

Abstract
Background:
Despite recommendations to integrate palliative care into nursing home care, little is known about the most effective ways to meet this goal.
Objective:
To examine the characteristics and effectiveness of multicomponent nursing home palliative care interventions.
Design:
Systematic review
Methods:
We searched MEDLINE via PubMed, Embase, CINAHL, and Cochrane Library’s CENTRAL for clinical trials from inception through January 2019. We assessed the type of intervention, outcomes, and the risk of bias in included studies.
Results:
We screened 1167 records for eligibility and included 13 articles. Trials used usual care and or an active comparator as the control condition. Most interventions focused on staff education/training strategies and implementing a palliative care team. Several integrated advance care planning initiatives into the intervention. We found that palliative care interventions in nursing homes may enhance palliative care practices including processes to assess and manage pain and symptoms. However inconsistent outcomes and high or unclear risk of bias among the majority of studies requires results to be interpreted with caution.
Conclusions and Implications:
Our systematic review revealed that evidence for nursing home palliative care interventions is sparse.
Keywords: nursing homes, clinical trials, palliative care, end-of-life care, interventions
Brief Summary:
We conducted a systematic review to examine the characteristics and effectiveness of multicomponent nursing home palliative care interventions. We found 13 unique clinical trials. In six trials, interventions enhanced nursing home palliative care processes including increased use of care pathways, higher hospice referrals, and better documentation of pain and symptom assessment and management. However, in most trials there was mixed or insufficient evidence about the effect of palliative care interventions on reducing potentially burdensome care, resident/surrogate symptom ratings, advance care planning discussions and documentation, and improving family members’ evaluation of care. Our findings suggest there is limited evidence that palliative care interventions improve nursing home end-of-life care outcomes.
Introduction
Over the past two decades, palliative care services have grown dramatically to meet the healthcare needs of an aging population and the growing burden of serious illness. Palliative care is an interdisciplinary, patient-and family-centered approach to serious illness that incorporates symptom management, open communication, and informed decision making to elicit patients’ and families’ goals of care and preferences for treatments. Its goal is to relieve suffering and improve quality of life by addressing the myriad of physical, psychosocial, and spiritual needs of persons with serious, progressive illness.1 An expanding body of literature demonstrates that palliative care programs improve patient outcomes, optimize the use of healthcare resources, and enhance family and caregiver evaluation of care.2-4 However, much of the research has focused on home, hospital, and outpatient clinic settings.5,6
Evidence-based nursing home palliative care services are essential to enhance high quality end-of-life care. Close to 30% of older adults receive care in nursing homes until their death7 and experience untreated pain and other physical symptoms.8 Dying residents often report loneliness, depression, and limited support with spiritual needs.9 Many undergo potentially burdensome treatments with little benefit.10-12
The majority of published literature about palliative care programs in nursing homes is anecdotal or observational.13-16 A 2010 Cochrane Collaborative systematic review found few studies of palliative care interventions in nursing homes that were of high quality to assess outcomes.17 Continued growth of nursing home palliative care programs in the last several years18-20 requires analysis of new literature to expand on the earlier review by Hall et al.17 We therefore conducted a systematic review of multicomponent palliative care clinical trials in nursing homes to examine the characteristics and effectiveness of program interventions.
Methods
Search Strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) in this review.21 We searched MEDLINE, Embase, CINAHL, and Cochrane CENTRAL from inception to January 1, 2019 using (""palliative nursing"" OR ""palliative care""[Mesh] OR ""palliative""[tiab] AND ""care"" [tiab] OR ""palliative care"" [tiab]) AND ""nursing homes""[Mesh]). A health sciences librarian assisted us as we developed, piloted, and executed the searches. Literature searches excluded pediatric, non–English-language articles, commentaries, conference abstracts, letters, notes, and news. We hand searched the reference lists of all included articles to identify additional trials that met our eligibility criteria.
Study Eligibility
We defined study eligibility using the PICO (Patient, Problem or Population; Intervention; Comparison, Control or Comparator; Outcome) framework (Table 1).22 We included clinical trials of palliative care interventions focused on individuals receiving care in a nursing home and/or their family caregivers. Initially, we planned to include interventions if they incorporated at least one of eight palliative care domains as defined by the National Consensus Project’s Clinical Practice Guidelines for Quality Palliative Care.1 However, we later modified our inclusion criteria to include only multiple component interventions (defined as clearly integrating more than one palliative care domain).6,23 Trials had to incorporate a comparison condition (e.g., usual care, attention control, historical control, waitlist). We only included trials that reported on at least one of six outcomes: healthcare use, symptoms, resident or family evaluation of the quality of care, advance care planning, quality of life, and costs/expenditures.
Table 1.
Patient, Problem or Population; Intervention; Comparison, Control or Comparator; Outcome (PICO) Criteria
| Population | Inclusion: Individuals receiving care in a nursing home that provides healthcare services, skilled nursing, and medical care. |
| Exclusion: Assisted living residential care, continuing care retirement communities | |
| Intervention | Inclusion: Two or more of the following 8 domains:
|
| Exclusion: Observational study, interventions focused on a single component of palliative care (e.g., advance care planning or pain management) | |
| Comparator | Inclusion: Any comparison group including usual care, attention control, waitlist, historical control |
| Exclusion: No comparator | |
| Outcomes | Inclusion: One or more of the following patient/family focused outcomes: healthcare use, symptom management, resident or family evaluation of the quality of care, advance care planning, quality of life, and costs/expenditures. |
| Exclusion: Staff focused outcomes; practice environment changes |
PC=palliative care; ACP = advance care planning; NH = nursing home; ED= emergency department
Authors screened each article abstract for eligibility, then two reviewers independently appraised the full text of each eligible article using our inclusion/exclusion criteria to ensure appropriateness for the study. We resolved disagreements by consulting with a third author.
Data Extraction and Bias Assessment
We developed and piloted a structured abstraction tool to record evidence from each study. Two reviewers independently evaluated each report and extracted data (Table 2). We also rated risk of bias using a tool informed by the Cochrane Collaboration that included five categories: random sequence generation, allocation concealment, blinding of outcomes assessment, incomplete outcomes data, and selective reporting.24 If a study scored low on 4-5 of 5 categories, it was judged to have an overall low risk of bias; studies that scored high on 2-5 of 5 categories were judged overall high risk of bias; studies with unclear risk of bias or if assessment was not applicable (such as random sequence generation in a trial comparing an intervention to a historical control group) on 2-5 of 5 categories were judged overall unclear risk of bias.
Table 2.
Table of Evidence
| Reference | Intervention Domain |
Design | Description | Main Findings |
|---|---|---|---|---|
| Agar et al, 2017 PLOS one (Australia) | Structure and processes of care Ethical and legal aspects of care |
Design: Two arm, parallel cluster RCT Randomized at the NH level Population: People with advanced dementia and their families and professional caregivers in 20 NHs Dates: Feb 2013 - Dec 2014 Primary Measures Surrogate rated Comfort Assessment in Dying with Dementia; CAD–EOLD, Symptom Management at the End of life in Dementia; SM–EOLD, Satisfaction with Care at the End of life in Dementia; SWC–EOLD Secondary Measures: Proxy Nurse-rated CAD-EOLD, SM-EOLD, and Quality of Life in Late-stage Dementia (QUALID) Scale, rates of potentially inappropriate non-palliative interventions, rates of inappropriate acute care, nursing home staff ’s attitudes to, knowledge of and confidence in providing palliative/EOL care to residents with advanced dementia. |
Intervention: NH(n=10) ∣ Residents(n=156) Facilitated family case conferences (FCC) and staff palliative care training. Palliative Care nurse Planning Coordinator in facility for 16 hours per week over 18 months Control: NH(n=10) ∣ Residents(n=130) Usual care |
Healthcare Use
|
| Berkowitz et al, 2011 JAGS (Boston, MA, USA) | Structure and processes of care Physical aspects of care Ethical and legal aspects of care |
Design: Two arm prospective Quasi-experimental trial (historical control group) Population: Residents of one 50-bed skilled nursing unit (short term care) Dates: Control: June 2008 to May 2009 before the intervention started; Intervention Jun 2009 - May 2010 Measures: Distribution of discharge dispositions, including readmission, transfer to long-term care facility, discharge to home, and death. |
Intervention: (n=862) Standardized physician admission template Goals of Care discussion template Automated Palliative Care consult if >3 hospitalizations in last 6 months and Interdisciplinary team conference every 2 weeks (cases of rehospitalization deemed potentially avoidable were reviewed and “lessons learned” email was shared with all staff after each meeting) Control: (n=863) Retrospective cohort |
Healthcare Use (intervention vs. control)
|
| Boogaard et al, 2018 Palliative Medicine (The Netherlands) | Structure and processes of care Care of the patient nearing the end of life |
Design: Three arm parallel cluster-RCT; triplets of NHs matched on number of psychogeriatric beds, presence of a palliative care unit, and urban/nonurban location; Randomized at the NH level Population: Family caregivers of deceased residents with dementia in 18 Dutch NHs psychogeriatric wards Dates: Pre-intervention phase January 2012- October 2012; Intervention: November 2012-July 2014 Measures: Bereaved family member rated End-of-Life in Dementia-Satisfaction With Care scale (EOLD-SWC) and the End-of-Life in Dementia-Comfort Assessment in Dying scale (EOLD-CAD) |
Intervention: Data feedback reports (derived from two dementia-specific family-reported tools) coupled with evidence-based suggestions to improve end-of-life care (1) Generic feedback strategy NH n=6∣Residents (n=123) NH teams receive and discuss targeted suggestions for care improvement strategies based on cumulative family-reported feedback (2) Patient-specific feedback strategy: NH n=4∣Residents(n=71) NH teams receive and discuss targeted suggestions for care improvement strategies based on individual family-reported feedback Control (3) Usual care : NH n=6 ∣ Residents(n=113) |
Symptoms
|
| Brännström et al, 2016 Palliative Medicine (Sweden) | Structure and processes of care Care of the patient nearing the end of life Physical aspects of care |
Design: Two arm quasi experimental exploratory, controlled before- and-after trial Population: Deceased residents in 19 residential care homes Dates: Jun 2009 – Oct 2011 Primary Measures: Edmonton Symptom Assessment System (ESAS) Secondary Measures: Views of Informal Carers – Evaluation of Services (VOICES) |
Intervention: (usual care n=64; intervention n=71) Usual care x 15 months, then Liverpool Care Pathway (LCP) for the Dying Patient (education and training for staff included 1) a 3-hour session about the LCP and EOL care for all assistant nurses, RNs and GPs; 2) a nurse who completed a 35-hour web-based LCP train-the-trainer course) Control: (usual care n=61; usual care n=64) Usual care X15 months, then usual care |
Symptoms
|
| Casarett et al, 2005 JAMA (Phila, PA, USA) | Structure and processes of care Care of the patient nearing the end of life Ethical and legal aspects of care |
Design: Two arm parallel RCT; randomized at patient level Population: NH residents and their surrogate decision makers in 3 NHs Dates: Dec 2003 – Dec 2004 Measures: Deaths, hospitalizations, new orders to limit life-sustaining treatment, hospice enrollment, bereaved family survey (Afterdeath Survey), surrogate rated: care in the last week of life, whether a member of the health care team discussed the resident’s prognosis with them and what to expect during the dying process, whether the resident had pain or shortness of breath that was not managed as well as it could have been, and whether the resident died where he/she would have wanted. |
Intervention: (n=107) Structured interview to identify residents whose goals for care, treatment, preferences, and PC needs are appropriate for hospice care → hospice informational visit Control: (n=98) Usual care |
Healthcare Use Intervention group more likely to (intervention vs control):
|
| Chapman and Toseland, 2007 (Northeastern USA) | Structure and processes of care Physical aspects of care Psychological and psychosocial aspects of care Social aspects of care |
Design: 2x2 randomized partial crossover trial; randomized in cohorts at patient level; crossover results not reported Population: NH residents with advanced dementia in 2 NHs Dates: Unclear; Random assignment done in cohorts over a 1 year period Measures: Cohen-Mansfield Agitation Inventory, Faces Legs Activity Cry Consolability, Cornell Scale for Depression in Dementia, Pain in Advanced Dementia (PAINAD) |
Intervention:(n= 57; after crossover n=118) Advanced Illness Care Teams (AICT) consisting of staff from medicine, nursing, social work, psychology, physical and occupational therapy, and nutrition. AICT met 5 times during an 8 week period to address 1) medical issues, 2) meaningful activities, 3) psychological problems, 4) behavioral concerns. ACP explicitly was not included in the intervention b/c investigators assessed that participating NHs “thoroughly addressed the ACP needs of residents during the admission and care planning process” Control: (n=61) Usual care; residents in usual care received the intervention after the 8-week measures were administered. |
Symptoms
|
| Comart et al, 2013 Gerontologist (Boston, MA, USA) | Structure and processes of care Physical aspects of care Psychological and psychosocial aspects of care Ethical and legal aspects of care Social Aspects of Care Spiritual, Religious, Existential Aspects of Care |
Design: Two arm Quasi-experimental trial (matched historical control group) Population: Deceased residents in 1 long term care facility Dates: 2006 – 2009 Control: Residents who died when the PC service didn’t exist (2006). Intervention: residents who died during the period of the PC service (2007–2009) Measures: Physician orders, medication use, hospital stays, ER visits, falls, shortness of breath, weight loss, depression, pain, delirium, pressure ulcers. |
Intervention: (n=125) Interdisciplinary Palliative Care Team: PC physician (0.6 fte), clinical nurse specialist (0.6 fte), chaplain (0.3 fte), social worker (0.5 fte), and a psychologist who also serves as the lead administrator for the program (1.0 fte): helping the family define the goals of care, providing expert pain management, or assisting families come to agreement on treatment options Control: (n=125) Retrospective cohort; usual care |
Healthcare Use
|
| Hanson et al, 2005 J Palliative Med (NC, USA) | Structure and processes of care Ethical and legal aspects of care Physical aspects of care |
Design: Two arm Quasi-experimental pre-post trial; “control” sites used to examine temporal trends. Measures at baseline, 3, 6 months post-intervention Population: 9 NHs in North Carolina Dates: Jan 2001 – Dec 2002 (3 month recruitment/planning phase, 9 month intervention) Measures: Percent of all residents enrolled in hospice or receiving hospice palliative care consultation services, pain, treatments for pain, advance care planning discussions, orders limiting life-sustaining treatments, living wills, and health care powers of attorney |
Intervention: NH n=7∣Residents(n=345) 1) Identification of NH-based interdisciplinary Palliative Care Leadership Team who all attended 1-day conference covering hospice services, pain management, ACP, communication, quality improvement ; 2) Monthly on-site education and technical assistance on quality improvement, 3) 6 in-services for clinical staff (live & videotaped); 4) Monthly strategy meetings w/ investigators & hospice providers to design/implement stepwise organizational changes w/feedback on performance measures and action plans Control: NH=2∣ Residents(n=113) Usual Care |
Healthcare Use
|
| Hockley at al, 2010 Palliative Medicine (Midlothian, Scotland) | Structure and processes of care Ethical and legal aspects of care Physical aspects of care Care of the patient nearing the end of life |
Design: Two arm quasi-experimental trial (historical control group) Population: Deceased residents in 7 NHs Dates: Control: those who had died a year previous to the study (3/2006-2/2007) Intervention: those who had died during/following the Intervention (3/2007-unclear) Measures: Medical record evidence of documentation for advance care planning and do not attempt resuscitation orders, hospital admissions in the last 8 weeks of life, place of death and the use of the Liverpool Care Pathway |
Intervention (n=133) Gold Standards Framework for Care Homes and an adapted Liverpool Care Pathway for Care Homes implemented over an 18 month period with a model of high facilitation every 10–14 days; incorporated “key champions”, a nurse facilitator and key champion and NH staff training. Control (n=95) Retrospective cohort; usual care |
Healthcare Use
|
| Kinley et al, 2014 Palliative Medicine (UK) | Structure and process of care Ethical and legal aspects of care Care of the patient nearing the end of life |
Design: 3 arm parallel cluster RCT; stratified according to geographical location; randomized at NH level Population: Deceased residents in 38 NHs Dates: Jun 2008 – May 2011 preliminary stage (June 2008–August 2009); implementation (September 2009–May 2010); consolidation (June 2010–May 2011) Primary Measures: Place of death of resident Secondary Measures: Medical record documentation of advance care planning, having a cardiopulmonary resuscitation decision, and using end-of-life care plan documentation |
Intervention: Implementation of the GSF (Gold Standards Framework for Care Homes) High facilitation and Action Learning (NH n=12∣ Residents n=805); high facilitation and managers receiving action learning High Facilitation only (NH n=12∣ Residents n=703) high facilitation only Control: (NH n=14∣ Residents(n=936) Usual GSF care (received standard facilitation of the program available in their locality). |
Healthcare Use
|
| Strumpf et al Annals of Long-Term Care, 2004 (MD, USA) | Structure and processes of care Ethical and legal aspects of care Physical aspects of Care Psychological and psychosocial aspects of care |
Design: Two arm quasi-experimental trial Population: Residents at 6 community NHs; with terminal or end-stage disease, or those who had experienced significant functional decline, recent multiple hospitalizations, or major alterations in nutritional status Dates: Dec 1998-Dec 2001 Measures: Medical record documentation of physical and emotional symptoms, recording events at the time of death (eg, pain, hospital transfer, family present, etc), recording advance directives, surveying family satisfaction |
Intervention NH (n=4) PC Delivery Process training on advance care planning, pain and symptom management, and psychosocial concerns with ongoing guidance from a nurse with expertise in palliative care; Two of the four intervention homes also developed a dedicated interdisciplinary PC team with weekly meetings. Control NH (n=2) Usual Care |
Healthcare Use (intervention v control)
|
| Temkin-Greener et al, 2018 Medical Care (NY, USA) | Structure and processes of care Care at the end of life Physical aspects of care Psychological and psychosocial aspects of care |
Design: Two arm RCT with difference-in-difference analysis; randomized at the facility level after stratified by bed size Population: Deceased Medicare beneficiaries over age 65 at New York state NHs Dates: Pre intervention Oct 2012- Sep 2013; Intervention Oct 2013 – Apr 2016 Measures: Minimum data set documentation of place of death, number of hospitalizations within the last 90 days of stay, pain, depression |
Intervention: (NH n=14) Facility level intervention: Implemented PC teams and training-education program for staff, then 2-month period of active intervention phase with rounds w/ gero-palliative nurse practitioner, then 8-month passive phase with as needed coaching. Control: (NH n=11) Usual care Non-randomized control: (NH n=609) Usual care (used to assess placebo effect) |
Healthcare Use
|
| Teo et al, 2014 Palliative Medicine (Singapore) | Structure and processes of care Physical aspects of care Ethical and legal aspects of care |
Design: Quasi-experimental trial (matched historical control group) Population: Residents at 7 NHs at risk of dying in the next 6 months-1 year (identified through a clinical algorithm) Dates: Control group: deceased residents who were at the NH for at least 3 months Oct 2007-Sept 2009; Intervention group: Sept 2009-Feb 2011 Measures: hospitalization length of stay, nursing home LOS, emergency department visits, specialist outpatient clinic visits, costs of healthcare use, nursing home cost |
Intervention: (n=48) Project CARE: ACP (Respecting Choices framework) to 1) identify residents who choose comfort care; 2) palliative care staff training; 3) access to specialist physician and nurse visits Control: (n=197) Retrospective cohort; usual care |
Healthcare Use
|
Abbreviations: PC=palliative care; ACP = advance care planning; NH = nursing home; ED= emergency department
Results
We identified 1148 records through our database searches and an additional 19 articles by hand searches of reference lists. After reviewing the abstracts for all 1167 records, we identified 67 articles for full text review. Following review of the full text, we retained thirteen articles, each reporting results from unique trials, published between 2004 and 2018. Figure 1 details the screening and inclusion/exclusion process.
Figure 1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram:
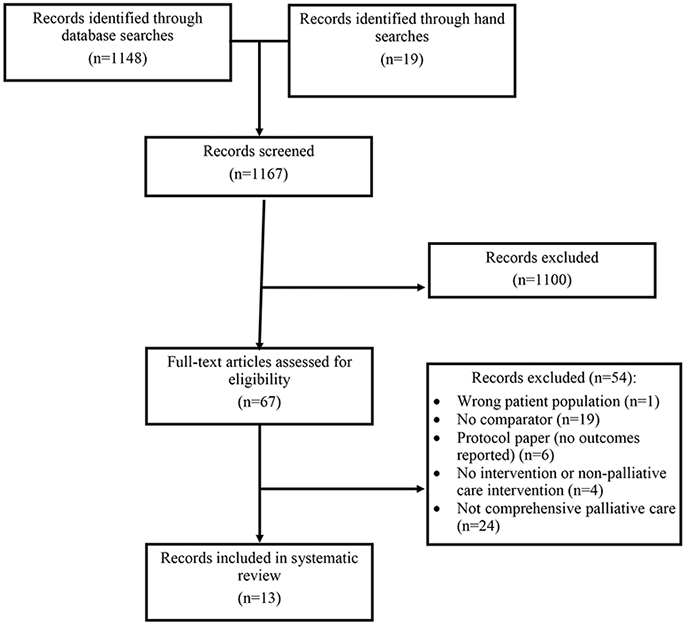
Results of Searches to Identify Clinical Trials of Palliative Care Interventions
Study Characteristics
About half of the studies were conducted in the United States (n=7).25-31 Three studies focused specifically on residents with dementia.27,32,33 Five studies used parallel group design with randomization at the facility (n=4)31-34 or resident level (n=1)26 and compared interventions to usual care26,31,32 or an active comparator.33,36 Seven studies used quasi-experimental designs in which intervention groups were compared to historical control groups (n=4)25,28,35,36 or usual care (n=3).29,30,37 One study used a randomized partial cross over design.27 Overall, nine of the 13 trials were judged as having high (n=4) or unclear (n=5) risk of bias (table 3).24
Table 3.
Bias Assessment
| Author, Year | Random sequence generation |
Allocation concealment |
Blinding of Outcomes assessment |
Incomplete outcomes data |
Selective reporting |
Overall Rating |
|---|---|---|---|---|---|---|
| Agar et al, 2017 | ● | ⊗ | ● | ● | ● | ● |
| Berkowitz et al, 2011 | n/a | n/a | n/a | ● | ⊝ | ⊝ |
| Boogard et al., 2018 | ● | ● | ⊗ | ⊗ | ● | ⊗ |
| Brännström et al, 2016 | n/a | n/a | n/a | ⊗ | ● | ⊝ |
| Casarett et al, 2005 | ● | ● | ⊗ | ● | ● | ● |
| Chapman and Toseland, 2007 | ⊝ | ● | ⊝ | ● | ● | ⊝ |
| Comart et al, 2012 | n/a | n/a | n/a | ● | ● | ⊝ |
| Hanson et al, 2005 | ⊝ | ⊗ | ⊗ | ● | ● | ⊗ |
| Hockley at al, 2010 | n/a | n/a | n/a | ● | ● | ⊝ |
| Kinley et al, 2014 | ● | ● | ● | ● | ● | ● |
| Strumpf et al 2004 | n/a | n/a | ⊝ | ● | ● | ⊝ |
| Temkin-Greener et al, 2018 | ● | ⊝ | ● | ● | ● | ● |
| Teo et al, 2014 | n/a | n/a | n/a | n/a | ● | ⊝ |
●= low; ⊗= high; ⊝= unclear
Palliative Care Intervention Characteristics
The multi-component interventions comprised a median of three of eight National Consensus Project domains (range 2-6). All interventions incorporated Structure and Process of Care and over half integrated Ethical and Legal Aspects of Care (n=9) and Physical Aspects of Care (n=9). Several interventions addressed Care at the End of Life (n=6) and Psychological and Psychiatric Aspects of Care (n=4). Two of the studies specifically described Social Aspects of Care.27,28 Only one intervention explicitly incorporated Spiritual, Religious, Existential Aspects of Care.28 None of the interventions addressed Cultural Aspects of Care.
Interventions focused on three major strategies: (1) advance care planning, (2) staff education (e.g., general concepts taught in a class or seminar) or training (e.g., mentoring palliative care skills in practice) and (3) integrating a palliative care team. Berkowitz et al. and Teo et al. integrated all three strategies into interventions.25,35
Staff education and/or training was the most common strategy used in the interventions. One trial used an audit and feedback strategy in which they regularly shared results of bereaved family care evaluations with staff.33 After discussing the reports, staff participated in quality improvement activities aimed at increasing evaluation scores. Several education/training programs also incorporated staff champions or facilitators to act as palliative care resources.29,34,37 Others implemented staff training in end-of-life care alongside facility based palliative care teams30,31 or consultative teams.28
Of six trials that implemented an interdisciplinary palliative care team; four clearly incorporated multiple disciplines (medicine, nursing, chaplains, social worker, and/or psychologist).25,27,28,30 The others utilized two disciplines: medicine and nursing35 or nursing and social work.31,38 Three interventions explicitly described creating palliative care teams from existing nursing home staff.27,30,31 Others implemented consultation services.25,28,35
Five studies integrated advance care planning into the palliative care intervention. Advance care planning strategies most often screened for individuals that would benefit from an advance care planning conversation. Four used illness prognosis and acute changes in clinical status to identify residents who would benefit from an advance care planning discussion25,36 35 32 One intervention implemented resident and surrogate interviews to identify residents with goals for care that focused on comfort.26
Outcomes
Healthcare use and symptoms were the most common outcomes evaluated in the trials and measured in various ways. Four trials described evidence of resident/surrogate advance care planning discussions and documentation. Three assessed family evaluation of care and only one trial each evaluated resident quality of life and costs/expenditures (Table 4).
Table 4.
Strategies, outcomes, and overall risk of bias
| Author, year | Strategies | Outcomes | Overall Risk of Bias |
||
|---|---|---|---|---|---|
| Advance Care Planning |
Staff training and education |
Integrating a palliative team |
|||
| Agar et al, 2017 | X | X | Healthcare Use Enhance NH palliative care (+) Symptoms Assessment/Management Process: pain/discomfort (+), restlessness (+), agitation (+), constipation (+), skin issues (+), resistive to care (+),respiratory issues (+) Resident/surrogate report: Comfort (−) Quality of life Resident/surrogate ratings at the end-of-life (−) Family Evaluation of Care Satisfaction with care (−) |
Low | |
| Berkowitz et al, 2011 | X | X | X | Healthcare Use Reduce potentially burdensome care (+) Enhance NH palliative care (+) |
Unclear |
| Boogard et al., 2018 | X | Symptoms Resident/surrogate report: Comfort (−) Dying symptoms (+), physical distress (−), emotional distress (−), wellbeing (−) Family Evaluation of Care Satisfaction * |
High | ||
| Brännström et al, 2016 | X | Symptoms Resident/surrogate report: shortness of breath (+), nausea (+), pain (−), tiredness (−), drowsiness (−), loss of appetite (−), anxiety (−), depression (−), wellbeing (−) |
Unclear | ||
| Casarett et al, 2005 | X | Healthcare Use Reduce potentially burdensome care* Enhance NH palliative care* Family Evaluation of Care End-of-life care ratings (+) |
Low | ||
| Chapman and Toseland, 2007 | X | Symptoms Resident/surrogate report: pain (−), depression (−),agitation (−), physically nonaggressive behaviors (+) |
Unclear | ||
| Comart et al, 2012 | X | X | Healthcare Use Reduce potentially burdensome care* Enhance NH palliative care (−) Symptoms Resident/surrogate report: depression (+), delirium (−), falls (−), pain (−), skin ulcers (−), shortness of breath (−), weight loss (−) |
Unclear | |
| Hanson et al, 2005 | X | Healthcare Use Enhance NH palliative care (+) Symptoms Assessment/Management Process: pain* Resident/surrogate report: pain (−) Advance Care Planning Documented discussions and orders (+) Advance Directives (−) |
High | ||
| Hockley at al, 2010 | X | X | Healthcare Use Reduce potentially burdensome care (+) Enhance NH palliative care (+) Advance Care Planning Documented discussions and orders (+) |
Unclear | |
| Kinley et al, 2014 | X | Healthcare Use Reduce potentially burdensome care (−) Enhance NH palliative care (+) Advance Care Planning Documented discussions and orders (−) |
Low | ||
| Strumpf et al, 2004 | X | X | Healthcare Use Enhance NH palliative care (+) Symptoms Assessment/Management Process: pain (+) Advance Care Planning Advance Directives (+) |
Unclear | |
| Temkin-Greener et al, 2018 | X | X | Healthcare Use Reduce potentially burdensome care (−) Symptoms Resident/surrogate report: pain (−), depression (−) |
Low | |
| Teo et al, 2014 | X | X | X | Healthcare Use Reduce potentially burdensome care* Costs/Expenditures Reduce costs (+) |
Unclear |
NH= Nursing Home
= mixed results
Changes in Clinical Practice and Healthcare Use
Six studies measured nursing home clinical practices aimed to enhance palliative care for residents. Seven studies examined the effects of palliative care interventions on potentially burdensome end-of-life healthcare use such as hospitalizations and emergency department visits.
In total, six studies reported positive changes in nursing home palliative care practices. Four found greater physician involvement in residents’ care during the last weeks of life30,32 and increased use of a pathway to assist staff in providing end-of-life treatments in nursing homes.34,36 Two studies found that interventions resulted in more discussions about hospice and higher hospice referral and enrollment rates.26,29
The effect of nursing home palliative care on residents’ acute care outcomes varied. Five studies found that palliative care interventions reduced resident emergency department visits,28 rehospitalizations,25,35 acute care admissions,26,36 days in acute care,26,35 and in-hospital death.36 In contrast, four interventions showed no significant effect on emergency department use in the last three months of life,35 rehospitalization,28,31 or in-hospital death.31,34
Effects of palliative care on nursing home death and hospice use were conflicting. Berkowitz et al. reported that residents receiving a palliative care consult intervention were more likely to die in the nursing home.25 Conversely, Casarett et al. found that an advance care planning intervention was not associated with greater likelihood of dying in the nursing home or death while receiving hospice services.26
Symptoms
Across eight studies, pain and symptom measures varied. To better synthesize the results, we categorized outcomes according to how they were measured: nursing home processes or resident/surrogate report. One study used process measures only (e.g., documented pain assessment and management),30 five studies evaluated resident or surrogate reported symptom severity,27-29,31,33,37 and two studies used both.29,32 Of the eight studies, three focused exclusively on residents with dementia.27,32,33 Most studies focused on measuring pain or discomfort, respiratory issues, depressive symptoms, and agitation.
Two studies found an improvement in pain and symptom assessment and management processes. After implementing staff education, Hanson et al. reported pre- to post-intervention increase in pain assessments (18% to 60%) and nonpharmacologic treatments (15% to 34%).29 Using education and training in conjunction with a facility-based palliative care team, Strumpf et al. reported intervention nursing homes had higher rates of documented symptoms and more residents with opioid pain management in the last weeks of life.30 One study that focused exclusively on residents with dementia found that staff education and training improved symptom management practices including documentation of pain, shortness of breath, agitation, nausea and constipation.32
In contrast to studies that documented improved pain and symptom clinical processes, evidence of enhanced patient symptom outcomes was uneven. Four interventions did not improve resident pain ratings.28,29,31,37 Effects of palliative care interventions on non-pain symptoms were reported in three trials with inconsistent results. Braanstrom et al. found residents in intervention nursing homes experienced less shortness of breath after integrating an end-of-life care pathway.37 In contrast, Comart et al. found no intervention effect on shortness of breath28 after implementing staff education and training and a palliative care team. Comart et al. found depression improved28 but trials using a palliative care team31 and an end-of-life care pathway37 did not report an improvement in depressive symptoms.
Of three studies that reported on surrogate-reported symptoms, none found that palliative care interventions decreased pain or improved comfort at the end of life for residents with dementia.27,33,34 Two trials that measured non-pain symptom outcomes had mixed results; residents assigned to a palliative care intervention showed a decrease in physically non-aggressive behaviors27 and improved dying symptoms;33 but no improvement in agitation or depression.
Advance Care Planning
There was mixed evidence among four studies examining the effect of palliative care interventions on advance care planning discussions and documentation. All the interventions incorporated ongoing staff support for palliative care with onsite education and expert assistance over a nine to 18-month period. Three quasi-experimental studies found increases in documented discussions of residents’ end-of-life treatment preferences, 29 “do not attempt resuscitation” orders,36 and presence of advance directives.30 In contrast, Kinley et al. found no significant difference in documented “do not attempt resuscitation” orders between intervention and control groups34 and Hanson et al. showed no change in documented use of advance directives pre- to post-intervention.29
Family Evaluation of Care
Three randomized clinical trials examined the effectiveness of interventions on bereaved family ratings of end-of-life care with varied outcomes. Casarett et al. reported that an advance care planning intervention designed to promote communication about hospice showed higher bereaved family ratings of end-of-life care, a difference that also was associated with greater numbers of days receiving hospice services.26 In contrast, two studies focusing on residents with dementia found no significant improvement in family members’ satisfaction with end-of-life care.33,32
Quality of Life
Only one study reported on the effects of a palliative care intervention on quality of life. In a trial of interactive, person-centered palliative care training and facilitated case conferencing, Agar et al found no intervention effects on quality of life in the 3 months prior to death for residents with advanced dementia and their family caregivers.32 However in additional analyses, better quality of life ratings were associated with nursing homes reporting higher staff knowledge and confidence providing palliative care.
Costs/Expenditures
Teo et al examined healthcare costs following staff education and training, a palliative care team intervention, and a clinical algorithm to identify residents at high risk of unmet palliative care needs.35 The investigators found that the mean cost per resident at three months prior to death was lower in the intervention group than that of a historical control group; this difference persisted into the final month of life.
Discussion
We examined the results of 13 clinical trials of multi-component palliative care interventions for persons receiving care in nursing homes. In six trials, interventions enhanced nursing home palliative care processes including increased use of care pathways, higher hospice referrals, and better documentation of pain and symptom assessment and management. However, in most trials there was mixed or insufficient evidence about the effect of palliative care interventions on reducing potentially burdensome care, resident/surrogate symptom ratings, advance care planning discussions and documentation, and improving family members’ evaluation of care. Our findings suggest there is limited evidence that palliative care interventions improve nursing home end-of-life care outcomes. In addition, the high or unclear risk of bias among the majority of the clinical trials requires caution when interpreting the results.
Of the three studies that included only residents with dementia, none found that palliative care interventions improved surrogate-reported resident pain. Because persons with dementia have limited ability to self-report symptoms, researchers often rely on surrogate report and medical record data, which may be inaccurate. Previous research demonstrates that pain in persons with dementia is frequently unrecognized and under-reported in long-term care settings.39,40 Additionally, small sample sizes in the included studies may have prevented researchers from achieving significant results.
Eleven of the studies in our review used an intervention that included palliative care education/training; four trials used this approach alone and had mixed or no effect on resident symptoms. Clinicians and researchers alike suggest that education is essential for change in clinical practice however a recent literature review found that existing palliative care education/training resources may be inadequate.41 Our findings demonstrate a movement toward interventions that integrate education and training with other approaches to improve palliative care delivery. Of the seven interventions that combined education with at least one other palliative care strategy, four enhanced nursing home palliative care practices.25,30,32,36 This is consistent with prior work showing residents in nursing homes with higher palliative care knowledge and practice scores experience better care at the end-of-life.43
The design of palliative care teams differed across six studies, with some creating an internal team from the preexisting facility staff and others creating a consultative palliative care team; neither model demonstrated consistently positive results. For example, three studies in our review that created an internal team and provided ongoing access to a palliative care expert showed an improvement in symptom management processes30 but not in residents’ pain and depression.27,31 We believe the existing nursing home interdisciplinary team is a strength that can be built upon for palliative care interventions. However, Norton et al. cite many challenges with this approach including the need for administrative support, financial resources, staff and leadership turnover, and competing priorities; all may interrupt or delay the uptake of palliative care interventions.38
Three trials that used a palliative care specialty consultation team demonstrated a reduction in potentially burdensome care including emergency department visits28 and hospital transfers.25,35 These findings are complementary to previous work by Miller et al. who showed that integrating a palliative care consultant into routine care reduces potentially burdensome setting transitions.15,19 It may be that using an “outside” resource captures the specialty training of consultants to address the unmet needs of seriously ill residents. However, current palliative care workforce projections suggest that palliative care needs cannot be met by specialists alone.43
Based on our findings, we recommend that future research should be multifaceted and support nursing home care providers in delivering primary palliative care, allow for ongoing collaboration with experts, and identify appropriate residents for services. This is consistent with Hall et al. 2010 systematic review that revealed potentially promising results for interventions that assessed residents’ suitability for palliative care and focused on developing palliative care expertise in nursing homes.17 In addition, program expenses and staffing should be monitored to address facilities’ concerns about costs and resource utilization.
The evidence included in this review is limited by the complexity of the palliative care interventions. A lack of effect on outcomes may reflect intervention implementation failure rather than ineffectiveness.44 A systematic process evaluation during and after a trial may help to identify implementation challenges.45 Further, it is difficult to assess what parts of each intervention were most effective and what parts did not provide benefit. Future work should focus on examining components of palliative care interventions that residents, family, and nursing home staff value, especially those that improve outcomes.
Our review has a number of strengths, including a comprehensive search for palliative care clinical trials that integrate multiple domains recommended by national guidelines and reporting on resident and family-oriented outcomes. However, there are several limitations. First, we noted great heterogeneity across trial designs that limited our synthesis of study outcomes. For example, quasi-experimental designs that compare intervention groups to historical control groups and non-randomized pre-post studies are known to be confounded by temporal trends and the inability to control for variability among the groups being compared. Similar methodologies across studies would have enabled a deeper examination of inconsistent or mixed outcomes as few clinical trials of palliative care interventions in nursing homes exist. Second, our selection criteria may have resulted in the exclusion of some effective interventions because we did not include single component interventions that incorporated only one palliative care domain. Additionally, we acknowledge that the projects supported by the Centers for Medicare and Medicaid Initiative to Reduce Avoidable Hospitalizations among Nursing Facility Residents included palliative care componenects however they were not explicitly framed as palliative care interventions so were not included in our review.46 Lastly, while we attempted to use a practical risk of bias assessment tool, it was subjective and may not be sensitive to the complexities of all the clinical trial designs in our study.
Conclusion
In this systematic review, we found that the evidence base for multi-component nursing home palliative care interventions is limited. We identified a small group of diverse clinical trials that enhanced nursing home palliative care and improved symptom assessment and management processes. Effects on other outcomes such as reducing potentially burdensome care, resident /surrogate reported symptoms, advance care planning discussions and documentation, and family members’ evaluation of care is lacking and warrants further study. There is a critical gap in evidence for quality of life and costs outcomes. Future research should focus on developing nursing home palliative care interventions that contain components important to staff, providers, residents and their family caregivers, provide access to experts, and identify residents who would most benefit from services. In addition, palliative care interventions are highly complex and outcome evaluations should explore how an intervention is implemented so that if successful, it can be tailored to nursing home environments.44
Supplementary Material
Funding sources:
Research reported in this publication was supported by: National Institute of Nursing Research of the National Institutes of Health under Award Number K23NR017663. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health; Rita & Alex Hillman Foundation Emergent Innovation Program; Veterans Health Administration Postdoctoral Nurse Fellowship Program; University of Pennsylvania Center for Undergraduate Research Mentorship Program; and the University of Pennsylvania AD Center P30 Grant # AG 10124.
Footnotes
Conflicts of Interest Statement: There are no conflicts of interest.
References
- 1.Ferrell BR, Twaddle ML, Melnick A, Meier DE. National Consensus Project Clinical Practice Guidelines for Quality Palliative Care Guidelines, 4th Edition. J Palliat Med. 2018. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 2.Cassel JB, Kerr K, Pantilat S, Smith TJ. Palliative care consultation and hospital length of stay. J Palliat Med. 2010;13:761–767. [DOI] [PubMed] [Google Scholar]
- 3.Chand P, Gabriel T, Wallace CL, Nelson CM. Inpatient palliative care consultation: Describing patient satisfaction. Perm J. 2013;17:53–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.May P, Normand C, Morrison RS. Economic impact of hospital inpatient palliative care consultation: Review of current evidence and directions for future research. J Palliat Med. 2014;17:1054–1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Singer AE, Goebel JR, Kim YS, et al. Populations and interventions for palliative and end-of-life care: A systematic review. J Palliat Med. 2016;19:995–1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kavalieratos D, Corbelli J, Zhang D, et al. Association between palliative care and patient and caregiver outcomes: A systematic review and meta-analysis. JAMA. 2016;316:2104–2114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Teno JM, Gozalo PL, Bynum JP, et al. Change in end-of-life care for Medicare beneficiaries: site of death, place of care, and health care transitions in 2000, 2005, and 2009. JAMA. 2013;309:470–477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hunnicutt JN, Ulbricht CM, Tjia J, Lapane KL. Pain and pharmacologic pain management in long-stay nursing home residents. Pain. 2017;158:1091–1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Greenwood N, Menzies-Gow E, Nilsson D, Aubrey D, Emery CL, Richardson A. Experiences of older people dying in nursing homes: A narrative systematic review of qualitative studies. BMJ Open. 2018;8:e021285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Carpenter JG, Berry PH, Ersek M. Nursing home care trajectories for older adults following in-hospital palliative care consultation. Geriatric Nurs. 2017;38:531–536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aragon K, Covinsky K, Miao Y, Boscardin WJ, Flint L, Smith AK. Use of the medicare posthospitalization skilled nursing bnefit in the last 6 months of life. Arch Intern Med. 2012;172:1573–1579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Temkin-Greener H, Lee T, Caprio T, Cai S. Rehabilitation Therapy for nursing home residents at the end-of-life. J Am Med Dir Assoc. 2019;20:476–480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Carlson MD, Lim B, Meier DE. Strategies and innovative models for delivering palliative care in nursing homes. J Am Med Dir Assoc. 2011;12:91–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ersek M S J., Stevenson D. Palliative care in nursing homes. In: Kelley AM Meier DE, eds. Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care Reform. New York: Springer; 2014. [Google Scholar]
- 15.Miller SC, Lima JC, Intrator O, Martin E, Bull J, Hanson LC. Palliative care consultations in nursing homes and reductions in acute care use and potentially burdensome end-of-life transitions. J Am Geriatr Soc. 2016;64:2280–2287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Froggatt KA, Wilson D, Justice C, et al. End-of-life care in long-term care settings for older people: a literature review. Int J Older People Nursing. 2006;1:45–50. [DOI] [PubMed] [Google Scholar]
- 17.Hall S, Kolliakou A, Petkova H, Froggatt K, Higginson IJ. Interventions for improving palliative care for older people living in nursing care homes. Cochrane Database Systc Rev. 2011:CD007132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Miller SC, Lima JC, Intrator O, Martin E, Bull J, Hanson LC. Specialty palliative care consultations for nursing home residents with dementia. J Pain Symptom Manage. 2017;54:9–16.e15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Miller SC, Dahal R, Lima JC, et al. Palliative care consultations in nursing homes and end-of-life hospitalizations. J Pain Symptom Manage. 2016;52:878–883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Temkin-Greener H, Ladwig S, Caprio T, et al. Developing palliative care practice guidelines and standards for nursing home-based palliative care teams: A Delphi study. J Am Med Dir Assoc. 2015;16:86.e1–7. [DOI] [PubMed] [Google Scholar]
- 21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009;6:e1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7:16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fulton JJ, LeBlanc TW, Cutson TM, et al. Integrated outpatient palliative care for patients with advanced cancer: A systematic review and meta-analysis. Palliat Med. 2019;33:123–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Berkowitz RE, Jones RN, Rieder R, et al. Improving disposition outcomes for patients in a geriatric skilled nursing facility. J Am Geriatr Soc. 2011;59:1130–1136. [DOI] [PubMed] [Google Scholar]
- 26.Casarett D, Karlawish J, Morales K, Crowley R, Mirsch T, Asch DA. Improving the use of hospice services in nursing homes: a randomized controlled trial. JAMA. 2005;294:211–217. [DOI] [PubMed] [Google Scholar]
- 27.Chapman DG, Toseland RW. Effectiveness of advanced illness care teams for nursing home residents with dementia. Soc Work. 2007;52:321–329. [DOI] [PubMed] [Google Scholar]
- 28.Comart J, Mahler A, Schreiber R, Rockett C, Jones RN, Morris JN. Palliative care for long-term care residents: Effect on clinical outcomes. Gerontologist. 2013;53:874–880. [DOI] [PubMed] [Google Scholar]
- 29.Hanson LC, Reynolds KS, Henderson M, Pickard CG. A quality improvement intervention to increase palliative care in nursing homes. J Palliat Med. 2005;8:576–584. [DOI] [PubMed] [Google Scholar]
- 30.Strumpf N, Tuch H, Stillman D, Parrish P, Morrison N. Implementing Palliative Care in the Nursing Home. Annals of Long Term Care. 2004;12(11). [Google Scholar]
- 31.Temkin-Greener H, Mukamel DB, Ladd H, et al. Impact of nursing home palliative care teams on end-of-life outcomes: A randomized controlled trial. Med Care. 2018;56:11–18. [DOI] [PubMed] [Google Scholar]
- 32.Agar M, Luckett T, Luscombe G, et al. Effects of facilitated family case conferencing for advanced dementia: A cluster randomised clinical trial. PloS One. 2017;12:e0181020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Boogaard J, Vet H, Soest-Poortvliet M, Anema J, Achterberg W, Steen J. Effects of two feedback interventions on end-of-life outcomes in nursing home residents with dementia: A cluster-randomized controlled three-armed trial. Palliat Med. 2018;32:693–702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kinley J, Stone L, Dewey M, et al. The effect of using high facilitation when implementing the Gold Standards Framework in Care Homes programme: A cluster randomised controlled trial. Palliat Med. 2014;28:1099–1109. [DOI] [PubMed] [Google Scholar]
- 35.Teo WS, Raj AG, Tan WS, Ng CW, Heng BH, Leong IY. Economic impact analysis of an end-of-life programme for nursing home residents. Palliat Med. 2014;28:430–437. [DOI] [PubMed] [Google Scholar]
- 36.Hockley J, Watson J, Oxenham D, Murray SA. The integrated implementation of two end-of-life care tools in nursing care homes in the UK: an in-depth evaluation. Palliat Med. 2010;24:828–838. [DOI] [PubMed] [Google Scholar]
- 37.Brännström M, Fürst CJ, Tishelman C, Petzold M, Lindqvist O. Effectiveness of the Liverpool care pathway for the dying in residential care homes: An exploratory, controlled before-and-after study. Palliat Med. 2016;30:54–63. [DOI] [PubMed] [Google Scholar]
- 38.Norton SA, Ladwig S, Caprio TV, Quill TE, Temkin-Greener H. Staff Experiences Forming and Sustaining Palliative Care Teams in Nursing Homes. Gerontologist. 2018;58:e218–e225. [DOI] [PubMed] [Google Scholar]
- 39.Closs SJ, Barr B, Briggs M. Cognitive status and analgesic provision in nursing home residents. Br J Gen Pract. 2004;54:919–921. [PMC free article] [PubMed] [Google Scholar]
- 40.Reynolds KS, Hanson LC, DeVellis RF, Henderson M, Steinhauser KE. Disparities in pain management between cognitively intact and cognitively impaired nursing home residents. J Pain Symptom Manage. 2008;35:388–396. [DOI] [PubMed] [Google Scholar]
- 41.Aldridge MD, Hasselaar J, Garralda E, et al. Education, implementation, and policy barriers to greater integration of palliative care: A literature review. Palliat Med. 2016;30:224–239. [DOI] [PubMed] [Google Scholar]
- 42.Miller SC, Lima JC, Thompson SA. End-of-life care in nursing homes with greater versus less palliative care knowledge and practice. J Palliat Med. 2015;18:527–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kamal AH, Bull JH, Swetz KM, Wolf SP, Shanafelt TD, Myers ER. Future of the Palliative care workforce: Preview to an impending crisis. Am J Med. 2017;130:113–114. [DOI] [PubMed] [Google Scholar]
- 44.Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Stetler CB, Legro MW, Wallace CM, et al. The role of formative evaluation in implementation research and the QUERI experience. J Gen Intern Med. 2006;21 Suppl 2:S1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ingber MJ, Feng Z, Khatutsky G, et al. Initiative To reduce avoidable hospitalizations among nursing facility residents shows promising results. Health Aff (Millwood). 2017;36:441–450. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.