

A 57-year-old male with previous myocardiopathy, polyneuropathy, bilateral cataract, and autonomic dysfunction had a family history of Familial Amyloid Polyneuropathy (FAP)1,2. When he was 55 years old, he underwent a genetic testing, which detected a deleterious heterozygous mutation c.325G>A, Glu109Lys, on exon 3 of the Transthyretin gene, for the diagnosis of FAP3. He was treated with Vyndaqel® (tafamidis meglumine) and amiodarone. He developed reduction of visual acuity in the right eye and floaters. Physical examination found that he had visual acuity of 20/40 (OD) and 20/25 (OS), with altered campimetry only in OD. The neuro-ophthalmological evaluation is provided in Figures 1-4. Laboratory testing excluded other hematological abnormalities. The final diagnosis was retinal amyloid angiopathy secondary to FAP. Ocular manifestations in FAP are rare; nevertheless, neurologists should investigate visual symptoms in patients with FAP. Retinal amyloid angiopathy is even rarer, but is a sight-threatening complication. Neurologists should assess the visual acuity, the intraocular pressure, vessel tortuosity, collaterals, or scalloped pupils, promptly indicating an ophthalmological evaluation4. Recent progress in the neuro-ophthalmological evaluation indicated that retinal amyloid angiopathy is more frequent than previously reported4. Therefore, neurologists should be aware of this complication in patients with FAP, especially in those presenting vitreous amyloidosis or longer duration of the disease5.
Figure 1. A: Retinography showing vitreous opacity in temporal periphery in OD. It was normal in the OS. B: FAF images show hyper autofluorescence whitish deposit above the optic disk and in the superior and inferior vascular arcades of the OD. The FAF was normal in the OS. C: Fluorescein angiography: a -whitish deposit in the nasal superior retina; b -superior peripheral vascular tortuosity, collateral secondary to arterial occlusion; c -detail of figure b; d -whitish deposit in the superior and inferior (hyper autofluorescence) temporal vascular arcades; e -arterial retinal occlusion in the inferior periphery in the OS; and f -detail of figure e.
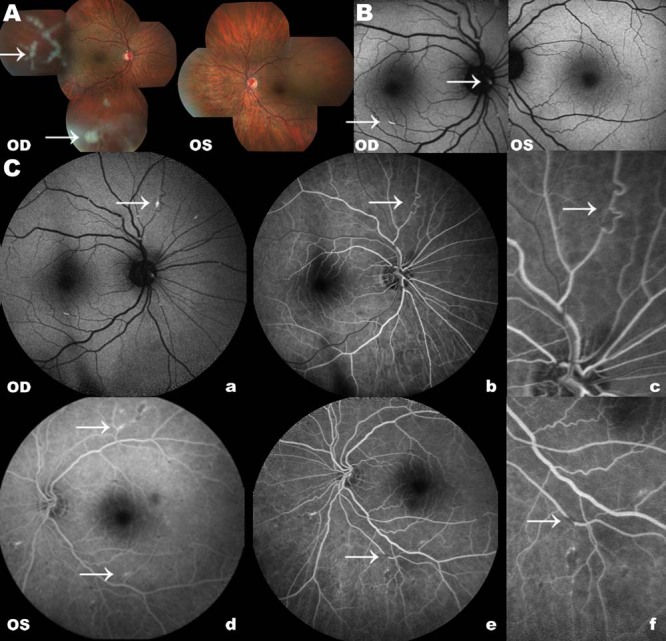
OD: right eye; OS: left eye; FAF: fundus autofluorescence; arrow: alterations.
References
- Adams D, Suhr OB, Hund E, Obici L, Tournev I, Campistol JM, et al. First European consensus for diagnosis, management, and treatment of transthyretin familial amyloid polyneuropathy. Curr Opin Neurol. 2016;29(1) 1:S14–S26. doi: 10.1097/WCO.0000000000000289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plante-Bordeneuve V. Transthyretin familial amyloid polyneuropathy: an update. J Neurol. 2018;265(4):976–983. doi: 10.1007/s00415-017-8708-4. [DOI] [PubMed] [Google Scholar]
- Nakamura M, Asl KH, Benson MD. A novel variant of transthyretin (Glu89Lys) associated with familial amyloidotic polyneuropathy. Amyloid. 2000;7(1):46–50. doi: 10.3109/13506120009146824. [DOI] [PubMed] [Google Scholar]
- Latasiewicz M, Sala-Puigdollers A, Gonzalez-Ventosa A, Milla E, Civera AA. Multimodal retinal imaging of familial amyloid polyneuropathy. Ophthalmic Genet. 2019;40(5):407–420. doi: 10.1080/13816810.2019.1666413. [DOI] [PubMed] [Google Scholar]
- Beirão NM, Miranda V, Beirão I, Costa PP, Torres P. The use of intravitreal ranibizumab to treat neovascular glaucoma because of retinal amyloid angiopathy in familial amyloidosis transthyretin v30m related. Retin Cases Brief Rep. 2013;7(1):114–116. doi: 10.1097/ICB.0b013e3182681259. [DOI] [PubMed] [Google Scholar]