
Figure 6. Pathophysiological characteristics of the 4 major apoB dyslipoproteinemic phenotypes.
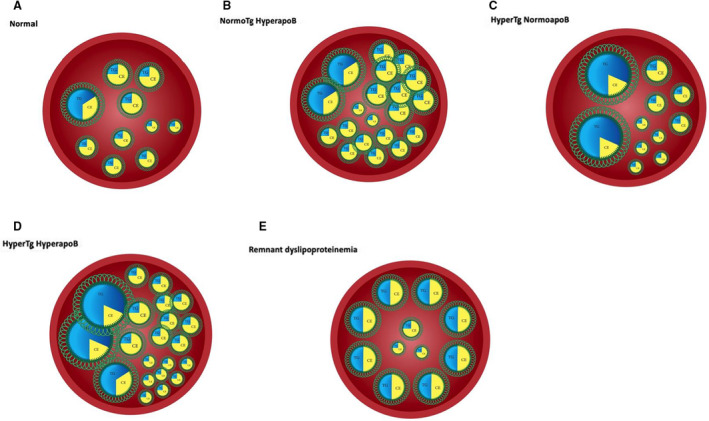
A, Normal number of VLDL and LDL particles within an arterial lumen. B, Increased number of VLDL particles with an increased number of cholesterol‐rich LDL particles. Familial hypercholesterolemia is the prototypic disorder that represents the extreme manifestations of this phenotype. C, Relative number of VLDL and LDL particles within an arterial lumen in a patient with hyperTG normoapoB. The VLDL particles are enriched in triglycerides or increased in number, but LDL particle number is normal. The net result is that apoB is normal. Familial hypertriglyceridemia is present when this is the dominant phenotype within a family. D, Increased number of VLDL and LDL particles within the arterial lumen of a patient with hyperTG hyperapoB. This occurs because of increased production of VLDL and LDL particles in hyperTG hyperapoB. Familial combined hyperlipidemia represents the expression of this disorder within a family. Levels of apoB are >120 mg/d (>90th percentile) in subjects with familial combined hyperlipidemia. E, Markedly increased number of cholesterol‐enriched VLDL and chylomicron remnants with a normal number of LDL particles in a patient with dysbetalipoproteinemia (type III hyperlipoproteinemia). apoB indicates apolipoprotein B; CE, cholesterol ester; hyperTG hyperapoB, hypertriglyceridemic hyperapoB; hyperTG normoapoB, hypertriglyceridemic normal apoB; LDL, low‐density lipoprotein; TG, triglycerides; and VLDL, very low‐density lipoprotein.