

Abstract
Background
Carbapenem-resistant gram-negative bacteria (CR-GNB) are becoming increasingly important bacterial pathogens in critically ill patients. Several clinicians use Intravenous colistin sulfate to treat infections due to CR-GNB, although the clinical data is limited. The aim of our retrospective observational study was to evaluate the effectiveness and nephrotoxicity of intravenous colistin sulfate in the treatment of CR-GNB infections.
Methods
Fifty critically ill intensive care patients with infections due to CR-GNB were retrospectively enrolled between January 2020 and December 2021 in the Zhejiang Provincial People’s Hospital. Favorable clinical response rate, bacterial clearance rate, nephrotoxicity, and 28-day mortality were evaluated.
Results
The overall favorable clinical response rate was 58%, the bacterial clearance rate was 40%, and the 28-day all-cause mortality was 44%. Temperature, neutrophil count, C-reaction protein (CRP), procalcitonin (PCT), creatinine (Cr), and lactate levels were also significantly decreased (P<0.05). The major adverse reaction is nephrotoxicity, and renal function was evaluated on the day before and after treatment with colistin sulfate. Possible nephrotoxicity was observed in three patients (6%). Backward logistic regression was conducted to determine risk factors for the nephrotoxicity of colistin sulfate, the result showed there were no significant differences in the duration and dose of colistin sulfate.
Conclusions
Our results provide evidence for the positive clinical efficacy and safety of colistin sulfate. Appropriate use of colistin sulfate may be viable and safe in the treatment of severe infections caused by CR-GNB.
Keywords: Carbapenem-resistant gram-negative organism, colistin sulfate, infection, renal function
Introduction
Sepsis is potentially a life-threatening condition, and it is characterized by bacterial infection and resultant organ dysfunction. The surviving sepsis campaign bundles emphasise the early administration of broad spectrum antibiotics (1). However, in recent years, the problem of carbapenem-resistant organisms has become increasingly prevalent, which can delay targeted treatment and increase mortality (2). The resistance rate of carbapenem-resistant gram-negative bacteria (CR-GNB) is increasing over time. According to data from the Chain Antimicrobial Resistance Surveillance System (CARSS), the resistance rate of carbapenem-resistant Klebsiella pneumoniae (CR-KP) increased from 4.9% to 10.9% from 2013 to 2020. The resistance rates of carbapenem-resistant Acinetobacter baumannii and Enterobacteriaceae were 53.7% and 18.3%, respectively, in 2020 (3).
Polymyxins have been revived as a last-line treatment for infections caused by multidrug-resistant (MDR), extensively drug-resistant (XDR), and pandrug-resistant (PDR) bacteria (4,5). Polymyxins are a class of antibiotic drugs targeting gram-negative bacterial infections, which are used to treat systemic infections caused by susceptible strains of multidrug-resistant organisms such as Pseudomonas aeruginosa, Acinetobacter baumannii, and Enterobacteriaceae. Polymyxins act on the outer membrane of gram-negative bacteria by disrupting the stabilization of phospholipids and lipopolysaccharides. Polymyxins can also neutralize the endotoxic effects of pathogens, thus reducing their effect on circulation (6-8).
Polymyxin B (PMB) and polymyxin E (colistin) are the two drugs most commonly used in clinical practice in this class of antibiotics (9,10). Two forms of colistin are commercially available: colistin sulfate and colistimethate sodium (CMS), also called sodium colistin methanesulfonate.
PMB has direct action, is less dependent on renal function, and is widely used in clinical treatment. Nephrotoxicity is the most commonly reported adverse event for intravenous polymyxins, with an incidence as high as 10–60%. CMS has higher nephrotoxicity than PMB and may induce acute kidney injury at a rate of up to 53%.
However, while PMB has lower nephrotoxicity than CMS (11,12), several studies have reported that PMB induces skin hyperpigmentation (13-15). There are no published reports of this side-effect with CMS. Because of these adverse effects, the clinical uses for PMB and CMS have been limited (16).
In most countries, CMS is the only form of polymyxin E. Colistin sulfate, another form of polymyxin E, has been widely used in China. In 2018, the colistin sulfate was approved by the Chinese National Medical Products Administration (NMPA) for clinical use. Thus, the clinical efficacy and side effects have not been reported and the clinical data are limited. Several studies showed that the efficacy of colistin sulfate was similar to the efficacy of PMB. And no patient developed colistin sulfate-related nephrotoxicity (17-19). But the clinical data on colistin sulfate are still limited. There is lack of data on efficacy, adverse events especially the nephrotoxicity for colistin sulfate in the treatment of CR-GNB infections. Thus, we conducted this retrospective study to assess the efficacy and safety of colistin sulfate in CR-GNB infections in Chinese. We present the following article in accordance with the STROBE reporting checklist (available at https://atm.amegroups.com/article/view/10.21037/atm-22-4959/rc).
Methods
Study design and patient selection
This retrospective cohort study was conducted at Zhejiang Provincial People’s Hospital, China, during January 1, 2020 to December 31, 2021. Patients were included who had a positive culture of CR-GNB or a highly suspected CR-GNB infection and hospitalized in the intensive care unit (ICU), and all patients received intravenous colistin sulfate more than 48 h. The CR-GNB included Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Escherichia coli, Stenotrophomonas maltophilia, and Enterobacter cloacae. Patients were excluded if they were <18 years old or died within 48h after being treated with intravenous colistin sulfate. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Ethics Committee of Zhejiang Provincial People’s Hospital (No. QT2022190). And individual consent for this retrospective analysis was waived.
Definition and data collection
All microorganisms were isolated by conventional methods. Bacterial identification and drug sensitivity tests were performed using a Vitek® 2 automated system (Biomerieux, France).
All patients in this study received intravenous colistin sulfate (Colistin Sulfate for Injection; Shanghai SPH New Asia Pharmaceutical Co. Ltd., Shanghai, China) for more than 48h at a dose of 1.0–1.5 million IU per day.
The following variables were recorded: the clinical characteristics of each patient, including gender, age, body mass index, admitting diagnosis, admission and discharge date, the date of admission and discharge from ICU, and the need for mechanical ventilation and continuous renal replacement therapy (CRRT). The following clinical and laboratory parameters were compared before and after therapy: temperature, white blood cell (WBC) count, C-reactive protein (CRP), procalcitonin (PCT), platelet count (PLT), Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and the Sequential Organ Failure Assessment (SOFA) score.
The major adverse event was nephrotoxicity. Renal function was evaluated on the day before and after treatment with colistin sulfate. Increased creatinine (Cr) was calculated by subtracting the creatinine level before the commencement of colistin sulfate treatment from the creatinine level after treatment. The presence of nephrotoxicity was determined according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria (20).
A favorable clinical response was defined as recovery from symptoms and signs at the conclusion of colistin sulfate treatment. An unfavorable clinical response was defined as deterioration or persistence of symptoms and signs during treatment. During the treatment, microbiological cultures were repeatedly evaluated. Bacterial eradication was defined as a quantity reduction or clearance of causative pathogens according to the microbiological culture results.
The primary outcome of this research was defined as 28-day mortality after ICU admission. The secondary outcomes were the occurrence of adverse events during colistin sulfate therapy, including nephrotoxicity as the primary adverse event and identified using the KDIGO criteria.
Statistical analysis
SPSS25.0 software was used for statistical analyses. Data are presented as n (%), mean ± SD or median (interquartile range). The Student’s t-test was conducted for continuous variables between groups. The χ2 or Fisher’s exact test was performed for categorical variables. Logistic regression models were built after univariate analysis. Variables that were significantly associated with outcome and nephrotoxicity in the univariate analyses were entered in the multivariate backward logistic regression models. Kaplan-Meier curves were conducted to demonstrate the survival probability and were compared using the log-rank test between groups. A two-tailed P value <0.05 was considered statistically significant.
Results
Clinical characteristics
The clinical characteristics of patients are summarized in Table 1.
Table 1. Patient characteristics.
| Characteristics | Patients receiving colistin sulfate |
|---|---|
| Male | 40 (80.0) |
| Weight (kg) | 70 (56.8–86.5) |
| T (℃) | 38.3±1.0 |
| MV | 42 (84.0) |
| CRRT | 14 (28.0) |
| Septic shock | 29 (48.0) |
| SOFA score | 10.9±4.3 |
| APACHE II score | 24.3±5.3 |
| CKD | 1 (2.0) |
| Prior hospitalization | 12 (5–17.3) |
| ICU stay (days) | 30 (19.3–47.3) |
| Total length of stay (days) | 37 (25–67.3) |
| 28-day mortality | 22 (44.0) |
| Bacteria eradication | 20 (40.0) |
| Favorable clinical response | 29 (58.0) |
| Laboratory parameters (before CS treatment) | |
| WBC (×109/L) | 11.56 (7.9–18.0) |
| N (×109/L) | 9.6 (6.7–16.5) |
| CRP (mg/L) | 113.2 (74.1–165.5) |
| PCT (ng/mL) | 2.21 (0.9–6.0) |
| PLT (×109/L) | 91 (60.1–188.3) |
| TBIL (μmol/L) | 27.25 (19.4–91.8) |
| Cr (μmol/L) | 91.4 (66.8–121.8) |
| Alb (g/L) | 31.05 (28.3–34.2) |
| Lac (mmol/L) | 26 (1.7–3.6) |
| Bacterial | N=70 |
| AB | 23 (32.9) |
| KP | 20 (28.5) |
| PA | 12 (17.1) |
| Fungus | 3 (4.3) |
| Other | 12 (17.0) |
| Infection sites | N=64 |
| POSI | 4 (6.3) |
| Pulmonary infection | 43 (67.2) |
| Intraperitoneal infection | 4 (6.3) |
| Incision infection | 2 (3.1) |
| Central venous catheter | 1 (1.6) |
| Other | 10 (15.6) |
| Duration of CS treatment days | 11 (7–16.3) |
| Nephrotoxicity | |
| Baseline | 22 (44.0) |
| After treatment | 12 (24.0) |
Data are shown as mean ± SD, median (IQR) or n (%). IQR, interquartile range; SD, standard deviation; T, temperature; MV, mechanical ventilation; CRRT, continuous renal replacement therapy; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; CKD, chronic kidney disease; ICU, intensive care unit; CS, colistin sulfate; WBC, white blood cell; N, neutrophils; CRP, C-reaction protein; PCT, procalcitonin; PLT, platelet; TBIL, total bilirubin; Cr, creatinine; Alb, albumin; Lac, lactate; AB, Acinetobacter baumannii; KP, Klebsiella pneumoniae; PA, Pseudomonas aeruginosa; POSI, postoperative surgical infection.
The study screened 62 patients who fulfilled the inclusion criteria. Twelve patients were excluded as they were <18 years or died within 48 h after being treated with intravenous colistin sulfate (Figure 1). A total of 50 patients were enrolled who were admitted between January 2020 and December 2021. All 50 patients with CR-GNB infections received empirical antimicrobial therapy in ICU before colistin sulfate therapy, and a 28-day follow-up was required for every patient included in the study.
Figure 1.
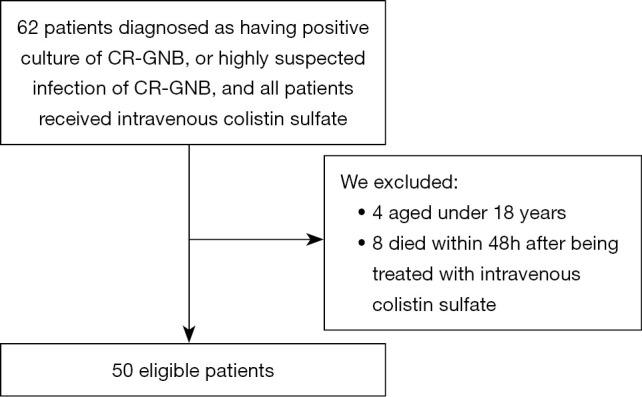
Flow-chart of the patient selection process. CR-GNB, carbapenem-resistant gram-negative bacteria.
The mean age of all patients was 70 years (range, 56.8–86.5 years), and there were 40 (80%) male patients. The average APACHE II score was 24.3±5.3, and the average SOFA score was 10.9±4.3. The rate of mechanical ventilation was 84% (42 patients).
Twenty-nine (58%) and 20 (40%) patients had favorable clinical responses and confirmed bacterial eradication, respectively.
Twenty-two patients died within 28 days. The 28-day all-cause mortality was 44%. About 56% of deaths occurred within 28 days of colistin sulfate treatment, as shown in the Kaplan-Meier survival curve (Figure 2).
Figure 2.
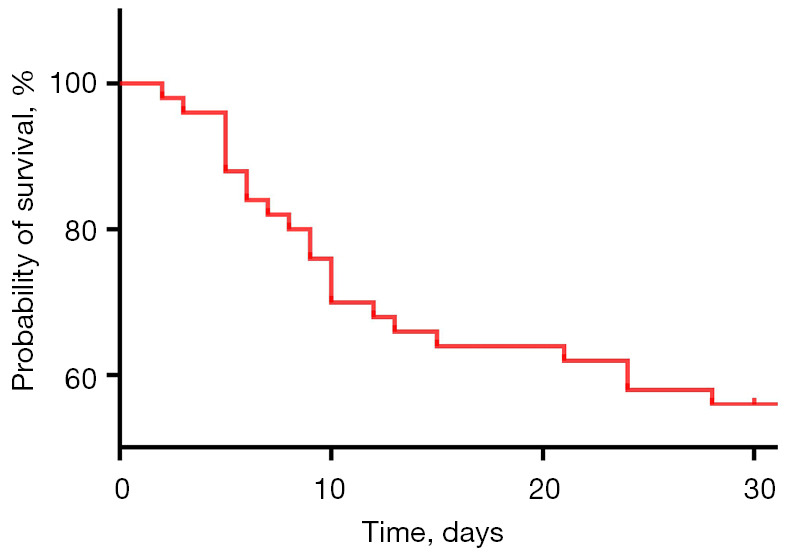
The Kaplan-Meier survival analysis curve at 28 days following treatment with colistin sulfate.
Pathogens
There were 14 patients with possible polymicrobial infections. Fifteen patients presented with multiple sites of infection. Seventy pathogens were isolated in total. There were 23 (32.9%) carbapenem-resistant Acinetobacter baumannii (CR-Ab), 20 (28.6%) carbapenem-resistant Klebsiella pneumoniae (CR-Kp), 12 (17.1%) carbapenem-resistant Pseudominas aeruginosa (CR-Pa), three (4.3%) fungus, and nine (12.9%) other pathogens. Fifty patients received between 2 to 5 antibiotics per day. The most common combined anti-infective therapy was colistin sulfate with carbapenem (40%). Five patients received concomitant tigecycline treatment (10%).
Colistin sulfate administration
In total, 50 patients were administered colistin sulfate at 1.0–1.5 million IU/day. Three patients received a dose of 1.0 million IU/day, and the other 47 patients received a dose of 1.5 million IU/day. The cumulative dose was 17.7±7.9 million IU, and the average duration of colistin sulfate use was 11 days (range, 7–16.3 days).
Analysis of therapy and mortality
The distribution of various characteristics included demographics, co-morbid conditions, pathogens and nephrotoxicity were compared between survivors and non-survivors. However, the duration and cumulative dose of colistin sulfate in survivors were higher than in the non-survivor group at 28-day follow-up (P=0.002 and 0.001, respectively). The nephrotoxicity rate before and after colistin sulfate therapy was higher in the non-survivor group than in the survivor group (P=0.013 and 0.015, respectively). The rate of CRRT was higher in the non-survivor group (P=0.02) (Table 2). The 28-day mortality was 65% in patients who developed nephrotoxicity after colistin sulfate treatment compared to 30% in patients without nephrotoxicity after treatment. The survival of patients is shown in Figure 3.
Table 2. Characteristics associated with 28-day mortality among patients who received colistin sulfate.
| Characteristics | Survivors (n=28) | Non-survivors (n=22) | P value |
|---|---|---|---|
| Age (years) | 66 (47.5–84.3) | 79 (65.8–88) | 0.78 |
| Male | 22 (78.6) | 18 (81.8) | 1.0 |
| Weight (kg) | 60 (55.0–75.0) | 59 (54.3–70.0) | 0.445 |
| T (℃) | 38.4±0.81 | 37.9±1.1 | 0.098 |
| SOFA score | 10.0±4.3 | 12.0±4.1 | 0.119 |
| APACHE II score | 23.2±6 | 25.6±3.8 | 0.084 |
| MV | 23 (82.1) | 19 (86.4) | 0.988 |
| CRRT | 3 (10.7) | 11 (50.0) | 0.02 |
| Shock | 15 (53.6) | 14 (63.6) | 0.569 |
| Dose | 1.5 (1.5–1.5) | 1.5 (1.5–1.5) | 0.117 |
| ICU stay (days) | 42 (21.3–61.3) | 24 (16.5–31.5) | 0.007 |
| Total length of stay (days) | 57 (268–87.8) | 31.5 (18.8–41.8) | 0.007 |
| MV (days) | 25.5 (14.3–58.5) | 20 (11.5–30) | 0.17 |
| Duration of CS use (days) | 14.5 (9.3–19.8) | 10 (6–11.5) | 0.002 |
| Cumulative CS dose (million IU) | 20.71±8.36 | 13.9±5.4 | 0.001 |
| WBC (109/L) | 11.56 (7.0–17.9) | 12.11 (8.4–18.3) | 0.792 |
| N (109/L) | 8.75 (5.7–15.6) | 12.4 (7.0–22.5) | 0.348 |
| CRP (mg/L) | 89.6 (64.2–146.5) | 131.7 (87.4–200.2) | 0.107 |
| PCT (ng/mL) | 2.38 (0.8–7.0) | 2.21 (1.3–6.0) | 0.703 |
| PLT (109/L) | 120 (71–198) | 76 (36.5–162.5) | 0.113 |
| TBIL (μmol/L) | 32.05 (19.2–89.0) | 23.8 (19.4–111.6) | 0.113 |
| Cr (μmol/L) | 82.15 (61.9–129.9) | 97.8 (68.6–119.7) | 0.406 |
| Alb (g/L) | 30.55 (28.5–34) | 31.45 (27.9–35.0) | 0.907 |
| Lac (mmol/L) | 2.6 (1.6–3.53) | 2.75 (1.78–4.3) | 0.525 |
| Bacteria eradication | 18 (64.3) | 11 (50.0) | 0.31 |
| Baseline nephrotoxicity | 8 (28.6) | 14 (63.6) | 0.013 |
| Nephrotoxicity after therapy | 7 (25.0) | 13 (59.1) | 0.015 |
Data are shown as mean ± SD, median (IQR) or n (%). IQR, interquartile range; SD, standard deviation; T, temperature; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; MV, mechanical ventilation; CRRT, continuous renal replacement therapy; ICU, intensive care unit; CS, colistin sulfate; WBC, white blood cell; N, neutrophils; CRP, C-reaction protein; PCT, procalcitonin; PLT, platelet; TBIL, total bilirubin; Cr, creatinine; Alb, albumin; Lac, lactate.
Figure 3.
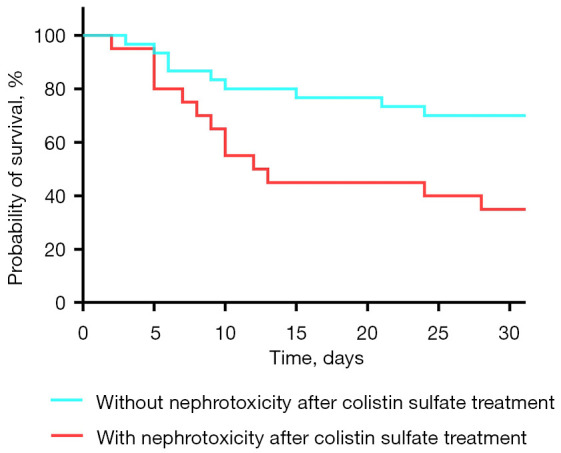
Kaplan-Meier survival curve comparing patients with and without nephrotoxicity after colistin sulfate treatment (log-rank, P<0.05).
Overall, the clinical condition of patients improved after colistin sulfate treatment, and temperature, neutrophil count, C-reaction protein (CRP), procalcitonin (PCT), Cr, and lactate levels were also significantly decreased (P<0.05).
The number of patients with nephrotoxicity significantly decreased after colistin sulfate treatment, which indicated that colistin sulfate could possibly improve renal function (P<0.001) (Table 3).
Table 3. Comparison of patient demographic characteristics at baseline and after therapy.
| Characteristics | Baseline | After therapy | P value |
|---|---|---|---|
| T (℃) | 38.2±1.0 | 37.3±0.8 | <0.001 |
| SOFA score | 10.9±4.3 | 12.0±6.2 | 0.118 |
| APACHE II score | 24.3±5.3 | 26.3±12.1 | 0.118 |
| MV | 42 (84.0) | 37 (74.0) | 0.003 |
| CRRT | 14 (28.0) | 15 (30.0) | <0.001 |
| Septic shock | 29 (58.0) | 19 (38.0) | 0.07 |
| WBC (109/L) | 11.6 (7.9–18.0) | 10.2 (6.8–15.2) | 0.255 |
| N (109/L) | 9.6 (6.7–16.5) | 7.8 (5.5–11.6) | 0.041 |
| CRP (mg/L) | 113.2 (74.1–165.5) | 70.8 (45.0–110.1) | 0.001 |
| PCT (ng/mL) | 2.2 (0.9–6.0) | 1.2 (0.5–3.7) | 0.024 |
| PLT (109/L) | 91 (60.5–188.3) | 69.3 (40.0–173.8) | 0.191 |
| TBIL (μmol/L) | 27.4 (19.4–91.8) | 32.9 (17.3–217.9) | 0.062 |
| Cr (μmol/L) | 91.4 (66.8–121.8) | 80.2 (60.8–122.9) | 0.035 |
| Alb (g/L) | 31.1 (28.3–34.2) | 31.9 (29.1–34.3) | 0.54 |
| Lac (mmol/L) | 2.6 (1.7–3.6) | 3.4 (1.4–11.3) | 0.017 |
| Nephrotoxicity | 22 (44.0) | 12 (24.0) | <0.001 |
Data are shown as mean ± SD, median (IQR) or n (%). IQR, interquartile range; SD, standard deviation; T, temperature; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; MV, mechanical ventilation; CRRT, continuous renal replacement therapy; WBC, white blood cell; N, neutrophils; CRP, C-reaction protein; PCT, procalcitonin; PLT, platelet; TBIL, total bilirubin; Cr, creatinine; Alb, albumin; Lac, lactate.
Risk factors related to the occurrence of acute kidney injury (AKI)
The characteristics of patients with and without nephrotoxicity after colistin sulfate treatment were analyzed (Table 4).
Table 4. Comparison of demographic characteristics of patients with and without AKI after discontinuation.
| Characteristics | AKI after treatment (n=20) | Without AKI after treatment (n=30) | P value |
|---|---|---|---|
| Age (years) | 79.5 (68.3–88.0) | 65.5 (50.0–82.8) | 0.039 |
| Male | 15 (75.0) | 25 (83.3) | 0.718 |
| Weight (kg) | 58.0 (55.0–68.8) | 64.0 (54.3–70.5) | 0.606 |
| T (℃) | 38.0±1.0 | 38.3±0.9 | 0.236 |
| SOFA score | 12.2±5.2 | 10.0±3.5 | 0.089 |
| APACHE-II score | 25.2±4.5 | 23.7±5.7 | 0.333 |
| MV | 19 (95.0) | 23 (76.7) | 0.181 |
| MV days | 22 (10.5–32.3) | 22.3 (14.3–48.8) | 0.858 |
| CRRT | 10 (50.0) | 4 (13.3) | 0.005 |
| Shock | 12 (60.0) | 17 (56.7) | 0.815 |
| ICU stay (days) | 29.5 (20.5–42.5) | 33.5 (20.0–53.3) | 0.937 |
| Total length of stay (days) | 35 (23.0–66.5) | 49.5 (25.3–70.8) | 0.476 |
| 28-day mortality | 13 (65.0) | 9 (30.0) | 0.015 |
| Duration of CS use (days) | 11 (6.3–13.0) | 11.5 (8.3–18.8) | 0.427 |
| Cumulative CS dose (106 IU) | 16.1±6.7 | 18.8±8.6 | 0.234 |
| WBC (109/L) | 11.5 (8.9–15.7) | 11.4 (6.0–18.5) | 0.593 |
| N (109/L) | 8.4 (6.9–15.9) | 9.6 (5.5–16.3) | 0.984 |
| CRP (mg/L) | 106.6 (64.2–146.3) | 120.8 (77.7–171.2) | 0.812 |
| PCT (ng/mL) | 2.2 (1.1–4.4) | 3.1 (0.8–9.0) | 0.961 |
| PLT (109/L) | 108.5 (40.0–193.3) | 84.0 (64.0–190.8) | 0.804 |
| TBIL (μmol/L) | 46.4 (19.4–117.0) | 25.1 (18.3–65.5) | 0.572 |
| Baseline Cr level (μmol/L) | 109.0 (84.6–189.9) | 78.6 (61.3–106.8) | 0.004 |
| Alb (g/L) | 30.8 (27.7–32.2) | 31.6 (28.6–35.5) | 0.157 |
| Lac (mmol/L) | 3.0 (1.5–6.0) | 2.6 (1.7–3.2) | 0.322 |
| Bacteria eradication | 11 (55.0) | 18 (60.0) | 0.726 |
| Baseline nephrotoxicity | 17 (85.0) | 5 (16.7) | <0.001 |
Data are shown as mean ± SD, median (IQR) or n (%). IQR, interquartile range; SD, standard deviation; AKI, acute kidney injury; T, temperature; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; MV, mechanical ventilation; CRRT, continuous renal replacement therapy; ICU, intensive care unit; CS, colistin sulfate; WBC, white blood cell; N, neutrophils; CRP, C-reaction protein; PCT, procalcitonin; PLT, platelet; TBIL, total bilirubin; Cr, creatinine; Alb, albumin; Lac, lactate.
The duration and the cumulative dose of colistin sulfate were not significantly different between the two groups (P=0.427 and P=0.234, respectively), although patients without nephrotoxicity had reduced baseline Cr levels [78.6 (range, 61.3–106.8) vs. 109.4 (range, 84.6–189.9), P=0.004]. The outcomes analysis showed that patients with nephrotoxicity had increased all-cause mortality and an increased prevalence of baseline nephrotoxicity, and a higher rate of CRRT treatment.
Backward logistic regression showed that a higher baseline Cr level was independently associated with nephrotoxicity. Interestingly, there were no significant differences in the duration and dose of colistin sulfate (Table 5).
Table 5. Univariate and multivariate analysis of nephrotoxicity after therapy in patients receiving colistin sulfate.
| Variables | Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|---|
| Odds ratio | 95% CI | P value | Odds ratio | 95% CI | P value | ||
| Albumin | 0.788 | 0.63–0.99 | 0.037 | 0.899 | 0.77–1.06 | 0.186 | |
| Lac | 1.316 | 0.80–2.17 | 0.281 | ||||
| SOFA score | 1.467 | 1.02–2.11 | 0.04 | 1.231 | 1.00–1.52 | 0.054 | |
| APACHE II score | 0.891 | 0.71–1.12 | 0.324 | ||||
| Cr | 1.026 | 1.00–1.05 | 0.030 | 1.013 | 1.00–1.03 | 0.028 | |
| WBC | 1.040 | 0.92–1.18 | 0.535 | ||||
| CRP | 1.001 | 0.99–1.01 | 0.883 | ||||
| PCT | 0.897 | 0.79–1.02 | 0.104 | ||||
| PLT | 1.014 | 1.00–1.03 | 0.026 | 1.007 | 1.00–1.02 | 0.109 | |
| Duration of CS use (days) | 0.947 | 0.78–1.15 | 0.582 | ||||
| Dose of CS | 0.959 | 0.87–1.07 | 0.404 | ||||
CI, confidence interval; Lac, lactate; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; Cr, creatinine; WBC, white blood cell; CRP, C-reaction protein; PCT, procalcitonin; PLT, platelet; CS, colistin sulfate.
Discussion
In recent years, polymyxins have been reinstated as a last-line treatment for severe CR-GNB infections. Some studies have reported on the effectiveness and safety of CMS and PMB: according to previously documented outcomes, the clinical cure rate of CMS varies from 41% to 67%, and the AKI rate varies from 26% to 50% (21,22). The rate of nephrotoxicity for PMB was found to range from 20% to 60% in previous studies (23-28). But the data for colistin sulfate has been lacking.
In this study, patients with serious CR-GNB infections treated with colistin sulfate had a bacterial eradication rate of 40%, and the all-cause mortality at 28 days was 44%. ICU-related mortality was 50%. These results were compared with previous studies of serious CR-GNB infections treated with polymyxins or other antibiotic drugs. According to these previous studies, the mortality of patients treated with other antibiotic therapies ranged from 45% to 63% (29-31). One systematic review showed that patients with CR-GNB infections who were given inappropriate antibiotic treatment had higher mortality. Receiving inappropriate antibiotic therapy is a mortality risk factor for patients with CR-GNB, and the mortality rate was reported as 86% in this particular review (32).
Our study found that after colistin sulfate therapy, the patients’ temperature decreased to normal, and CRRT and mechanical ventilation rates were significantly decreased. Furthermore, infection indicators, including neutrophil count, CRP, and PCT levels, were also significantly reduced. The Cr level representing renal function declined as well. The lactate level, indicative of septic shock, also reduced markedly. Of note, the survivors received a longer duration of colistin sulfate treatment.
A case report shared the experience of using intravenous colistin sulfate in one patient with extensive drug-resistant Acinetobacter baumannii. After therapy, the patient’s symptoms improved, circulation stabilized, and kidney function improved (33). Our results also suggested that colistin sulfate may be a clinically effective treatment for patients infected with CR-GNB. But larger randomized controlled trials are needed to validate our findings.
This study retrospectively summarized nephrotoxicity after colistin sulfate treatment for CR-GNB. The rate of renal dysfunction present decreased after therapy with colistin from 44% to 24%, one could reasonably extrapolate that therapy with the correct antibiotic (colistin in this case) led to a resolution of infection and reversed the renal dysfunction. One reason for this may be that the baseline condition before colistin sulfate treatment might have been caused by severe infection and was reversed by antibiotic treatment. The prevalence of nephrotoxicity in our study was lower than PMB or CMS in other observational studies. In this group bilirubin levels were unaffected by colistin therapy and significant hepatic dysfunction was not noted in association with colistin therapy. Our analysis suggests that colistin therapy is safe in patients with CR-GNB infections.
Some studies have reported that chronic kidney disease (CKD) increases the risk of AKI (23,34). As our study included 50 patients, with only five having a history of CKD, the small sample influenced our analysis. However, our study found that the baseline Cr level was an independent risk factor for the occurrence of nephrotoxicity after therapy. It is also possible that the renal impairment of patients in our study may have been complicated by other factors, such as other nephrotoxic drug use, multiple organ dysfunction syndrome, and septic shock.
Multiple studies have shown that polymyxin B has dose-dependent nephrotoxicity (27,35,36). Nelson et al. found a dose of ≥250 mg per day was associated with a higher incidence of AKI (37). In contrast, the dosage and duration of colistin sulfate treatment were not significantly correlated with nephrotoxicity in our study. Colistin sulfate seems to cause less damage to renal functioning than polymyxin B or CMS. With this finding, we suggest that despite the initial renal dysfunction, clinicians should consider using colistin sulfate. Moreover, compared with PMB, we did not find any other adverse events, such as skin hyperpigmentation or neurotoxicity.
In this study the presence of underlying renal dysfunction, chronic renal failure and the need for dialysis were, as expected, associated with an increased mortality at 28 days. The survivors in our study had a longer duration of colistin sulfate treatment.
Colistin sulfate has only been listed in China for a short time and its clinical application is not widespread. We observed that the dosage was usually not adjusted according to the patients’ weight.
This study has limitations, a retrospective single centre cohort of 50 patients limits the widespread applicability of our data. The lack of a control or comparator group prevented direct comparisons with polymyxin B or combination therapies such as carbapenems, tigecycline, fosfomycin, aminoglycosides or rifampicin. Additional antibiotics were prescribed at the discretion of the senior clinicians; therefore, treatment effect may not be attributed entirely to the effects of colistin sulfate. Another limitation was the small sample of patients included in our study because the single-center design and small sample size limited the validity of our findings.
Conclusions
We would suggest, based upon an overall favorable response rate of 58% and bacterial clearance rate of 40% that Colistin is an effective treatment for CR-GNB infections. The baseline Cr level was an independent risk factor for nephrotoxicity, which was independent of the dosage and duration of colistin sulfate treatment. Large, prospective randomized controlled trials are needed in the future to investigate the efficacy and safety of intravenous colistin sulfate.
Supplementary
The article’s supplementary files as
Acknowledgments
The authors appreciate the academic support from AME Sepsis Collaborative Group.
Funding: This work was supported by the General Project Funds from the Health Department of Zhejiang Province (Nos. 2021KY481 and 2018KY269) and the Public Welfare Project of Zhejiang Provincial Department of Science and Technology (No. LGF22H150018).
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Ethics Committee of Zhejiang Provincial People’s Hospital (No. QT2022190). And individual consent for this retrospective analysis was waived.
Footnotes
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://atm.amegroups.com/article/view/10.21037/atm-22-4959/rc
Data Sharing Statement: Available at https://atm.amegroups.com/article/view/10.21037/atm-22-4959/dss
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-4959/coif). The authors have no conflicts of interest to declare.
References
- 1.Cecconi M, Evans L, Levy M, et al. Sepsis and septic shock. Lancet 2018;392:75-87. 10.1016/S0140-6736(18)30696-2 [DOI] [PubMed] [Google Scholar]
- 2.van Duin D, Doi Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence 2017;8:460-9. 10.1080/21505594.2016.1222343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ernst CM, Braxton JR, Rodriguez-Osorio CA, et al. Adaptive evolution of virulence and persistence in carbapenem-resistant Klebsiella pneumoniae. Nat Med 2020;26:705-11. 10.1038/s41591-020-0825-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Li J, Nation RL, Turnidge JD, et al. Colistin: the re-emerging antibiotic for multidrug-resistant Gram-negative bacterial infections. Lancet Infect Dis 2006;6:589-601. 10.1016/S1473-3099(06)70580-1 [DOI] [PubMed] [Google Scholar]
- 5.Velkov T, Roberts KD, Thompson PE, et al. Polymyxins: a new hope in combating Gram-negative superbugs? Future Med Chem 2016;8:1017-25. 10.4155/fmc-2016-0091 [DOI] [PubMed] [Google Scholar]
- 6.Nang SC, Azad MAK, Velkov T, et al. Rescuing the Last-Line Polymyxins: Achievements and Challenges. Pharmacol Rev 2021;73:679-728. 10.1124/pharmrev.120.000020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sabnis A, Hagart KL, Klöckner A, et al. Colistin kills bacteria by targeting lipopolysaccharide in the cytoplasmic membrane. Elife 2021;10:65836. 10.7554/eLife.65836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McCall IC, Shah N, Govindan A, et al. Antibiotic Killing of Diversely Generated Populations of Nonreplicating Bacteria. Antimicrob Agents Chemother 2019;63:e02360-18. 10.1128/AAC.02360-18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Avedissian SN, Liu J, Rhodes NJ, et al. A Review of the Clinical Pharmacokinetics of Polymyxin B. Antibiotics (Basel) 2019;8:31. 10.3390/antibiotics8010031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.El-Sayed Ahmed MAE, Zhong LL, Shen C, et al. Colistin and its role in the Era of antibiotic resistance: an extended review (2000-2019). Emerg Microbes Infect 2020;9:868-85. 10.1080/22221751.2020.1754133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vardakas KZ, Falagas ME. Colistin versus polymyxin B for the treatment of patients with multidrug-resistant Gram-negative infections: a systematic review and meta-analysis. Int J Antimicrob Agents 2017;49:233-8. 10.1016/j.ijantimicag.2016.07.023 [DOI] [PubMed] [Google Scholar]
- 12.Wagenlehner F, Lucenteforte E, Pea F, et al. Systematic review on estimated rates of nephrotoxicity and neurotoxicity in patients treated with polymyxins. Clin Microbiol Infect 2021. [Epub ahead of print]. doi: . 10.1016/j.cmi.2020.12.009 [DOI] [PubMed] [Google Scholar]
- 13.Zheng G, Cao L, Che Z, et al. Polymyxin B-induced skin hyperpigmentation: a rare case report and literature review. BMC Pharmacol Toxicol 2018;19:41. 10.1186/s40360-018-0226-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Li YM, Milikowski C, Selvaggi G, et al. Polymyxin B-induced skin hyperpigmentation. Transpl Infect Dis 2020;22:e13312. 10.1111/tid.13312 [DOI] [PubMed] [Google Scholar]
- 15.Wen X, Luo C, Lyu W. Polymyxin B-Induced Skin Hyperpigmentation. Case Rep Med 2020;2020:6461329. 10.1155/2020/6461329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sisay M, Hagos B, Edessa D, et al. Polymyxin-induced nephrotoxicity and its predictors: a systematic review and meta-analysis of studies conducted using RIFLE criteria of acute kidney injury. Pharmacol Res 2021;163:105328. 10.1016/j.phrs.2020.105328 [DOI] [PubMed] [Google Scholar]
- 17.Yu XB, Zhang XS, Wang YX, et al. Population Pharmacokinetics of Colistin Sulfate in Critically Ill Patients: Exposure and Clinical Efficacy. Front Pharmacol 2022;13:915958. 10.3389/fphar.2022.915958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Xie YL, Jin X, Yan SS, et al. Population pharmacokinetics of intravenous colistin sulfate and dosage optimization in critically ill patients. Front Pharmacol 2022;13:967412. 10.3389/fphar.2022.967412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yu XB, Huang YY, Zhang XS, et al. Intraventricular colistin sulphate as a last resort therapy in a patient with multidrug-resistant Acinetobacter baumannii induced post-neurosurgical ventriculitis. Br J Clin Pharmacol 2022;88:3490-4. 10.1111/bcp.15238 [DOI] [PubMed] [Google Scholar]
- 20.Kdigo K., Acute Kidney Injury Work Group : KDIGO clinical practice guideline for acute kidney injury. Kidney International Supplement 2012;2:1-138. [Google Scholar]
- 21.Trifi A, Abdellatif S, Daly F, et al. Efficacy and Toxicity of High-Dose Colistin in Multidrug-Resistant Gram-Negative Bacilli Infections: A Comparative Study of a Matched Series. Chemotherapy 2016;61:190-6. 10.1159/000442786 [DOI] [PubMed] [Google Scholar]
- 22.Elefritz JL, Bauer KA, Jones C, et al. Efficacy and Safety of a Colistin Loading Dose, High-Dose Maintenance Regimen in Critically Ill Patients With Multidrug-Resistant Gram-Negative Pneumonia. J Intensive Care Med 2017;32:487-93. 10.1177/0885066616646551 [DOI] [PubMed] [Google Scholar]
- 23.Crass RL, Rutter WC, Burgess DR, et al. Nephrotoxicity in Patients with or without Cystic Fibrosis Treated with Polymyxin B Compared to Colistin. Antimicrob Agents Chemother 2017;61:e02329-16. 10.1128/AAC.02329-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Osorio J, Barreto J, Samboni CF, et al. Risk factors for acute kidney injury in patients treated with polymyxin B experience from 139 cases at a tertiary university hospital in Colombia. Rev Chilena Infectol 2017;34:7-13. 10.4067/S0716-10182017000100001 [DOI] [PubMed] [Google Scholar]
- 25.Soares DS, Reis ADF, Silva GBD, Junior, et al. Polymyxin-B and vancomycin-associated acute kidney injury in critically ill patients. Pathog Glob Health 2017;111:137-42. 10.1080/20477724.2017.1309338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rigatto MH, Oliveira MS, Perdigão-Neto LV, et al. Multicenter Prospective Cohort Study of Renal Failure in Patients Treated with Colistin versus Polymyxin B. Antimicrob Agents Chemother 2016;60:2443-9. 10.1128/AAC.02634-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang X, Qi S, Duan X, et al. Clinical outcomes and safety of polymyxin B in the treatment of carbapenem-resistant Gram-negative bacterial infections: a real-world multicenter study. J Transl Med 2021;19:431. 10.1186/s12967-021-03111-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ngamprasertchai T, Boonyasiri A, Charoenpong L, et al. Effectiveness and safety of polymyxin B for the treatment of infections caused by extensively drug-resistant Gram-negative bacteria in Thailand. Infect Drug Resist 2018;11:1219-24. 10.2147/IDR.S169939 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bassetti M, Echols R, Matsunaga Y, et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect Dis 2021;21:226-40. 10.1016/S1473-3099(20)30796-9 [DOI] [PubMed] [Google Scholar]
- 30.Wu X, Zhu Y, Chen Q, et al. Tigecycline Therapy for Nosocomial Pneumonia due to Carbapenem-Resistant Gram-Negative Bacteria in Critically Ill Patients Who Received Inappropriate Initial Antibiotic Treatment: A Retrospective Case Study. Biomed Res Int 2016;2016:8395268. 10.1155/2016/8395268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Geng TT, Xu X, Huang M. High-dose tigecycline for the treatment of nosocomial carbapenem-resistant Klebsiella pneumoniae bloodstream infections: A retrospective cohort study. Medicine (Baltimore) 2018;97:e9961. 10.1097/MD.0000000000009961 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Du X, Xu X, Yao J, et al. Predictors of mortality in patients infected with carbapenem-resistant Acinetobacter baumannii: A systematic review and meta-analysis. Am J Infect Control 2019;47:1140-5. 10.1016/j.ajic.2019.03.003 [DOI] [PubMed] [Google Scholar]
- 33.Xue X, Zhou T, Wang G, et al. Treatment of pulmonary infection of extensively drug-resistant Acinetobacter baumannii with intravenous colistin sulfate combined with atomization: a case report. Ann Palliat Med 2021;10:9288-96. 10.21037/apm-21-2112 [DOI] [PubMed] [Google Scholar]
- 34.John JF, Falci DR, Rigatto MH, et al. Severe Infusion-Related Adverse Events and Renal Failure in Patients Receiving High-Dose Intravenous Polymyxin B. Antimicrob Agents Chemother 2018;62:e01617-17. 10.1128/AAC.01617-17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Chang K, Wang H, Zhao J, et al. Risk factors for polymyxin B-associated acute kidney injury. Int J Infect Dis 2022;117:37-44. 10.1016/j.ijid.2022.01.055 [DOI] [PubMed] [Google Scholar]
- 36.Xia GL, Jiang RL. Efficacy and safety of polymyxin B in carbapenem-resistant gram-negative organisms infections. BMC Infect Dis 2021;21:1034. 10.1186/s12879-021-06719-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nelson BC, Eiras DP, Gomez-Simmonds A, et al. Clinical outcomes associated with polymyxin B dose in patients with bloodstream infections due to carbapenem-resistant Gram-negative rods. Antimicrob Agents Chemother 2015;59:7000-6. 10.1128/AAC.00844-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as