
Figure 1.
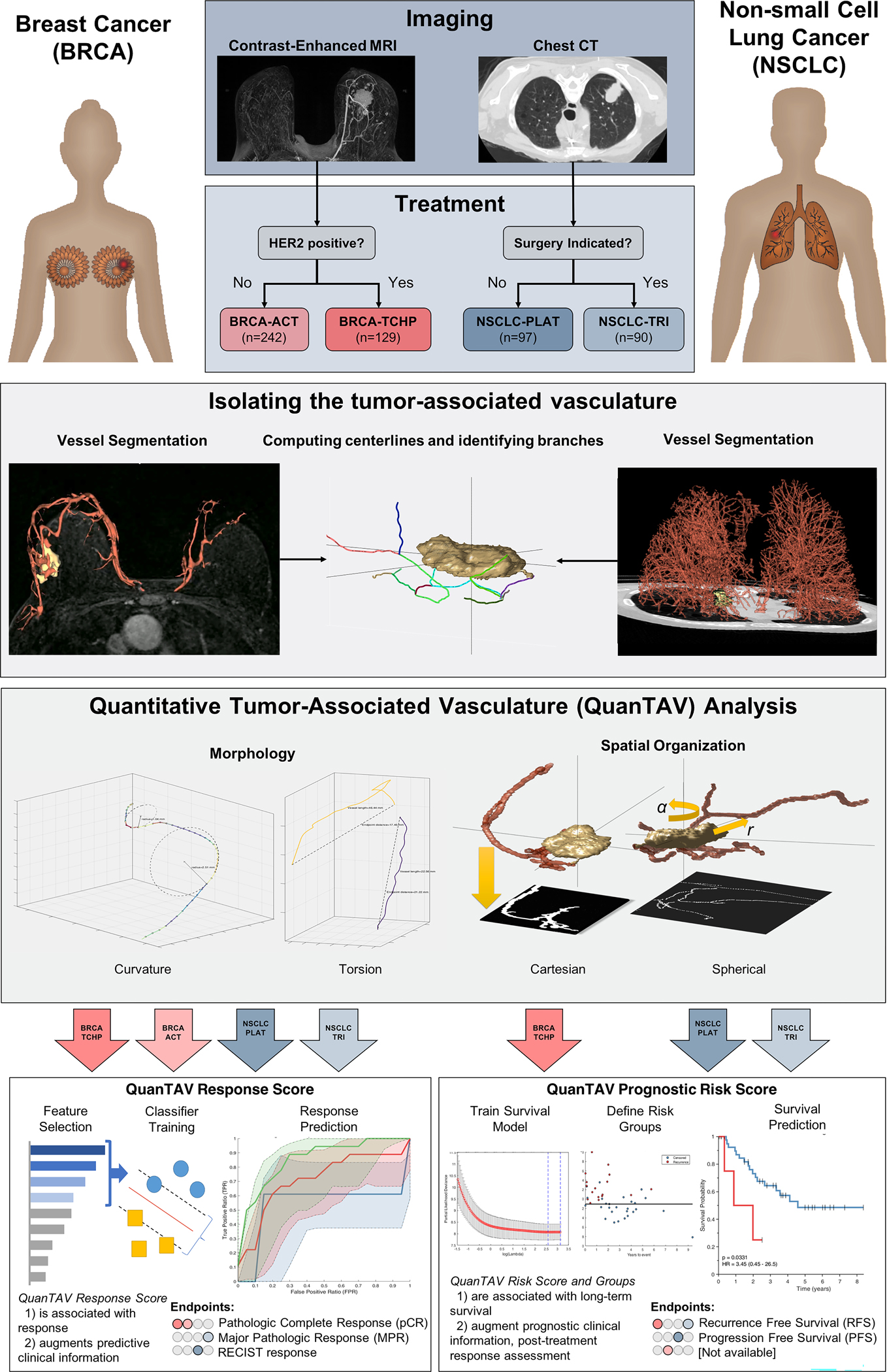
Overview of the development and validation of quantitative tumor-associated vasculature (QuanTAV) response and risk scores. Models were trained and validated in four therapeutic cohorts: anthracycline-based neoadjuvant chemotherapy [BRCA-ACT] and neoadjuvant chemotherapy with anti-HER2 agents [BRCA-TCHP] in breast cancer and platinum-based chemotherapy only [NSCLC-PLAT] and neoadjuvant chemoradiation with surgery [NSCLC-TRI] in non-small cell lung cancer. The tumor and associated-vasculature were extracted from pre-treatment breast DCE-MRI and chest CT. For each vessel network, centerlines were derived and two categories of QuanTAV features were computed: Morphology and Spatial Organization. QuanTAV morphology features quantified the shape of tumor vessels. Statistics describing the distribution of metrics such as curvature (inversely proportional to the radius of a circle fitting three adjacent vessel points) and torsion (detecting differences in vessel length relative to the distance between its start and end points) comprised the bulk of QuanTAV morphology features. QuanTAV Spatial Organization features evaluate the architecture of the vessel network by evaluating the degree of vessel alignment along 2D projection images depicting the position of vessels in either the imaging space (cartesian) or a coordinate system relative to the tumor center and surface (spherical). QuanTAV features were optimized to predict response in each training cohort, then a linear discriminant analysis (LDA) classifier was trained to predict response from a limited set of features selected by wilcoxon rank sum test. The classifier’s was the QuanTAV response score, which was assessed for independent ability to predict therapeutic response in the testing set. Likewise, in the three cohorts with progression- (NSCLC-PLAT) or recurrence-free survival (BRCA-ACT, NSCLC-TRI) data available, a regularized cox proportional hazards model was trained to derive a QuanTAV risk score and low/high risk groups in the training set, which were assessed for univariable and multivariable association with survival in the testing set.