
Fig. 1.
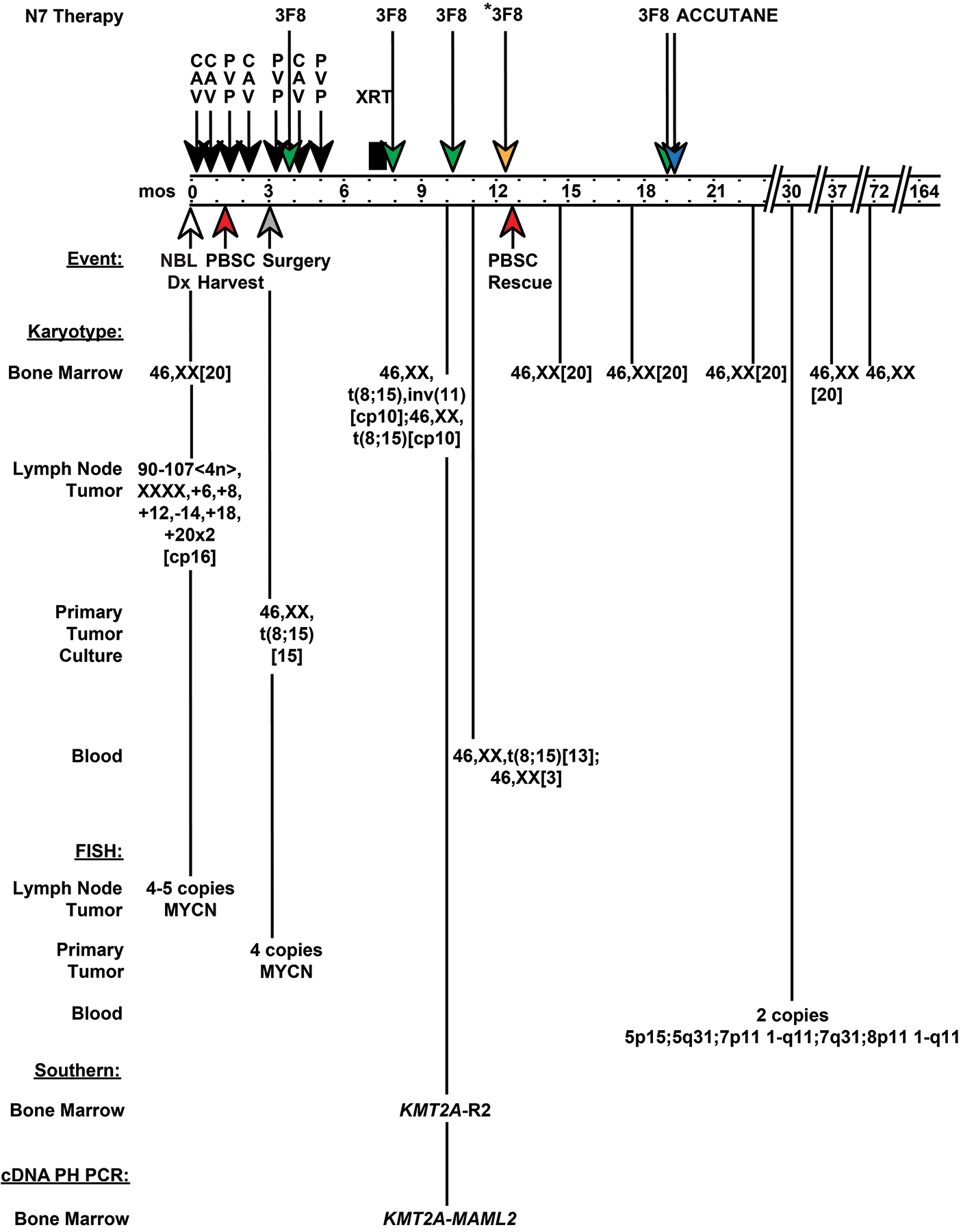
Treatment, clinical course, and timeline of cytogenetic and molecular findings in patient with Stage 4N neuroblastoma enrolled to MSK-N7 trial. Schematic shows when inv(11)(q21q23) resulting in KMT2A-MAML2 rearrangement occurred and disappeared relative to treatment. The treatment included 7 dose-intensive cycles of induction chemotherapy [4 cycles of cyclophosphamide, adriamycin, and vincristine (CAV); 3 cycles of cisplatin and etoposide (PVP)], 3 cycles of cold anti-GD2 monoclonal antibodies (3F8) and local radiation before myeloablation with radiolabeled 3F8 monoclonal antibodies (3F8*) and autologous PBSC rescue. Autologous PBSCs were harvested after cycle 2, which was CAV. Following PBSC rescue, a final cycle of adjuvant 3F8 began, but accutane was substituted for 3F8 due to allergic reaction. At neuroblastoma diagnosis (time 0 months), note hyper-tetraploid karyotype of lymph node tumor tissue, and normal marrow karyotype. At surgical resection (time 3 months) the primary tumor cells contained 4 copies of MYCN by FISH, whereas the karyotype after culture was 46,XX,t(8;15)(p21;q26)[15], suggesting contaminating blood cells in the tumor. After all 7 chemotherapy cycles (time 10 months), all cells in the marrow had a pseudodiploid karyotype with t(8;15)(p21;q26), and half also had inv(11)(q21q23). At time 11 months the peripheral blood karyotype was 46,XX,t(8;15)(p21;q26)[13];46,XX[3]. All subsequent marrow karyotypes were normal. FISH studies and results are shown. Abbreviations: mos, months; CAV, cyclophosphamide 4200 mg/m2, adriamycin 75 mg/m2, vincristine 1.5 mg/m2; PVP, cisplatin 200 mg/m2, etoposide 600 mg/m2; 3F8*, radiolabeled anti-GD2 monoclonal antibody; 3F8, cold anti-GD2 monoclonal antibody; NBL, neuroblastoma; XRT, local radiation therapy to neck and chest and to abdomen and hip; PBSC, peripheral blood stem cell; KMT2A-R2, two rearranged KMT2A bcr fragments; cDNA PH PCR, cDNA panhandle PCR.