

Correction: Chinese Medicine (2022) 17:99 https://doi.org/10.1186/s13020-022-00654-z
Following publication of the original article [1], the authors would like to make corrections after identifying the errors below which were caused by typo mistakes and the latest update of data analysis prior to publication but updating on some texts and Fig. 6A correspondingly had been missed. These changes will not impact the results nor alter the conclusion of this study.
Correction (1): Clinical symptoms, diagnosis and health conditions during hospitalization
Published version: Fever, fatigue, and dry cough were the most common symptoms, exhibiting in 59.3% (89 of 150), 55.3% (83 of 150), and 46.67% (69 of 150) participants, respectively.
Corrected version: Fever, fatigue, and dry cough were the most common symptoms, exhibiting in 59.3% (89 of 150), 55.3% (83 of 150), and 46.67% (70 of 150) participants, respectively.
Reason for correction: it is a typo mistake made by the authors.
Correction (2): Improvement in 6MWT performance
Published version: However, with each increased age year, the distance achieve in 6MWT will decrease by 1.03 m.
Corrected version: However, with each increased age year, the distance achieve in 6MWT will decrease by 0.961 m.
Reason for correction: texts were not updated upon the latest update in data analysis with changes in linear mixed model equation. The authors believe it is necessary to correct the numerical values in text even though the change doesn’t impact on the findings. The corresponding data in Table 9 is correct and do not require any change.
Correction (3): Lowered risk of COPD
Published version: However, with each increased age year, the score obtained in LFQ will decrease by 0.11.
Corrected version: The statement “However, with each increased age year, the score obtained in LFQ will decrease by 0.11” has been removed.
Reason for correction: texts were not updated upon the latest update in data analysis with changes in linear mixed model equation. Although the statement would be correct under another calculation, it is no longer valid under the Model 2 calculation as published in the current article and serves no argument or discussion in this study. The authors believe that removing the statement can avoid inaccuracy and confusions.
Correction (4): Fig. 6(A)
Reason for correction: The authors identified an error in Fig. 6A which the graph was resulted from an earlier data analysis and was not from the latest one. The corresponding texts referring to this graph are correct and do not require any change.
Fig. 6.
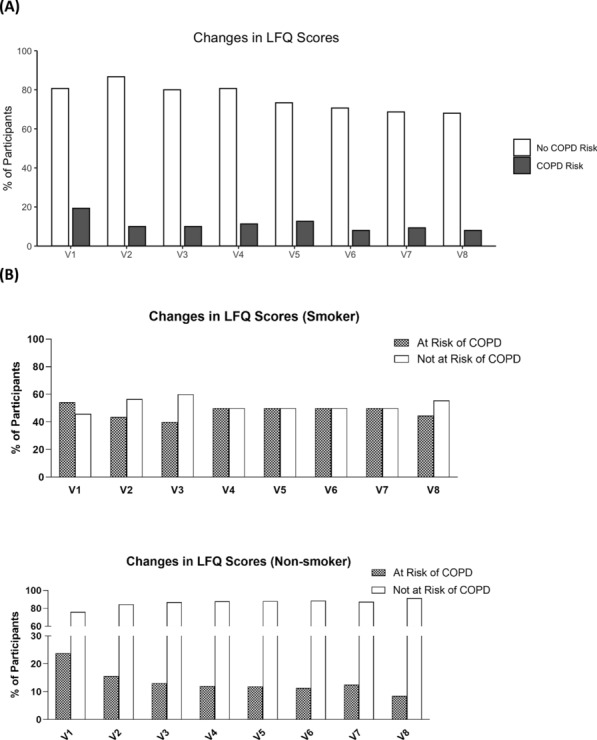
A Figure showed the percentage of participants with risk of COPD as accessed by their LFQ Scores. B Showed the percentage of non-smokers and smokers participants with risk of COPD
The original article [1] has been corrected.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Linda Li-Dan Zhong, Email: ldzhong@hkbu.edu.hk.
Zhao-Xiang Bian, Email: bzxiang@hkbu.edu.hk.
Reference
- 1.Zhong LL-D, Wong Y-P, Leung C-Y, Peng B, Lin Z-X, Taam VC-WW, Luo Y, Chen H-Y, Chao C-D, Wong C-F, Tam FS-C, Chan K, Lee K-Y, Ho L-F, Wong AY-L, Choy C-F, Ng BF-L, Wong RH-W, Feng Y-B, Liong C, Bian Z-X, COVID-19 CM Research Working Group Effects of Chinese medicine for COVID-19 rehabilitation: a multicenter observational study. Chin Med. 2022;17:99. doi: 10.1186/s13020-022-00654-z. [DOI] [PMC free article] [PubMed] [Google Scholar]