
Fig. 1.
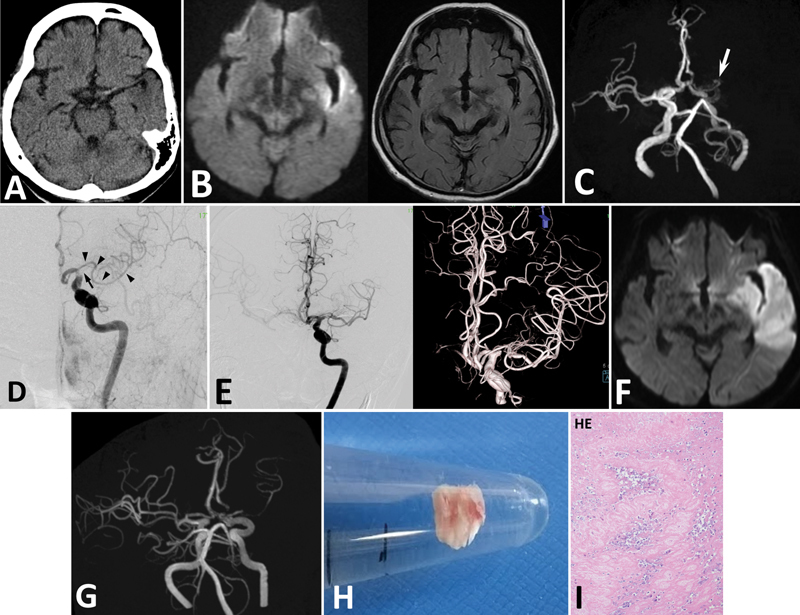
Case 1. ( A ) CT demonstrating a high density in the left MCA, but no low-density area in the left cerebrum. ( B ) DWI of MRI demonstrating a high-intensity region in the left cerebrum ( left panel ). FLAIR images showing no high-intensity region in the left cerebrum ( right ). ( C ) MRA faintly demonstrating the left ICA, and a small artery originating from ACA ( arrow ). However, opacification of this AMCA is not clear. ( D ) Angiography showing defect of contrast medium in the left ICA and MCA indicating thromboembolism. The main trunk of MCA is occluded at its origin ( arrow ). AMCA originates from ACA ( arrowheads ). ( E ) After endovascular treatment, the left MCA trunk is recanalized with residual stenosis in M1 of MCA. AMCA is patent. MRI ( F ) and MRA ( G ) on the next day showing cerebral infarction in the MCA territory, and re-occlusion of the main MCA. ( H ) The removed thrombus is a white thrombus. ( I ) Pathological examination of the thrombus revealing that it is composed of fibrous tissue and white blood cells (100×). HE; hematoxylin and eosin stain.