

This study assesses whether vitamin D supplementation prevents statin-associated muscle symptoms and reduces statin discontinuation.
Key Points
Question
Does vitamin D prevent statin-associated muscle symptoms and reduce statin discontinuation?
Findings
The 2083 participants in a randomized, double-blind trial of vitamin D supplementation who initiated statin therapy during follow-up and responded to a survey were equally likely to develop muscle symptoms (31% vs 31%) and discontinue statin therapy (13% vs 13%), whether assigned to vitamin D or to placebo.
Meaning
In this study, vitamin D supplementation did not prevent statin-associated muscle symptoms or statin discontinuation.
Abstract
Importance
Statin-associated muscle symptoms (SAMS) are common and may lead to discontinuation of indicated statin therapy. Observational studies suggest that vitamin D therapy is associated with reduced statin intolerance, but no randomized studies have been reported.
Objective
To test whether vitamin D supplementation was associated with prevention of SAMS and a reduction of statin discontinuation.
Design, Setting, and Participants
Men 50 years or older and women 55 years or older, free of cancer and cardiovascular disease, were enrolled in a randomized, placebo-controlled, double-blind clinical trial of vitamin D supplementation. Participants who initiated statin therapy after randomization were surveyed in early 2016. The data were analyzed in early 2022.
Interventions
Daily cholecalciferol (2000 international units) or placebo with assessment of statin prescriptions during follow-up.
Main Outcomes and Measures
Muscle pain or discomfort lasting several days (primary outcome) and discontinuation of a statin due to SAMS (secondary outcome).
Results
Statins were initiated by 1033 vitamin D–assigned participants and 1050 placebo-assigned participants; mean (SD) age was 66.8 (6.2) years and 49% were women. Over 4.8 years of follow-up, SAMS were reported by 317 participants (31%) assigned vitamin D and 325 assigned placebo (31%). The adjusted odds ratio (OR) was 0.97 (95% CI, 0.80-1.18; P = .78). Statins were discontinued by 137 participants (13%) assigned to vitamin D and 133 assigned to placebo (13%) with an adjusted OR of 1.04 (95% CI, 0.80-1.35; P = .78). These results were consistent across pretreatment 25-hydroxy vitamin D levels (interaction P value = .83). Among participants with levels less than 20 ng/mL, SAMS were reported by 28 of 85 vitamin D–assigned participants (33%) and 33 of 95 placebo-assigned participants (35%). For those with levels less than 30 ng/ml, SAMS were reported by 88 of 330 vitamin–D assigned participants (27%) and 96 of 323 of placebo-assigned participants (30%).
Conclusions and Relevance
Vitamin D supplementation did not prevent SAMS or reduce statin discontinuation. These results were consistent across pretreatment 25-hydroxy vitamin D levels.
Trial Registration
ClinicalTrials.gov Identifier: NCT01169259
Introduction
Statin-associated muscle symptoms (SAMS) are common and often lead to discontinuation of statins.1,2,3,4,5,6 Several observational studies have shown that low levels of vitamin D are associated with the development of SAMS7,8 and plausible mechanisms have been proposed that link low levels of vitamin D to development of SAMS.8 Nonrandomized, uncontrolled studies have also reported that many patients who discontinued taking a statin because of SAMS and were then treated with vitamin D were able to tolerate reintroduction of a statin.8,9,10,11,12,13 Vitamin D supplementation may be particularly effective in preventing SAMS among patients with low levels of vitamin D (ie, less than 30 ng/mL [to convert to nmol, multiply by 2.496] of 25-hydroxy vitamin D [25-OHD]).8 Prior studies suggest vitamin D may reduce statin intolerance, but they were neither randomized nor blinded and lacked control groups.9,10,11,12,13 To our knowledge, no randomized, placebo-controlled clinical trials of vitamin D supplementation to prevent or treat SAMS have been reported.8,9
The Vitamin D and Omega-3 trial (VITAL) study randomized 25 871 participants to double-blind vitamin D supplementation to determine whether it would prevent cardiovascular disease and cancer14,15 and provided a unique opportunity to test whether vitamin D reduces SAMS among participants who initiated statins. The goal of this VITAL substudy was to test whether vitamin D was associated with significant reduction in SAMS among new statin users and to determine whether vitamin D would be more effective among participants with low prerandomization levels of serum 25-OHD.
Methods
The VITAL randomized trial has been described in detail previously.14 In brief, men 50 years or older and women 55 years or older without a history of either cardiovascular disease or cancer (other than nonmelanoma skin cancer) were enrolled in a 2 × 2 factorial, double-blind randomized trial of vitamin D supplements vs placebo and of ω-3 fatty acid supplements vs placebo. Participants randomized to vitamin D received 2000 international units of cholecalciferol per day. Participants completed VITAL study questionnaires at baseline and during follow-up that recorded the medications they were taking. Roughly two-thirds of the VITAL participants provided blood samples at baseline, which were assayed for serum 25-OHD using liquid chromatography–tandem mass spectroscopy that was standardized and calibrated by the US Centers for Disease Control and Prevention.15 The VITAL trial was approved by the institutional review board of Partners HealthCare-Brigham and Women’s Hospital and all participants provided written informed consent to participate and complete study questionnaires during follow-up.
VITAL participants who were not taking a statin at baseline and who reported that they were taking a statin in at least 1 of the follow-up questionnaires were identified as presumed new statin users. As previously described,16 in early 2016, we mailed the surviving presumed new statin users a survey about their statin use and muscle symptoms. The survey asked for the name of the statin(s) they used, whether they had musculoskeletal pain or discomfort while taking a statin that persisted for more than a few days, and whether they stopped taking the statin because of this discomfort (eAppendix in Supplement 1).
The study population consisted of the presumed new statin users who responded to the survey, confirmed initiating a statin after enrolling in VITAL, and responded to the questions about muscle symptoms. The primary end point was the development of muscle symptoms while taking a statin and the secondary end point was discontinuation of a statin due to muscle symptoms.
We first compared baseline characteristics by randomized group among those in the substudy to ensure comparability. Our primary analysis compared the frequency of muscle symptoms and statin discontinuation between the participants randomly assigned to vitamin D or placebo. We prespecified that outcomes would be compared using multivariable logistic regression models that adjusted for the baseline characteristics previously found to be associated with SAMS in the VITAL participants,16 namely age, sex, race (African American vs non–African American), and BMI, as well as any other baseline variables that were found to differ significantly between the 2 randomized groups. We compared baseline characteristics using the χ2 tests and outcomes using multivariable logistic regression using SAS version 9.4 (SAS Institute).
Results
A total of 25 871 participants were randomized in VITAL between November 2011 and March 2014; mean (SD) age was 67.1 (6.2) years and 51% were women (Figure 1). At study entry, 8890 participants (34%) were taking a statin, and 2835 participants who were not taking a statin at baseline reported taking a statin during a mean follow-up of 4.8 years (from randomization through early 2016). Almost all of the surviving presumed new statin users (88%) responded to the study survey; the nonresponders had higher levels of cardiac risk factors (eTable in Supplement 1). The 2083 survey respondents who confirmed statin initiation formed the study population (8% of all participants randomized in VITAL).
Figure 1. Flow Diagram of Study Participants.

SAMS indicates statin-associated muscle symptoms; VITAL, Vitamin D and Omega-3 trial.
The baseline characteristics of the 1033 participants randomly assigned to vitamin D were very similar to those of the 1050 participants randomly assigned to placebo (Table 1) apart from a small excess of placebo-assigned participants who drank alcohol daily. Muscle symptoms while taking a statin were reported by 317 participants (31%) assigned to vitamin D and by 325 assigned to placebo (31%) (Figure 2), a nonsignificant difference. The unadjusted odds ratio (OR) was 0.97 (95% CI, 0.81-1.17; P = .75) and the adjusted OR was 0.97 (95% CI , 0.80-1.18; P = .78). Statin discontinuation due to muscle symptoms also did not differ between the randomized groups (Figure 2); 137 of the vitamin D–assigned participants (13%) vs 133 of the placebo-assigned group (13%) stopped taking a statin. The unadjusted OR was 1.05 (95% CI, 0.81-1.36; P = .71) and the adjusted OR was 1.04 (95% CI, 0.80-1.35; P = .78).
Table 1. Baseline Characteristics by Random Assignment in the Overall Population.
| Baseline factor | No. (%) | P value | |
|---|---|---|---|
| Placebo | Vitamin D | ||
| No. | 1050 | 1033 | |
| Age, y | |||
| 50-64 | 393 (37) | 413 (40) | .21 |
| 65-74 | 570 (54) | 522 (51) | |
| ≥75 | 87 (8) | 98 (9) | |
| Sex | |||
| Male | 546 (52) | 522 (51) | .50 |
| Female | 504 (48) | 511 (49) | |
| Race and ethnicitya | |||
| White (Non-Hispanic) | 732 (72) | 724 (73) | .99 |
| African-American | 200 (20) | 189 (19) | |
| Hispanic | 47 (5) | 45 (5) | |
| Asian/Pacific Islander | 18 (2) | 20 (2) | |
| Otherb or unknown | 13 (1) | 12 (1) | |
| BMI | |||
| <25 | 284 (28) | 278 (28) | .97 |
| 25 to <30 | 398 (39) | 399 (39) | |
| ≥30 | 339 (33) | 334 (33) | |
| Exercise, MET-h/wk | |||
| <6.7 | 344 (34) | 338 (34) | .99 |
| 6.7 to 24.92 | 351 (34) | 347 (34) | |
| ≥24.93 | 332 (32) | 324 (32) | |
| Education | |||
| <High school | 10 (1) | 17 (2) | .18 |
| High school graduate | 129 (12) | 103 (10) | |
| College | 415 (40) | 429 (41) | |
| Postcollege | 492 (47) | 484 (47) | |
| Hypertension | |||
| Absent | 453 (43) | 458 (44) | .60 |
| Present | 593 (57) | 572 (56) | |
| Diabetes | |||
| Absent | 877 (84) | 859 (83) | .78 |
| Present | 170 (16) | 172 (17) | |
| Smoking | |||
| Never | 507 (50) | 522 (52) | .39 |
| Past | 434 (42) | 393 (39) | |
| Current | 84 (8) | 82 (8) | |
| Alcohol use | |||
| None | 322 (31) | 312 (31) | .02 |
| <Daily | 420 (41) | 469 (46) | |
| ≥Daily | 294 (28) | 240 (24) | |
| Statins usedc | |||
| Atorvastatin | 515 (49) | 515 (50) | .82 |
| Simvastatin | 227 (22) | 207 (20) | |
| Pravastatin | 150 (14) | 150 (15) | |
| Rosuvastatin | 68 (6) | 77 (7) | |
| Other | 90 (9) | 84 (8) | |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); MET-h; metabolic equivalents per hour.
Race and ethnicity were self-reported.
Includes American Indian and Alaska Native.
Total more than 100% due to use of more than 1 statin by 220 participants (11%).
Figure 2. Statin-Associated Muscle Symptoms and Statin Discontinuation.

Participants With Measured Serum 25-OH Vitamin D Levels
Two-thirds of the study participants (1397 of 2083) had serum 25-OHD levels measured prior to randomization. The baseline characteristics of these participants were similar in the vitamin–D assigned and placebo-assigned groups (Table 2). Baseline serum 25-OHD levels were virtually identical in the 2 treatment groups with equal means (30.4 ng/mL) and medians (30.0 ng/mL) (Table 2). A minority of participants had reduced baseline 25-OHD levels; 653 participants (47%) had a level less than 30 ng/mL and 180 participants (13%) had a level less than 20 ng/mL (Table 2).
Table 2. Baseline Factors in the Subgroup With Baseline 25-Hydroxy Vitamin D Levels Measured.
| Baseline factor | No. (%) | P value | |
|---|---|---|---|
| Placebo | Vitamin D | ||
| No. | 698 | 699 | |
| Age, y | |||
| 50-64 | 235 (34) | 252 (36) | .27 |
| 65-74 | 398 (57) | 370 (53) | |
| ≥75 | 65 (9) | 77 (11) | |
| Sex | |||
| Male | 377 (54) | 345 (49) | .08 |
| Female | 321 (46) | 354 (51) | |
| Race and ethnicitya | |||
| White (Non-Hispanic) | 514 (76) | 516 (77) | .57 |
| African-American | 103 (15) | 111 (17) | |
| Hispanic | 35 (5) | 23 (3) | |
| Asian/Pacific Islander | 12 (2) | 14 (2) | |
| Otherb or unknown | 8 (1) | 8 (1) | |
| BMI | |||
| <25 | 207 (30) | 199 (29) | .87 |
| 25 to <30 | 269 (39) | 267 (39) | |
| ≥30 | 207 (30) | 214 (31) | |
| Exercise, MET-h/wk | |||
| <6.7 | 202 (30) | 214 (32) | .63 |
| 6.7-24.92 | 242 (36) | 226 (33) | |
| ≥24.93 | 236 (35) | 239 (35) | |
| Education | |||
| <High school | 7 (1) | 8 (1) | .36 |
| High school graduate | 77 (11) | 65 (9) | |
| College | 261 (38) | 292 (42) | |
| Post-college | 350 (50) | 334 (48) | |
| Hypertension | |||
| Absent | 323 (46) | 320 (46) | .83 |
| Present | 372 (54) | 377 (54) | |
| Diabetes | |||
| Absent | 596 (85) | 586 (84) | .50 |
| Present | 102 (15) | 111 (16) | |
| Smoking | |||
| Never | 342 (50) | 359 (53) | .37 |
| Past | 284 (42) | 258 (38) | |
| Current | 52 (8) | 58 (9) | |
| Alcohol use | |||
| None | 198 (29) | 216 (31) | .12 |
| <Daily | 289 (42) | 307 (44) | |
| ≥Daily | 200 (29) | 167 (24) | |
| Statins initiatedc | |||
| Atorvastatin | 351 (50) | 343 (49) | .98 |
| Simvastatin | 153 (22) | 152 (22) | |
| Pravastatin | 96 (14) | 102 (15) | |
| Rosuvastatin | 47 (7) | 50 (7) | |
| Other | 51 (7) | 52 (7) | |
| Vitamin D levels (pretreatment), ng/mLd | |||
| ≥30 | 375 (54) | 369 (53) | .55 |
| 20-30 | 228 (33) | 245 (35) | |
| <20 | 95 (14) | 85 (12) | |
| Mean (SD) | 30.4 (9.6) | 30.4 (9.7) | |
| Median (IQR) | 30.0 (24.1-36.9) | 30.0 (24.0-36.9) | |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); MET-h; metabolic equivalents per hour.
Race and ethnicity were self-reported.
Includes American Indian and Alaska Native.
Total more than 100% due to use of more than 1 statin by some anticipated.
To convert to nmol, multiply by 2.496.
The frequency of muscle symptoms did not differ by treatment assignment among the participants with measured 25-OHD levels occurring in 194 of 699 vitamin D–assigned participants (28%) and in 214 of 698 placebo-assigned participants (31%) (Figure 3). The affect of vitamin D with muscle symptoms was similar across baseline 25-OHD levels (Figure 3). The ORs for the association with vitamin D on SAMS were 0.86 (95% CI, 0.69-1.09) in all participants with 25-OHD levels measured, 0.87 (95% CI, 0.64-1.19) in participants with levels 30 ng/mL or more, 0.85 (95% CI, 0.56-1.28) with levels 20 to 30 ng/mL, and 0.93 (95% CI, 0.50-1.74) with levels less than 20 ng/mL. The test for treatment effect modification by baseline serum 25-OHD level was not significant (interaction P value = .83).
Figure 3. Statin-Associated Muscle Symptoms (SAMS) in Participants With 25-OHD Levels Measured Prior to Randomization.
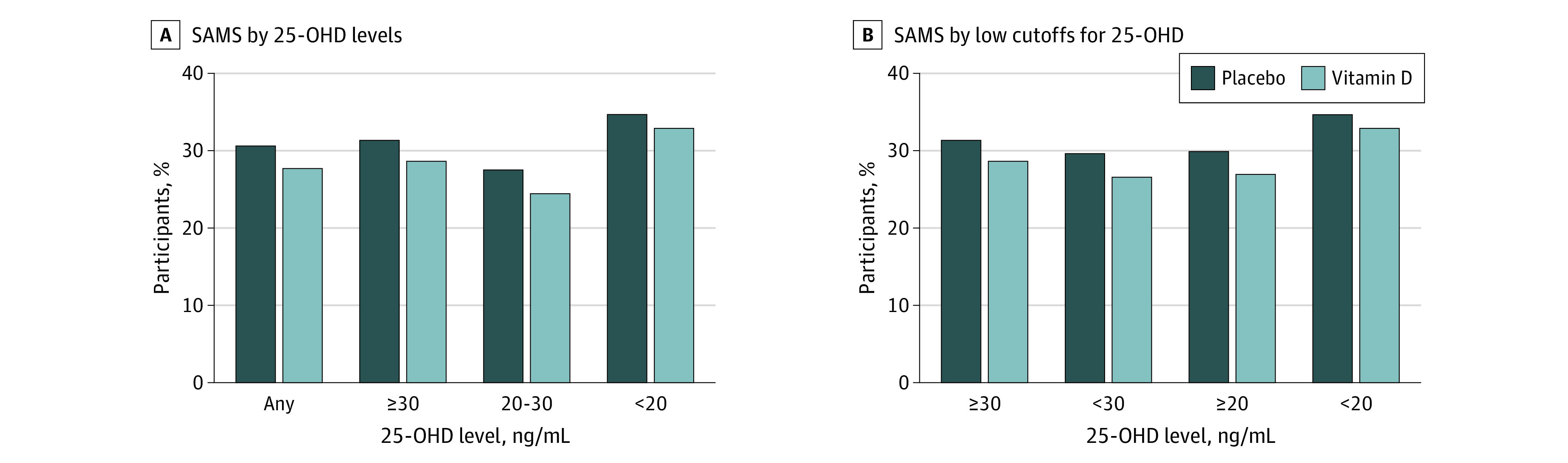
SI conversion factor: To convert to nmol, multiply by 2.496.
The frequency of SAMS are shown for placebo-assigned and vitamin–D assigned participants. A, Data are displayed from left to right, from all 1397 participants with 25-OHD levels measured (far left), then from the 744 participants with levels 30 ng/mL or more (middle left), then from the 473 participants with levels 20 to 30 ng/mL (middle right), and finally from the 180 participants with levels less than 20 ng/mL (far right). B, Data from the 744 participants with levels 30 ng/mL or more are compared with the 653 participants with levels less than 30 ng/mL on the left side and data from the 1217 participants with levels 20 ng/mL or more are compared with the 180 participants with levels less than 20 ng/mL on the right side.
Results were similar when applying different cut points to define low 25-OHD levels (Figure 3). With 25-OHD levels less than 30 ng/mL, SAMS were reported by 88 of 330 participants taking vitamin D (27%) and 96 of 323 participants taking placebo (30%). With 25-OHD levels less than 20 ng/mL, SAMS were reported by 28 of 85 participants taking vitamin D (33%) and 33 of 95 participants taking placebo (35%) (Figure 3).
Discussion
This study took advantage of the large double-blind, placebo-controlled VITAL trial,14 which randomized patients to vitamin D supplementation for primary prevention of cardiovascular disease and cancer to test whether vitamin D was associated with a reduction in SAMS among new statin users. It was not: we found essentially the same frequency of SAMS among the 1033 participants randomized to vitamin D as among the 1050 randomized to placebo and no difference in the frequency of statin discontinuation due to SAMS (Figure 2). These null results in a large, contemporary randomized clinical trial suggest that vitamin D has little, if any, association with preventing SAMS.
While VITAL randomized participants to blinded vitamin D supplementation or placebo, participants initiated statin therapy after randomization, which could have introduced differences between the treatment groups. Baseline characteristics were, however, well balanced between the treatment groups and we adjusted for characteristics previously shown to be associated with SAMS16 or that were imbalanced at baseline. The narrow 95% CIs on the adjusted ORs suggest a clinically important treatment effect from vitamin D on SAMS is unlikely.
Several observational studies of vitamin D treatment of SAMS have been performed,8,9,10,11,12,13 but we are unaware of any reports from randomized trials designed to test prospectively the effect of vitamin D on SAMS. Another randomized trial of vitamin D for prevention of cardiovascular disease, the Vitamin D Assessment (ViDA) study, assessed the effect of vitamin D on adherence to statins.17 ViDA randomized participants aged 50 to 84 years to receive monthly oral capsules containing either 100 000 international units of cholecalciferol or placebo. Among the 5110 randomized participants, 2494 had 2 or more statin prescriptions and were treated for at least 90 days. At 24 months after the initial statin prescription, there was no difference in statin adherence (defined as 80% or more proportion of days covered), with 79% of vitamin D–assigned participants adherent compared with 78% of placebo-assigned patients (risk ratio, 1.01; 95% CI, 0.97-1.05; P = .62). They did report that slightly more vitamin D–assigned participants (60%) than placebo-assigned participants (hazard ratio, 1.15; 95% CI, 1.02-1.30; P = .02) had uninterrupted statin therapy (ie, no gap of more than 30 days). The ViDA study, however, excluded participants who did not renew their initial statin prescription (55 participants assigned to vitamin D; 45 participants assigned to placebo) and participants who stopped taking a statin within 90 days (6 in each group), who may have stopped treatment due to SAMS. The ViDA study did not assess SAMS.
Serum 25-OHD Levels and SAMS
Vitamin D might be more effective for individuals with reduced vitamin D levels. The lower limit for normal 25-OHD levels has been controversial, however, with different expert groups suggesting levels of 20 ng/mL or 30 ng/mL.18,19,20 Two-thirds of VITAL participants had baseline 25-OHD levels measured: 47% had levels less than 30 ng/mL and 13% had levels less than 20 ng/mL. The prior observational studies of vitamin D to treat SAMS enrolled patients with levels less than 30 ng/mL or less than 32 ng/mL.9,10,11,12,13 We found no evidence that vitamin D was any more effective in the participants with lower pretreatment 25-OHD levels based on either definition of a low level (Figure 3). This finding reinforces the overall conclusion that there was no clinically important effect of vitamin D in preventing SAMS.
Frequency of Muscle Symptoms on Statins
Muscle pain is common in the general population, so it is not surprising that these symptoms are also common among patients treated with statins. In the National Health and Nutrition Examination Survey, 22% of statin users reported musculoskeletal pain within the prior 30 days, significantly more than the 17% of respondents who did not use a statin.2 Observational studies have reported widely varying rates of muscle symptoms among statin users, ranging from 10% to 44%,1,2,3,4,5,6 and these rates have also varied widely in double-blind, placebo-controlled randomized trials of statins.21 A recent individual participant data meta-analysis of 19 trials with 123 940 participants21 found muscle symptoms in 27% of participants assigned to statins over 4.3 years of follow-up, which is very similar to the 31% with muscle symptoms over 4.8 years of follow-up we found in the VITAL trial. This meta-analysis documented a significant increase in muscle symptoms among statin-assigned participants, with a relative risk of 1.07 (95% CI, 1.04-1.10) in the first year of treatment. Importantly, in VITAL, we found no difference in the rate of muscle symptoms among new statin users randomly assigned to vitamin D or placebo.
Placebo and Nocebo Effects
Participants in VITAL were blinded to vitamin D supplementation but they were not blinded to prescription of a statin by their personal physicians, which may have affected our findings. The previously reported beneficial effects of vitamin D on SAMS and statin tolerance in unblinded studies may have been due to a placebo effect: individuals were prescribed vitamin D specifically to improve statin tolerance and their anticipation of a benefit from vitamin D may have led to the reported effects. Nonspecific muscle symptoms that occur while taking a statin, especially those due to a nocebo effect,22,23,24 may be particularly responsive to any placebo effect from a physician’s recommendation to take vitamin D to reduce SAMS. Since participants in VITAL were unaware whether they were taking vitamin D or placebo, they were not expecting any beneficial effect from vitamin D on SAMS and any reduction in SAMS due to a placebo effect from vitamin D would not have been evident in this study.
Strengths and Limitations
The strengths of this study are its large size (2083 participants), the blinded and randomized assignment to vitamin D or placebo, and the high response rate (88%) to the survey about SAMS. Nevertheless, this study has several limitations, most notably that statin therapy was initiated after randomization by the participants’ personal physicians and that SAMS were not evaluated or treated prospectively. The survey nonresponders had higher levels of cardiac risk factors than the responders, but the nonresponse rate was very low (12%). We do not have data on the duration or dose of statin therapy before onset of SAMS, or information about any measures taken to manage SAMS or reinstitute statin therapy. However, these variables would be expected to have been balanced between randomized groups. By design, we tested whether vitamin D would reduce the frequency of SAMS and did not evaluate any potential role of vitamin D in managing SAMS, improving adherence to statin therapy, or reducing low-density lipoprotein cholesterol levels. Even though 47% of participants had 25-OHD levels less than 30 ng/mL, only 13% had levels less than 20 mg/mL, so the 95% CIs on the association of vitamin D with SAMS in this subgroup were broad. We cannot exclude an effect of vitamin D in treating patients who have well-documented intolerance to multiple statins, especially after recommended adjustments of the type and dose of statin, which could be tested in well-designed double-blind randomized trials.25 Despite these limitations, this study provides a unique and rigorous test of the hypothesis that routine vitamin D supplementation would prevent the development of SAMS.
Conclusions
Participants in the VITAL study who initiated statin therapy had a similar, high frequency of SAMS whether they were randomized to vitamin D or to placebo. This suggests that vitamin D lacks a clinically important effect in preventing SAMS.
eTable. Baseline factors of survey nonresponders and responders
eAppendix. Wording of survey about experience with statins
Data sharing statement.
References
- 1.Bruckert E, Hayem G, Dejager S, Yau C, Bégaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients–the PRIMO study. Cardiovasc Drugs Ther. 2005;19(6):403-414. doi: 10.1007/s10557-005-5686-z [DOI] [PubMed] [Google Scholar]
- 2.Buettner C, Rippberger MJ, Smith JK, Leveille SG, Davis RB, Mittleman MA. Statin use and musculoskeletal pain among adults with and without arthritis. Am J Med. 2012;125(2):176-182. doi: 10.1016/j.amjmed.2011.08.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cohen JD, Brinton EA, Ito MK, Jacobson TA. Understanding Statin Use in America and Gaps in Patient Education (USAGE): an internet-based survey of 10,138 current and former statin users. J Clin Lipidol. 2012;6(3):208-215. doi: 10.1016/j.jacl.2012.03.003 [DOI] [PubMed] [Google Scholar]
- 4.Lin I, Sung J, Sanchez RJ, et al. Patterns of statin use in a real-world population of patients at high cardiovascular risk. J Manag Care Spec Pharm. 2016;22(6):685-698. doi: 10.18553/jmcp.2016.22.6.685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Navar AM, Peterson ED, Li S, et al. Prevalence and management of symptoms associated with statin therapy in community practice: Insights from the PALM (Patient and Provider Assessment of Lipid Management) registry. Circ Cardiovasc Qual Outcomes. 2018;11(3):e004249. doi: 10.1161/CIRCOUTCOMES.117.004249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zhang H, Plutzky J, Skentzos S, et al. Discontinuation of statins in routine care settings: a cohort study. Ann Intern Med. 2013;158(7):526-534. doi: 10.7326/0003-4819-158-7-201304020-00004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Michalska-Kasiczak M, Sahebkar A, Mikhailidis DP, et al. ; Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group . Analysis of vitamin D levels in patients with and without statin-associated myalgia—a systematic review and meta-analysis of 7 studies with 2420 patients. Int J Cardiol. 2015;178:111-116. doi: 10.1016/j.ijcard.2014.10.118 [DOI] [PubMed] [Google Scholar]
- 8.Bartlomiejczyk MA, Penson P, Banach M. Vitamin D and SAMS. In: Thompson PD, Taylor BA, eds. Statin-associated muscle symptoms. Humana Press; 2020:121-128. doi: 10.1007/978-3-030-33304-1_14 [DOI] [Google Scholar]
- 9.Reston JT, Buelt A, Donahue MP, Neubauer B, Vagichev E, McShea K. Interventions to improve statin tolerance and adherence in patients at risk for cardiovascular disease: a systematic review for the 2020 U.S. Department of Veterans Affairs and U.S. Department of Defense Guidelines for management of dyslipidemia. Ann Intern Med. 2020;173(10):806-812. doi: 10.7326/M20-4680 [DOI] [PubMed] [Google Scholar]
- 10.Khayznikov M, Hemachrandra K, Pandit R, Kumar A, Wang P, Glueck CJ. Statin intolerance because of myalgia, myositis, myopathy, or myonecrosis can in most cases be safely resolved by vitamin D supplementation. N Am J Med Sci. 2015;7(3):86-93. doi: 10.4103/1947-2714.153919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kang JH, Nguyen QN, Mutka J, Le QA. Rechallenging statin therapy in veterans with statin-induced myopathy post vitamin D replenishment. J Pharm Pract. 2017;30(5):521-527. doi: 10.1177/0897190016674407 [DOI] [PubMed] [Google Scholar]
- 12.Glueck CJ, Budhani SB, Masineni SS, et al. Vitamin D deficiency, myositis-myalgia, and reversible statin intolerance. Curr Med Res Opin. 2011;27(9):1683-1690. doi: 10.1185/03007995.2011.598144 [DOI] [PubMed] [Google Scholar]
- 13.Ahmed W, Khan N, Glueck CJ, et al. Low serum 25 (OH) vitamin D levels (<32 ng/mL) are associated with reversible myositis-myalgia in statin-treated patients. Transl Res. 2009;153(1):11-16. doi: 10.1016/j.trsl.2008.11.002 [DOI] [PubMed] [Google Scholar]
- 14.Manson JE, Cook NR, Lee IM, et al. ; VITAL Research Group . Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380(1):33-44. doi: 10.1056/NEJMoa1809944 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Luttmann-Gibson H, Mora S, Camargo CA, et al. Serum 25-hydroxyvitamin D in the VITamin D and OmegA-3 TriaL (VITAL): clinical and demographic characteristics associated with baseline and change with randomized vitamin D treatment. Contemp Clin Trials. 2019;87:105854. doi: 10.1016/j.cct.2019.105854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gonzalez PE, Hlatky MA, Manson JE, et al. Statin-associated muscle symptoms in the VITamin D and OmegA-3 triaL (VITAL). Am Heart J. 2022;252:39-41. doi: 10.1016/j.ahj.2022.06.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wu Z, Camargo CA Jr, Khaw KT, et al. Effects of vitamin D supplementation on adherence to and persistence with long-term statin therapy: secondary analysis from the randomized, double-blind, placebo-controlled ViDA study. Atherosclerosis. 2018;273:59-66. doi: 10.1016/j.atherosclerosis.2018.04.009 [DOI] [PubMed] [Google Scholar]
- 18.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-281. doi: 10.1056/NEJMra070553 [DOI] [PubMed] [Google Scholar]
- 19.Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53-58. doi: 10.1210/jc.2010-2704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911-1930. Medline: doi: 10.1210/jc.2011-0385 [DOI] [PubMed] [Google Scholar]
- 21.Cholesterol Treatment Trialists’ Collaboration . Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022;400(10355):832-845. doi: 10.1016/S0140-6736(22)01545-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Colloca L, Barsky AJ. Placebo and nocebo effects. N Engl J Med. 2020;382(6):554-561. doi: 10.1056/NEJMra1907805 [DOI] [PubMed] [Google Scholar]
- 23.Tobert JA, Newman CB. The nocebo effect in the context of statin intolerance. J Clin Lipidol. 2016;10(4):739-747. doi: 10.1016/j.jacl.2016.05.002 [DOI] [PubMed] [Google Scholar]
- 24.Gupta A, Thompson D, Whitehouse A, et al. ; ASCOT Investigators . Adverse events associated with unblinded, but not with blinded, statin therapy in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid-Lowering Arm (ASCOT-LLA): a randomised double-blind placebo-controlled trial and its non-randomised non-blind extension phase. Lancet. 2017;389(10088):2473-2481. doi: 10.1016/S0140-6736(17)31075-9 [DOI] [PubMed] [Google Scholar]
- 25.Taylor BA, Lorson L, White CM, Thompson PD. A randomized trial of coenzyme Q10 in patients with confirmed statin myopathy. Atherosclerosis. 2015;238(2):329-335. doi: 10.1016/j.atherosclerosis.2014.12.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable. Baseline factors of survey nonresponders and responders
eAppendix. Wording of survey about experience with statins
Data sharing statement.