotid artery.