

Abstract
Background
Previous studies have linked environmental exposures with anti-Müllerian hormone (AMH), a marker of ovarian reserve. However, associations with multiple environment factors has to our knowledge not been addressed.
Methods
We included a total of 2,447 premenopausal women in the Nurses’ Health Study II (NHSII) who provided blood samples during 1996–1999. We selected environmental exposures linked previously with reproductive outcomes that had measurement data available in NHSII, including greenness, particulate matter, noise, outdoor light at night, ultraviolet radiation, and six hazardous air pollutants (1,3-butadiene, benzene, diesel particulate matter, formaldehyde, methylene chloride, and tetrachloroethylene). For these we calculated cumulative averages from enrollment (1989) to blood draw and estimated associations with AMH in adjusted single exposure models, principal component analysis (PCA), and hierarchical Bayesian kernel machine regression (BKMR).
Results
Single exposure models showed negative associations of AMH with benzene (percentage reduction in AMH per interquartile range (IQR) increase = 5.5%, 95%CI=1.0, 9.8) and formaldehyde (6.1%, 95%CI=1.6, 10). PCA identified four major exposure patterns but only one with high exposure to air pollutants and light at night was associated with lower AMH. Hierarchical BKMR pointed to benzene, formaldehyde, and greenness, and suggested an inverse joint association with AMH (percentage reduction comparing all exposures at the 75th percentile to median= 8.2%, 95%CI=0.7, 15.1. Observed associations were mainly among women above age 40.
Conclusions
We found exposure to benzene and formaldehyde to be consistently associated with lower AMH levels. The associations among older women are consistent with the hypothesis that environmental exposures accelerate reproductive aging.
Keywords: mixture, hazardous air pollutants, benzene, formaldehyde, anti-Müllerian hormone, reproductive aging
Introduction
Ovarian aging is characterized by the decline of oocyte quantity and fluctuations of hormones and is associated with cardiovascular, musculoskeletal, and cognitive health 1–3. This process can be accelerated by both genetic and environmental factors, but to date its associations with exposures in the ambient environment have been understudied 1.
Produced by the granulosa cells in follicles, anti-Müllerian hormone (AMH) has been found to be correlated with other markers of ovarian reserve and menopausal age, and thus may be used as a reliable predictor of reproductive aging 4–9. In addition, epidemiologic studies also suggested that women with low AMH had higher risks of cardiovascular and metabolic diseases 10,11. Several environmental factors, including particulate air pollution, traffic, ultraviolet (UV) radiation, and greenspace, have been linked with AMH and age at menopause 12–17. However, these studies only examined the association of single exposure, without considering the complex mixture of exposures that is truly experienced. Additionally, other studies have linked impaired fertility and menstrual disorders, which are common consequences of reproductive aging, with occupational exposure to organic compounds that are also present in the ambient atmosphere 18–22. However, whether exposure to low levels of these compounds in the ambient environment can affect women’s reproductive system remains unclear. Physical environmental factors such as light and noise have been suggested to disrupt neuroendocrine homeostasis, which may adversely affect ovarian function. Furthermore, these factors may share emission source or have correlated geospatial distribution. Thus, co-exposures should be considered. However, few studies have considered the individual and joint effects of exposure to these factors when presenting simultaneously in the environment.
In this study, we aimed to examine the association of exposure to multiple environmental factors with AMH levels among women from a large, prospective US cohort. In addition to investigating the association of each individual exposure, we sought to estimate the overall association of simultaneous exposure to multiple factors and to identify the key exposure(s) that influence the outcome using mixture methods.
Methods
Study population
The Nurses’ Health Study II (NHSII) is an ongoing, prospective, nationwide female cohort with 116,429 registered nurses aged between 25 to 42 when enrolled in 1989. During follow-up, questionnaires have been sent to the participants every two years to collect information on health status and risk factors. Between 1996 and 1999, participants with no history of cancer were asked to provide blood samples for biomarker substudies, which were ultimately received from 29,611 women. At blood collection, participants completed a short questionnaire measuring current weight, smoking, and other factors. Participants were provided with supplies and instructions to return blood samples to the laboratory overnight. Samples were then processed immediately and stored in the vapor phase of liquid nitrogen freezers (−130°C) 23. Informed consent for participating in NHSII and blood sample collection was implied by receipt of completed follow-up questionnaires and blood samples, respectively. The study protocol was approved by the institutional board of Brigham and Women’s Hospital.
Plasma AMH was measured in a subset of these participants as part of five substudies, including three nested case–control studies of breast (N=794) and ovarian cancer (N=44) and early menopause (N=818), one prospective study of age trajectory of AMH (N=800), and one cross-sectional study of differences in AMH by race and ethnicity (N=306) (eFigure 1) 5,24,25. Premenopausal women who were not pregnant or breastfeeding and had not used oral contraceptives or exogenous hormones in the past six months before blood collection were eligible for all these substudies. We summarized inclusion criteria and matching factors by substudy in eTable 1. To reduce the possible impact of hormone-related cancer or menopause on AMH, we excluded women who reported breast, ovarian, or endometrial cancer or natural menopause within 2 years after blood collection. For women who were selected as controls for more than one study (N=44), we randomly selected one AMH measure.
Outcome measurement
Plasma AMH levels were assayed using the picoAMH enzyme-link immunosorbent assay (Ansh Labs, Webster, TX) at Massachusetts General Hospital (for the case–control study of ovarian cancer and the cross-sectional study), Boston Children’s Hospital (for the case–control study of early menopause and the prospective study), and Ansh Labs (for the case–control study of breast cancer), separately. All samples were analyzed in random order. Coefficients of variation in quality control samples from a blinded plasma pool ranged between 0.6–14.5% in all assays. For samples below the limit of detection (N=4 with detection limit of 0.0023 ng/mL and N=1 with detection limit of 0.05 ng/mL), we assigned values of half the detection limit by assay.
Exposure Assessment
We considered exposure to surrounding greenness, particulate matter (PM), noise, outdoor light at night, UV, and air toxins and collected measures of these exposures at residential addresses of each participant. Details of exposure assessment is described in eAppendix.
Briefly, we measured greenness using the Normalized Difference Vegetation Index (NDVI), which ranges from −1 to 1, from the Advanced Very High Resolution Radiometer with a 1 km resolution 26. We used NDVI in July of each year to achieve the largest contrast and set negative values to 0 (indicating no green vegetation), based on recommendations in the current literature 27. PM exposure was calculated as the annual averages of PM2.5–10 and PM2.5 measured at residential address from a geospatial prediction model 28. We estimated noise exposure from a geospatial model that provides time-integrated estimates over 2000–2014 for median anthropogenic noise measures (L50) in daytime (7AM-7PM) and nighttime (7PM-7AM), respectively, at a 270m resolution 29. We measured outdoor light at night by the annual average nighttime visible and near-infrared radiance (at ~1km resolution) from the earth surface using the satellite image data obtained from the US Defense Meteorological Satellite Program’s Operational Linescan System (DMSP-OLS) 30. We calculated solar UV radiation exposure using the average July noontime erythemal UV collected from National Aeronautics and Space Administration satellite UV data and downscaled to ~1 km resolution 31. We obtained exposure to hazardous air pollutants from the 1999 US Environment Protection Agency’s National Air Toxics Assessment (NATA) project. We selected pollutants that have been suggested to be mammary carcinogens or estrogenic disruptors or to have reproductive toxicity, and excluded those with more than 25% zero values among the participants as suggested in previous studies 32–34. To further ensure temporal comparability between the 1996 and 1999 and/or the 1999 and 2002 NATA assessment at the same location, we included toxics with high correlations, defined by the commonly used cutoff as Spearman correlation coefficients greater than 0.70 35,36. We included a total of six hazardous air pollutants (1,3-butadiene, benzene, diesel PM, formaldehyde, methylene chloride, and tetrachloroethylene).
For all exposures, we calculated the cumulative average from 1989 to the nearest questionnaire year prior to blood collection to represent long-term exposure in adulthood, approximately covering exposures across the early 30s to 40s among our participants.
Covariates
We selected covariates a priori that were potential confounders or predictors of AMH or ovarian reserve by subject matter knowledge and data availability in NHSII (eFigure 2), including age (in months and in a cubic spline with 3 degrees of freedom), body mass index (BMI, kg/m2), smoking status (never, past, and current smokers) and parity (nulliparous and parous) collected at blood draw, race and ethnicity (white, black, and others) measured at baseline, history of oral contraceptive use (never and ever) and breastfeeding (nulliparous or for less than 1 month, 1–12 months, and more than 12 months), and questionnaire cycle of blood collection (1995, 1997, and 1999). Information was limited for indiviudal socioeconomic status (SES) in NHSII, including the highest education level of the spouse in 1997 and pre-tax household income collected in 2001. We considered these two variables and the 2000 Census tract median household income to represent participant SES in the model. We included a categorical variable of batch, which corresponded to each substudy, to account for between-assay differences across substudies.
Statistical analysis
We merged data from all substudies into one dataset for statistical analysis. We chose to do so because the participants were selected from the same cohort and all exposures and covariables were measured in the same way. Therefore, heterogeneity across substudies was limited. In addition, analyzing data within each substudy and then pooling the results would greatly increase the uncertainty of estimates from our mixture analyses due to smaller sample sizes. To avoid impacts of extreme values in the exposure, we calculated the Mahalanobis distance across all exposure measures. We have applied this measure to identify extreme values in multi-dimensional data and considers the correlations of all variables in the matrix. We excluded participants whose Mahalanobis distance values above or below three standard deviations (SDs) from the mean. We used three SDs as the cutoff because our preliminary inspection suggested this cutoff can eliminate possible extremes while keeping sufficient variations in exposures. Pair-wise Spearman correlation coefficients were then calculated across the exposures. Because statistical models for mixture analyses can be unstable and difficult to interpret, we employed different statistical modeling approaches to examine the association of plasma AMH with the exposures, as described below.
We first used multivariable single-exposure linear models to examine the associations of each individual exposure with AMH, adjusting for age, race and ethnicity, parity, BMI, smoking status, spouse education, pre-tax household income, Census tract median household income, and batch. To further account for possible confounding between exposures, we also fitted a multi-exposure model with all exposure measures included simultaneously.
Next, to address the strong correlation between exposures, we used principal component analysis (PCA) to explore patterns of exposure among the participants. Components from PCA were independent linear combinations of the exposures. The component loadings indicated the exposures’ contribution and the component scores quantified the participants’ levels of exposure to each component. To examine the association of different exposure patterns (represented by components) with AMH, we fitted a linear model with all component scores included, adjusted for all potential confounders.
Finally, we used Bayesian Kernel Machine Regression (BKMR) to identify key individual exposures, to detect potential non-linear exposure–response relationships and effect modification between exposures, and to estimate the joint association of all exposures with AMH 37,38. BKMR uses a flexible kernel function to model the joint and individual association of the exposure and the outcome in a Bayesian regression model. For better model efficiency, we applied a variant of BKMR that performs hierarchical variable selection, by first selecting a group of exposures for inclusion and then individual exposure within the group. Exposure groupings are pre-specified and were performed based on the PCA results, the correlation structure across the exposures, and subject matter knowledge. We also applied the Gaussian predictive process approach to improve computational efficiency. This approach uses a set of knots covering the exposure space in BKMR and compute the projection of each vector of exposures onto a lower dimensional space. Therefore, instead of inverting a matrix with dimension equals to the number of observations, BKMR only needs to invert a smaller matrix with dimension of the number of knots in the algorithm 37. We assessed relative importance of the exposure by the posterior inclusion probabilities and computed the corresponding exposure–response curve by fixing all other exposures at the median.
Secondary analysis
Considering AMH declines faster in older age and exposure characteristics may differ by urban and rural areas, we examined possible effect modification by age (above and below age 40 at blood collection) and urban versus rural area (2000 Census tract population density above or below 1000 people/km2) by adding interaction terms in the linear models and fitting separate BKMR models. We also conducted sensitivity analyses that additionally adjusted for history of oral contraceptive use and breastfeeding, and questionnaire cycle of blood collection in the models. To assess the potential impact of perimenopause and hormone-related cancers on AMH, we repeated the analysis excluding women who reported natural menopause or breast, ovarian, or endometrial cancer in the 5 years after blood collection. Women with polycystic ovary syndrome (PCOS) can have higher AMH levels, therefore, we repeated the analysis after excluding women who reported irregular menstrual cycles in adulthood as a proxy of PCOS, due to a lack of valid PCOS diagnosis data in NHSII. To examine for possible influence of remaining extreme values in exposure, we further excluded participants whose Mahalanobis distance were above 1 and 2 SDs from the mean and those whose exposure levels were above or below 6 standard deviations from their means, respectively.
We log-transformed plasma AMH to improve normality of residuals. We transformed all exposures to z scores for PCA and BKMR. Estimates from the linear models are presented as the percentage change and 95% confidence intervals (CIs) of AMH with an interquartile range (IQR) increase of the exposure or with 1 SD increase in the component score. For BKMR, we used the group posterior inclusion probabilities and the conditional probabilities for each exposure in the group to determine importance of the exposures. The joint association of the exposures was estimated by fixing all exposures at the 75th percentile relative to the median. To aid in interpretation, we determined the change in AMH with age. All analysis were conducted in SAS 9.4 (SAS Institute, Cary, NC) and R (version 3.6.3) (R Foundation for Statistical Computing, Vienna, Austria).
Results
Descriptions
Major demographic, lifestyle, and socioeconomic characteristics, and all environmental exposures were comparable among women who provided blood samples and the entire NHSII cohort (eTable 2). We assayed blood samples from 2,714 women for plasma AMH. Among them, we excluded 211 women who reported menopause or cancer before or in the 2 years after blood collection and 64 women who used oral contraceptives or hormones near blood collection. We also excluded three women with missing smoking status, one woman with missing exposures, and 13 women with extreme values in the exposure profile as determined by Mahalanobis distance. A total of 2,447 women were included in analyses.
Characteristics of the included participants are summarized in Table 1 and eTable 3. Briefly, the mean age at blood collection was 39.8 years and the mean plasma AMH level was 2.3 ng/mL. Most participants were white (90.2%). The average duration of exposure measurement (from cohort enrollment to the nearest questionnaire year prior to blood collection) was 7.1 years. We found moderate to high correlations within noise and light at night (Spearman correlation coefficients=0.66–0.85) and within hazardous air pollutants (Spearman correlation coefficients=0.59–0.90), and between these two clusters (Figure 1). NDVI was negatively correlated with all other exposures. For comparison to the environmental results, a 1 month increase in age was associated with a 0.91% (95%CI=0.80, 1.0) lower AMH in our participants, and this association was stronger among women older than 40 (percentage reduction=1.5%, 95%CI=1.3, 1.8) than in younger women (percentage reduction =0.25%, 95%CI=−0.04, 0.54).
Table 1.
Participant characteristics at time of blood collection among 2,447 women in the Nurses’ Health Study II and by substudies a
| mean ± SD or % | |
|---|---|
|
| |
| N | 2,447 |
| Age at blood collection, y (mean±SD) | 40±4.0 |
| Plasma AMH (ng/mL, mean±SD) b | 2.3±2.6 |
| Smoking status, % | |
| Never smoked | 72 |
| Ever smoked | 21 |
| Currently smoke | 7 |
| Body mass index, kg/m2 (mean±SD) | 25±5.2 |
| Race/ethnicity, % | |
| White | 90 |
| Black | 4 |
| Others | 6 |
| Parity, % | |
| Nulliparous | 19 |
| Parous | 81 |
| History of oral contraceptive use,% | |
| Never used | 19 |
| Ever used | 81 |
| History of breastfeeding, % Nulliparous or breastfed < 1 month | 29 |
| 1–12 months | 26 |
| >12 months | 45 |
| Census tract median income, $1,000 (mean±SD) | 65±24 |
| Census tract population density, 1000 people per km2 (mean±SD) | 3.8±11 |
| Spouse education level, % | |
| High school or less | 17 |
| Some college | 44 |
| Graduate school | 28 |
| Missing | 10 |
| Household pre-tax income, % | |
| < $50,000 | 12 |
| $50,000 – $74,999 | 23 |
| $75,000 – $99,999 | 19 |
| ≥$100,000 | 30 |
| Missing | 16 |
| Environmental exposures, (mean±SD) c | |
| NDVI | 0.5±0.1 |
| PM10–2.5 (μg/m3) | 11±4.6 |
| PM2.5 (μg/m3) | 15±3.0 |
| Daytime L50 (dB) | 46±4.0 |
| Nighttime L50 (dB) | 43±3.2 |
| LAN (nW/cm2/sr) | 31±28 |
| UV (nW/m2) | 189±27 |
| 1,3-Butadiene (μg/m3) | 0.1±0.1 |
| Benzene (μg/m3) | 1.3±0.7 |
| Diesel PM (μg/m3) | 1.1±0.9 |
| Formaldehyde (μg/m3) | 1.5±0.8 |
| Methylene chloride (μg/m3) | 0.6±0.5 |
| Tetrachloroethylene (μg/m3) | 0.3±0.4 |
Abbreviations: SD, standard deviation; AMH, anti-Müllerian hormone; NDVI, normalized difference vegetation index; PM10–2.5, particulate matter with an aerodynamic diameters between 10 to 2.5 microns; PM2.5, particulate matter with an aerodynamic diameters less than or equal to 2.5 microns; L50, median anthropogenic noise; LAN, light at night; UV, ultraviolet radiation.
All values were age-standardized except for age at blood collection and plasma AMH levels. Values were mean±SD for continuous variables and percentages for categorical variables.
Calibrated across different batches.
Calculated as cumulative average from 1989 to the year of blood collection.
Figure 1. Spearman correlation coefficients among measures of surrounding greenness, particulate air pollution, noise, LAN, UV, and HAPs.
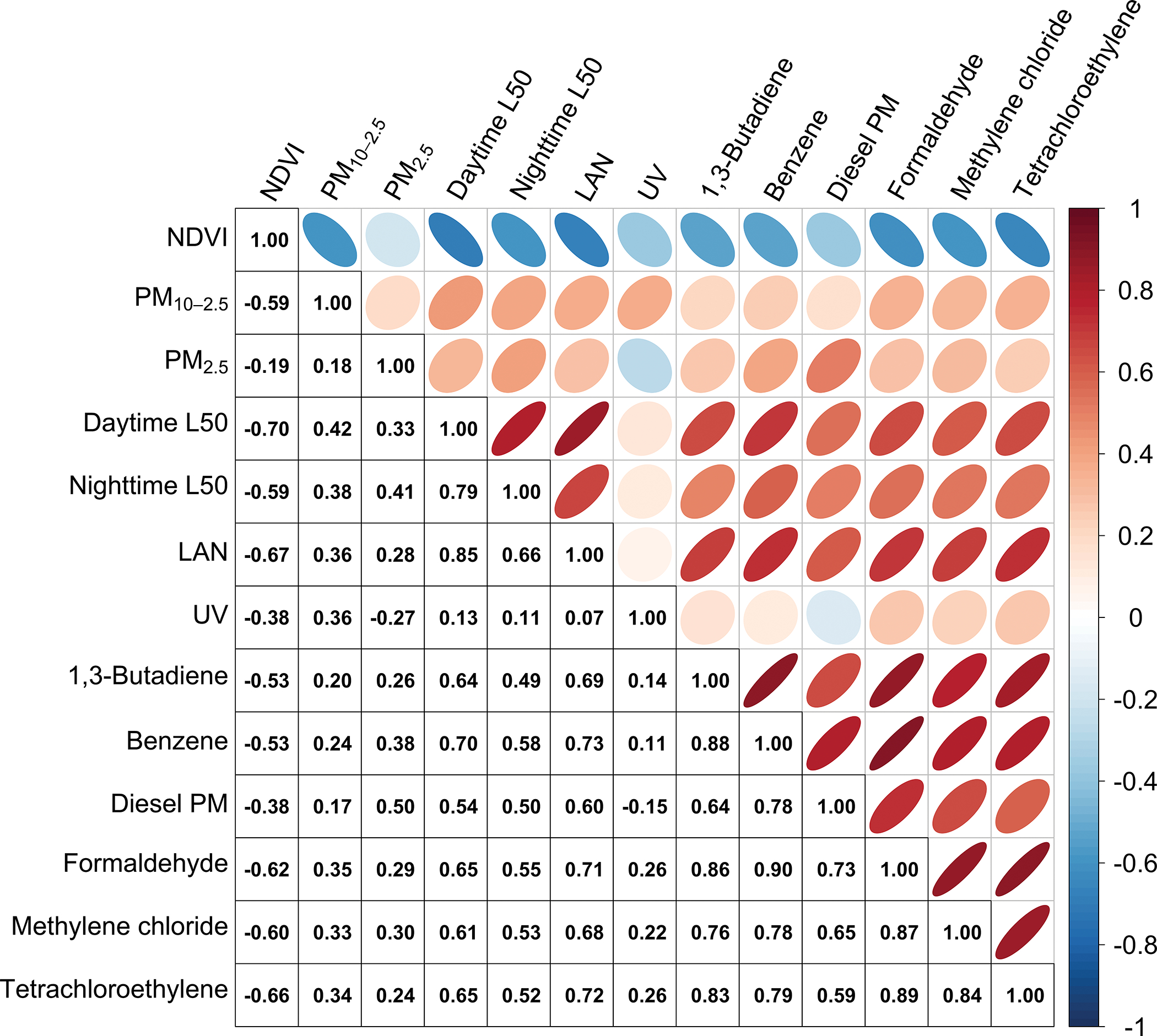
The shade of each ellipse on the upper panel indicates the absolute value of the correlation coefficient. When an ellipse is leaning towards the left, this suggests the correlation between two variables are negative; when an ellipse is leaning towards the right, this suggests the correlation between two variables are positive.
Abbreviations: NDVI, normalized difference vegetation index; PM10–2.5, particulate matter with an aerodynamic diameters between 10 to 2.5 microns; PM2.5, particulate matter with an aerodynamic diameters less than or equal to 2.5 microns; L50, median anthropogenic noise; LAN, light at night; UV, ultraviolet radiation; HAPs, hazardous air pollutants.
Single and multi-exposure models
After adjusting for potential confounders, we found that ambient benzene and formaldehyde were associated with lower AMH in single exposure models (Table 2). For example, one interquartile range width (IQRw) in benzene was associated with 5.5% (95%CIs= 1.0, 9.8) lower AMH and, for formaldehyde, with 6.1% (95%CIs=1.6, 10) lower AMH, equivalent to 6.0 and 6.7 months increase of age, respectively. However, we found no associations were found for the other exposures. Compared to single-exposure models, associations in the multi-exposure model often changed direction or magnitude and had inflated 95%CIs.
Table 2.
Percentage change (95% confidence intervals) in AMH with an interquartile range increase of each exposure in single and multi-exposure models
| IQRw | Single exposure a | Multi-exposure a | |
|---|---|---|---|
|
| |||
| NDVI | 0.14 | 2.8 (−3.1, 9.0) | −5.2 (−15, 5.7) |
| PM10–2.5 (μg/m3) | 5.2 | −3.2 (−8.0, 1.8) | −5.6 (−12, 1.6) |
| PM2.5 (μg/m3) | 4.2 | 1.4 (−4.9, 8.1) | 9.6 (0.66, 19) |
| Daytime L50 (dB) | 4.6 | −2.2 (−7.2, 3.0) | −0.90 (−12, 12) |
| Nighttime L50 (dB) | 3.5 | −1.7 (−6.4, 3.3) | −0.8 (−9.8, 9.1) |
| LAN (nW/cm2/sr) | 34 | −2.9 (−8.2, 2.6) | 4.1 (−6.0, 15) |
| UV (nW/m2) | 33 | −1.8 (−7.0, 3.6) | 3.4 (−5.3, 12) |
| 1,3-Butadiene (μg/m3) | 0.10 | −2.4 (−5.5, 0.92) | 0.95 (−4.0, 6.2) |
| Benzene (μg/m3) | 0.67 | −5.5 (−9.8, −1.0) | −1.0 (−14, 14) |
| Diesel PM (μg/m3) | 0.61 | −2.6 (−5.4, 0.33) | −0.85 (−5.4, 3.9) |
| Formaldehyde (μg/m3) | 0.77 | −6.1 (−10, −1.6) | −16 (−27, −2.1) |
| Methylene chloride (μg/m3) | 0.33 | −0.85 (−3.7, 2.1) | 1.7 (−2.0, 5.6) |
| Tetrachloroethylene (μg/m3) | 0.20 | −1.4 (−3.6 0.94) | 2.5 (−2.1, 7.4) |
Abbreviations: AMH, anti-Müllerian hormone; NDVI, normalized difference vegetation index; PM10–2.5, particulate matter with an aerodynamic diameters between 10 to 2.5 microns; PM2.5, particulate matter with an aerodynamic diameters less than or equal to 2.5 microns; L50, median anthropogenic noise; LAN, light at night; UV, ultraviolet radiation; IQRw, interquartile range width.
Adjusting for age (in natural cubic spline with 3 degrees of freedom), body mass index, race/ethnicity, parity, spouse education status, pre-tax household income, Census tract median income, batches, and smoking.
PCA
We selected the first four principal components from PCA, which explained 81.1% of the total variation in the 13 exposure measures. As shown in Figure 2, component 1 had high loadings for light at night and hazardous air pollutants and component 2 had high loadings for PM2.5–10 and UV. Component 3 had high loadings for noise and the last component had a high loading for PM2.5. NDVI had negative loadings for the first three components. The model using component scores showed an inverse association between AMH and component 1 (percentage change of AMH per 1 SD increase of the component score= −4.6%, 95%CIs= −9.0, −0.08), while no associations were found for the other components (percentage changes of AMH = −1.9 to 1.3%) (Table 3).
Figure 2. Component loadings for measures of surrounding greenness, particulate air pollution, noise, LAN, UV, and HAPs.

The direction of the triangles denotes the direction of the loading (upward: positive, downward: negative).
Abbreviations: NDVI, normalized difference vegetation index; PM10–2.5, particulate matter with an aerodynamic diameters between 10 to 2.5 microns; PM2.5, particulate matter with an aerodynamic diameters less than or equal to 2.5 microns; L50, median anthropogenic noise; LAN, light at night; UV, ultraviolet radiation; HAPs, hazardous air pollutants.
Table 3.
Percentage change (95% confidence intervals) in AMH with 1 SD increase of component scores
| High loading exposures | % change (95%CI) a | |
|---|---|---|
|
| ||
| Component 1 | LAN, 1,3-butadeine, benzene, diesel particulate matter, formaldehyde, methylene chloride, and tetrachloroethylene | −4.6 (−9.0, −0.08) |
| Component 2 | NDVI (negative), PM10–2.5, and UV | −1.9 (−6.2, 2.6) |
| Component 3 | Daytime and nighttime L50 | −0.76 (−5.1, 3.8) |
| Component 4 | PM2.5 | 1.3 (−3.1, 5.8) |
Abbreviations: AMH, anti-Müllerian hormone; PC, principle components; NDVI, normalized difference vegetation index; PM10–2.5, particulate matter with an aerodynamic diameters between 10 to 2.5 microns; PM2.5, particulate matter with an aerodynamic diameters less than or equal to 2.5 microns; L50, median anthropogenic noise; LAN, light at night; UV, ultraviolet radiation.
Adjusting for age (in natural cubic spline with 3 degrees of freedom), body mass index, race/ethnicity, parity, spouse education status, pre-tax household income, Census tract median income, batches, smoking, and scores for all other components.
BKMR
Based on results from the single exposure models and PCA, we allowed BKMR to select from the exposures in the first component (i.e., light at night and hazardous air pollutants), as well as NDVI (as it loaded high on the first component) for inclusion. The remaining exposure measures were added as covariates. The results indicated moderate support for inclusion of NDVI and the group of hazardous air pollutants (group posterior inclusion probabilities=0.25 and 0.11, respectively) but not for LAN (group posterior inclusion probability<0.01) (Table S3). Within the group of hazardous air pollutants, formaldehyde had the highest conditional posterior inclusion probability (0.83) followed by benzene (0.16), while the other pollutants were not selected. Greenness showed a non-linear exposure–response relationship with AMH, in which NDVI was positively associated with AMH at lower levels but then the association became negative as NDVI continued to increase (Figure 3A). Formaldehyde and benzene both showed decreasing trends with AMH and the curve was steeper for high levels of formaldehyde (Figure 3A). We observed no obvious effect modification among the exposures. Overall, simultaneous exposure to greenness, light at night, and hazardous air pollutants was inversely associated with AMH (Figure 3B). For example, the AMH level was 8.2% lower (95%CIs= 0.72, 15) when fixing all exposures at the 75th percentile compared to the median, which was equivalent to a 9-month increase in age.
Figure 3. Exposure–response curve for surrounding greenness (NDVI), benzene, and formaldehyde with AMH (A) and overall association (percentage change and 95% credible intervals) of the exposure to environmental factors with AMH (B).
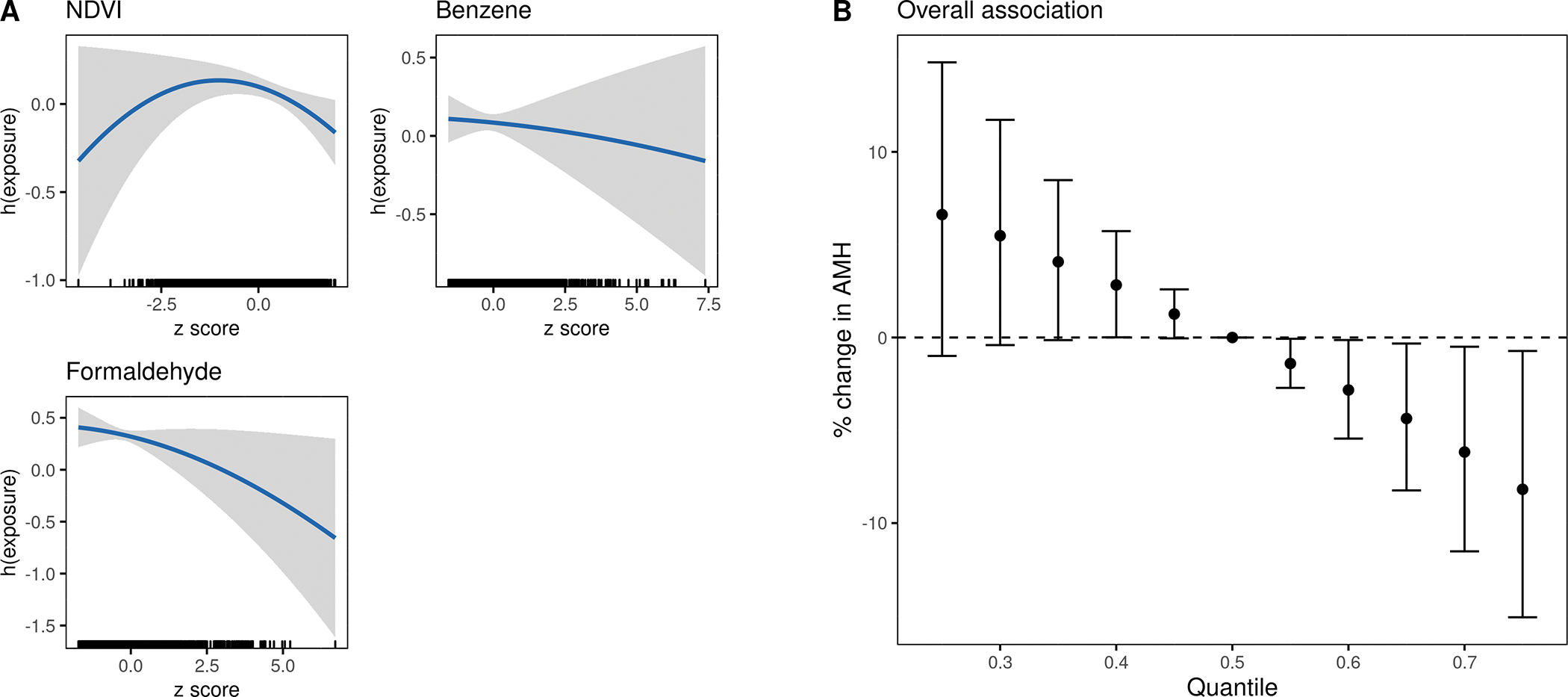
Abbreviations: NDVI, normalized difference vegetation index; AMH, anti-Müllerian hormone.
All exposures in the mixture matrix were standardized. All models were adjusted for age (in natural cubic spline with 3 degrees of freedom), body mass index, race–ethnicity, parity, spouse education status, pre-tax household income, Census tract median income, smoking, and other environmental exposures (PM10–2.5, PM2.5, daytime L50, nighttime L50, and UV).
Overall association was computed by comparing when all exposures are fixed at different quantiles to the median.
Secondary analyses
The observed associations in the full sample were generally only apparent among women older than 40. As shown in Table 4, the single exposure models showed that one IQRw increase of benzene was associated with 8.4% lower AMH (95%CIs=2.4, 14) and, in formaldehyde, 9.8% lower AMH (95%CIs=4.0, 15) among women above 40. 1,3-butadiene was also associated with lower AMH in these women (percentage change per 1 IQRw increase: −5.8%, 95%CIs= −9.9, −1.4). Meanwhile, benzene was associated with a −2.2% (95%CIs=−8.4, 4.3), formaldehyde with −1.9% (95%CIs=−8.0, 4.6), and 1,3-butadiene with1.4% (95%CIs=−3.2, 6.3) changes in AMH, respectively, among those under age 40. Similarly, component 1 was negatively associated with AMH for women above age 40 (percentage change per 1 SD increase in the component score= −9.3%, 95%CI= −15, −3.4) among older women while no associations were found for women under age 40 (0.20%, 95%CIs = −6.1, 7.0).
Table 4.
Percentage change (95% confidence intervals) in AMH for each exposure (per interquartile range width increase) and component (per 1 SD increase) by age at blood collection and by urban/rural area a
| By age | By urban/rural area b | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| < 40 (N=1,207) | ≥ 40 (N=1,242) | p for modification | Urban (N=1,455) | Rural (N=994) | p for modification | |
|
| ||||||
| Single exposures | ||||||
| NDVI | −0.83 (−8.8, 7.8) | 6.1 (−1.9, 15) | 0.24 | 1.3 (−6.2, 9.3) | 0.27 (−11, 13) | 0.89 |
| PM10–2.5 | −2.5 (−9.2, 4.7) | −3.9 (−10, 3.1) | 0.78 | −0.30 (−6.5, 6.3) | −6.2 (−14, 2.9) | 0.26 |
| PM2.5 | −0.48 (−9.0, 8.8) | 3.4 (−5.5, 13) | 0.56 | 5.6 (−2.8, 15) | −3.0 (−13, 7.9) | 0.22 |
| Daytime L50 | −2.9 (−9.8, 4.4) | −1.6 (−8.4, 5.6) | 0.80 | 3.1 (−6.8, 14) | −2.2 (−10, 6.1) | 0.42 |
| Nighttime L50 | −3.6 (−10, 3.2) | 0.30 (−6.3, 7.4) | 0.41 | −1.7 (−10, 7.8) | 0.88 (−5.8, 8.0) | 0.66 |
| LAN | −1.9 (−9.5, 6.2) | −3.8 (−11, 3.5) | 0.72 | −1.6 (−8.0, 5.2) | −0.63 (−16, 17) | 0.91 |
| UV | 4.0 (−3.6, 12) | −7.1 (−14, 0.09) | 0.04 | −2.3 (−8.3, 4.1) | 1.3 (−8.5, 12) | 0.56 |
| 1,3-Butadiene | 1.4 (−3.2, 6.3) | −5.8 (−9.9, −1.4) | 0.02 | −2.1 (−5.6, 1.6) | 0.21 (−9.5, 11) | 0.68 |
| Benzene | −2.2 (−8.4, 4.3) | −8.4 (−14, −2.4) | 0.10 | −5.1 (−10, 0.32) | −4.7 (−16, 7.5) | 0.95 |
| Diesel PM | −1.2 (−5.5, 3.2) | −3.6 (−7.3, 0.19) | 0.40 | −2.1 (−5.1, 1.0) | −4.4 (−16, 8.1) | 0.71 |
| Formaldehyde | −1.9 (−8.0, 4.6) | −9.8 (−15, −4.0) | 0.05 | −6.1 (−11, −0.85) | −3.4 (−14, 8.5) | 0.65 |
| Methylene chloride | 0.47 (−3.5, 4.6) | −2.3 (−6.3, 1.9) | 0.34 | −0.20 (−3.6, 3.3) | −0.56 (−7.1, 6.4) | 0.92 |
| Tetrachloroethylene | 0.53 (−2.6, 3.8) | −3.4 (−6.5, −0.20) | 0.07 | −1.0 (−3.4, 1.6) | −1.3 (−8.7, 6.7) | 0.93 |
| Component scoresc | ||||||
| Component 1d | 0.20 (−6.1, 7.0) | −9.3 (−15, −3.4) | 0.03 | −4.5 (−9.4, 0.61) | −2.0 (−15, 13) | 0.73 |
| Component 2e | 1.4 (−4.9, 8.0) | −4.9 (−11, 1.2) | 0.16 | −0.9 (−6.0, 4.4) | −3.2 (−12, 6.1) | 0.67 |
| Component 3f | −3.8 (−9.8, 2.5) | 2.4 (−3.7, 8.9) | 0.16 | 3.7 (−4.6, 13) | 0.08 (−7.1, 7.8) | 0.54 |
| Component 4g | −1.6 (−7.4, 4.7) | 4.3 (−2.0, 11) | 0.19 | 4.8 (−0.9, 11) | −3.7 (−11, 4.1) | 0.08 |
Abbreviations: AMH, anti-Müllerian hormone; SD, standard deviation; FDR, false discovery rate; NDVI, normalized difference vegetation index; PM10–2.5, particulate matter with an aerodynamic diameters between 10 to 2.5 microns; PM2.5, particulate matter with an aerodynamic diameters less than or equal to 2.5 microns; L50, median anthropogenic noise; LAN, light at night; UV, ultraviolet radiation.
Adjusting for age (in natural cubic spline with 3 degrees of freedom), body mass index, race/ethnicity, parity, spouse education status, pre-tax household income, Census tract median income, batches, and smoking.
Defined as Census tract population density ≥ 1,000/km2 (urban) and <1,000/km2 (rural).
Additionally adjusting for other component scores.
Characterized by high loadings for LAN, 1,3-butadiene, benzene, diesel particulate matters, formaldehyde, methylene chloride, and tetrachloroethylene.
Characterized by high loadings for NDVI (negative), PM10–2.5, and UV.
Characterized by high loadings for daytime and nighttime L50.
Characterized by high loading for PM2.5
BKMR models in women over 40 selected surrounding greenness, formaldehyde, and benzene with comparable overall effect estimates as the main model, while no exposures were selected and no overall associations of the exposures with AMH were detected for younger women (eTable 4, Figure 4). No effect modification was evident between urban and rural areas in the single exposure or component score models, although formaldehyde was associated with lower AMH among women from urban areas (Table 4). BKMR showed a negative overall association of the exposures with AMH among women in the urban areas, but no associations were found for women in rural areas (eFigure 3).
Figure 4. Overall association (percentage change and 95% credible intervals) of the exposures with AMH among women under (A) and above age 40 (B).
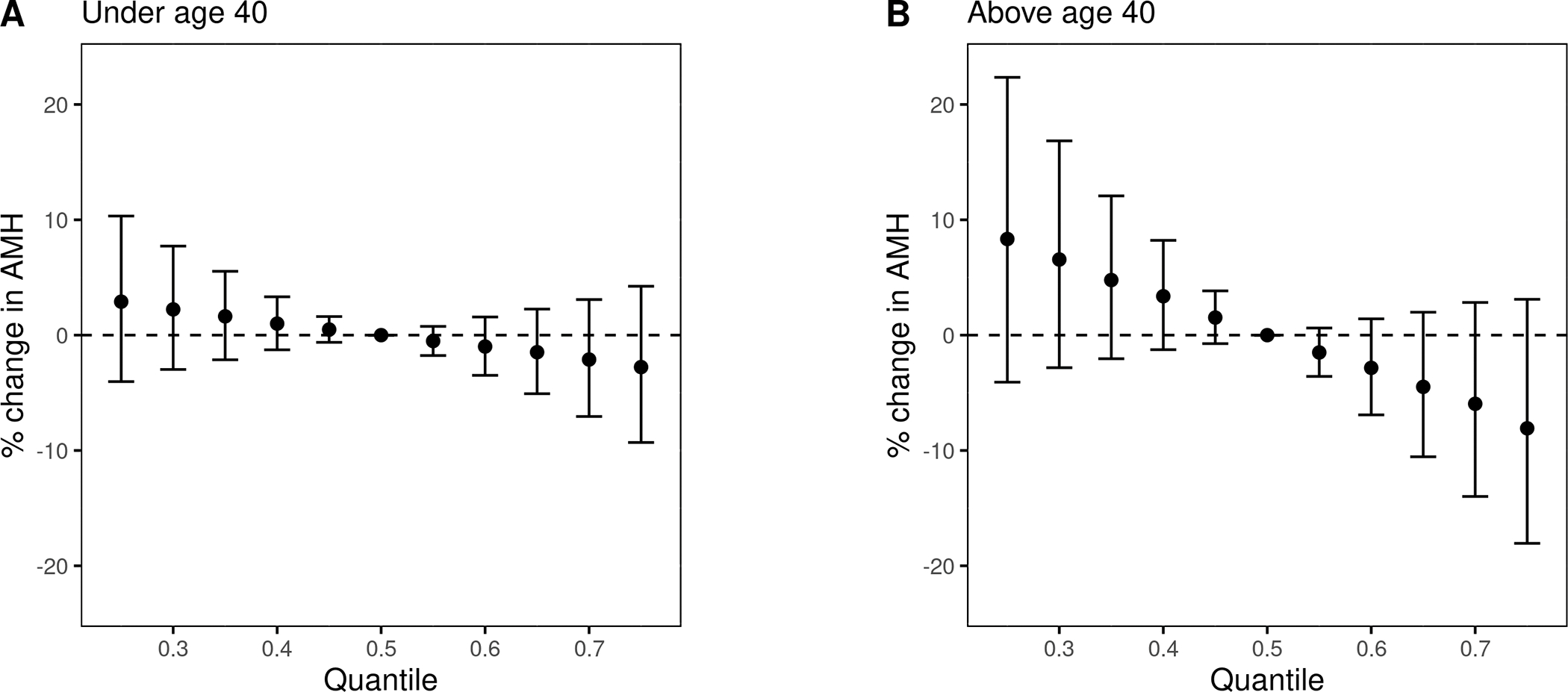
Abbreviations: NDVI, normalized difference vegetation index; AMH, anti-Müllerian hormone.
All exposures in the mixture matrix were standardized. All models were adjusted for age (in natural cubic spline with 3 degrees of freedom), body mass index, Census tract median income, smoking, and other environmental exposures (PM10–2.5, PM2.5, daytime L50, nighttime L50, and UV).
Overall association was computed by comparing when all exposures are fixed at different quantiles to the median.
Sensitivity analyses in models additionally adjusted for oral contraceptive use, breastfeeding, and questionnaire cycles and in models excluding women who reported menopause, hormone related cancer in 5 years after blood draw, and had irregular menstrual cycles in adulthood showed similar results (eTable 5, eFigure 4). Results were also robust when we repeated these sensitivity analyses in women above 40 (eTable 6 and eFigure 5). The estimated associations were similar, albeit slightly attenuated, after restricting to participants whose exposure Mahalanoibis distance within 1 and 2 SDs from the mean and removing participants whose exposure levels were above or below 6 SDs from the mean (data not shown).
Discussion
In this study, we examined associations of exposure to different environmental factors with plasma AMH levels using different mixture methods. Results from the single exposure models, PCA, and BKMR consistently suggested that ambient formaldehyde and benzene were associated with lower AMH. These associations were mainly evident among women older than 40 and were robust in sensitivity analyses. In general, our results showed that, of all the environmental exposures considered, ambient formaldehyde and benzene may be important factors related to female reproductive aging.
Ambient formaldehyde is mainly emitted by power plants, manufacturing facilities, incinerators, and motor vehicle exhaust, while ambient benzene is mainly from coal and oil combustion, motor vehicle exhaust, and evaporation from gasoline stations. Although both chemicals have been recognized as human carcinogens, evidence of their reproductive effects is still limited 39,40. Several studies have suggested that occupational exposure to formaldehyde and benzene could impair ovarian function and fertility. A study of wood workers found women with high formaldehyde exposure (mean concentration = 0.40 mg/m3) had longer time to pregnancy than the unexposed controls 21. One study showed among 70 women working in day care centers with formaldehyde-releasing building materials (mean exposure = 0.43 mg/m3), approximately 35% reported menstrual irregularities, while none in the control group (mean exposure = 0.08 mg/m3) reported the outcome 19. Other studies suggested women who were exposed to organic solvents containing formaldehyde and/or benzene had higher risks of menstrual irregularity, abnormal menstrual cycles or oligomenorrhea, and reduced fertility 18,20,22,41. However, these studies were conducted in occupational settings, where exposure levels were much higher (~250 times) than in the ambient environment. In addition, some studies only examined exposure to a mixture of chemicals and thus associations with individual chemicals were not clear. In the current study, we used mixture methods and found that formaldehyde and benzene were associated with lower AMH, a marker of ovarian reserve, even at low exposure levels found in the ambient environment.
Factors that are associated with oocyte or follicular survival, or can accelerate follicle depletion may affect AMH levels. Genotoxicity and oxidative stress were the possible main pathways mediating cellular damage and apoptosis from formaldehyde and benzene exposures, as suggested in an animal study 42. Two in vitro studies found chromosomal aberrations and DNA damage in ovary cells treated with formaldehyde and benzene metabolites 43,44. Animal studies suggested formaldehyde and benzene can stimulate reactive oxygen species production in reproductive tissue 42,44,45. Evidence in humans also showed increased markers of genotoxicity and oxidative stress with exposure to these compounds 46–53. Animal studies have shown formaldehyde and benzene activate the hypothalamus-pituitary-adrenal (HPA) axis, which can alter neuroendocrine homeostasis and suppress the hypothalamus-pituitary-gonad axis, leading to ovulatory dysfunction 54–56. Other animal studies also showed that elevated glucocorticoids, a marker of HPA activation, may impair oocyte developmental potential and competence, eventually resulting in anovulation and excess follicle atresia 57–60.
Interestingly, BKMR suggested a non-linear relationship between NDVI and AMH while no associations were found for greenness in single or multi-exposure models and PCA. However, this finding may be attributable to overfitting, which can be difficult to diagnose and prevent in BKMR. Therefore, this result should be interpreted with caution. Although our previous analysis in the NHSII suggested PM was modestly associated with earlier menopause 15, we observed no associations between PM2.5–10 or PM2.5 and AMH. So far, two studies reported inconsistent results for the association of PM with AMH 12,14. Such inconsistency may be due to differences in the study population, exposure levels and time windows of exposures examined, and geographic characteristics.
The observed associations in the main analysis were found in women above age 40, while there was less evidence of associations among younger women. These findings suggest that women in the late reproductive and peri-menopausal stage may be more vulnerable to external exposures. All primordial oocytes are formed at the fetal stage and can stay resting in the ovary for more than 40 years, exposed to both the internal and external stressors 61–63. It has been documented that oocytes have more chromosomal abnormality and cellular dysfunction with age, leading to greater vulnerability to any additional damage from the environment 63. Additionally, as follicle reserve has been greatly reduced by age 40, any excess follicle loss at this stage can be reflected by greater relative change in AMH 61,62.
A number of mixture analysis methods have been proposed and it is recommended to verify findings using different methods 64. Although the single exposure model, PCA, and BKMR consistently suggested that formaldehyde and benzene were associated with lower AMH, these results should be interpreted differently. Estimates from single-exposure models can inform the associations of each exposure with AMH but were subject to residual confounding by other exposures. Multi-exposure model can estimate the associations while holding all other exposures constant. However, collinearity among exposures can lead to unstable estimates and wide confidence intervals. PCA can avoid multicollinearity by projecting the exposures into fewer independent components, but the associations of individual exposure with the outcome cannot be estimated. Meanwhile, BKMR is flexible for selecting the most important exposures associated with the outcome and non-linear relationships, which the other methods may have limited ability to address. However, we only included exposures in the first component for BKMR selection to reduce the impact of noise by other exposures. Therefore, our BKMR results should be interpreted differently from linear models and PCA, as the most important exposures were selected from a subset of exposures and the individual and joint associations of exposures were estimated by holding the other exposures (i.e., those not included for selection) constant in addition to the covariates.
This study had notable limitations on exposure measurement. First, we relied on ambient measures of exposure at the residential address, which could lead to exposure measurement error. For example, these measures did not consider participant’s time spent at home, nor did they capture the use of mitigations. NDVI from satellite image had limited ability capturing the quality, type, accessibility, and actual interactions of the participants with greenspace. Because formaldehyde has also been suggested to be an indoor air pollutant, the ambient formaldehyde measure may not fully represent the actual personal exposure level for our participants. The EPA has validated the 1999 NATA estimates with monitoring data and showed that benzene can be both over- and underestimated while formaldehyde was largely underestimated 65. However, as these air toxins are rarely monitored across the country, we had to rely on NATA to estimate exposure to hazardous air pollutants in this study. There were also temporal mismatches for noise, light at night, and hazardous air pollutants due to limited data availability. Although part of the exposure measurement error was likely non-differential, it can be difficult to quantify the overall impact of exposure measurement error due to the lack of monitoring data and the use of complex statistical modeling such as BKMR.
Other limitations include that we only controlled for a limited number of potential confounders in our models, so residual confounding is possible. However, our sensitivity analysis adjusting for additional covariates showed that our models are likely robust to residual confounding. Most participants were selected from nested case–control studies in NHSII, Therefore, collider stratification bias is possible. However, all controls were selected based on matching for demographic and health factors such as age, pregnancy, and breastfeeding, and the environmental exposure levels were comparable between the cases and controls (eTable 7). Plasma AMH levels were only measured once in our participants. Therefore, we cannot capture the AMH trajectory to reflect ovarian aging. Long-term stability of AMH in plasma samples is unclear, although previous studies suggested that plasma or serum AMH was stable under −80°C for 5–7 days 66. In addition, due to the limited exposure data available in NHSII, we did not consider other exposures such as endocrine disruptors and occupational exposures. Finally, our results had limited generalizability to the entire NHSII cohort and the general US women population as we oversampled women with breast cancer and early menopause in the study population.
Nevertheless, compared to previous studies, our study has a number of strengths. The sample size is relatively large. Unlike most other sex steroids, circulating AMH level was stable across menstrual cycle and so the timing of blood draw in menstrual cycle may not affect our outcome measurement 67. In addition to examining the associations of each single exposure with AMH, we conducted mixture analyses to characterize patterns of exposure among these environmental factors, estimate the overall and individual association of these exposures with AMH, and identify the key exposures. Although these methods may be used for different study questions 68, they consistently showed inverse associations of ambient hazardous air pollutants, among which formaldehyde and benzene were the most important exposures. Finally, this availability of nearly 10 years of environmental exposure data allowed us to examine the impacts of long-term exposures during adulthood.
Conclusion
In this mixture analysis, we comprehensively examined associations of multiple environmental exposures with AMH, a marker of reproductive aging, in a subset of NHSII participants. Results from the single and multiple exposure models, PCA, and BKMR consistently showed inverse associations of ambient formaldehyde and benzene with AMH. These observed associations were mainly found in women above age 40. Our results are consistent with the hypothesis that ambient formaldehyde and benzene can accelerate ovarian aging, and that women in the late reproductive or perimenopausal stage are more susceptible.
Supplementary Material
Acknowledgment
This study was supported by the NIH grants U01 CA176726, U01 HL145386, R01 CA67262, R01 ES028033, R01 HL150119, and P30 ES000002.
Footnotes
Conflict of interest: None.
Reference
- 1.Duncan FE, Confino R, Pavone ME. Female Reproductive Aging. In: Conn’s Handbook of Models for Human Aging. Elsevier; 2018:109–130. doi: 10.1016/B978-0-12-811353-0.00009-9 [DOI] [Google Scholar]
- 2.Soules MR, Sherman S, Parrott E, et al. Executive summary: stages of reproductive aging workshop (STRAW). Fertil Steril. 2001;76(5):874–878. doi: 10.1016/S0015-0282(01)02909-0 [DOI] [PubMed] [Google Scholar]
- 3.Traub ML, Santoro N. Reproductive aging and its consequences for general health. Ann N Y Acad Sci. 2010;1204:179–187. doi: 10.1111/j.1749-6632.2010.05521.x [DOI] [PubMed] [Google Scholar]
- 4.Aydogan B, Mirkin S. The utility of measuring anti-Müllerian hormone in predicting menopause. Climacteric J Int Menopause Soc. 2015;18(6):777–789. doi: 10.3109/13697137.2015.1036853 [DOI] [PubMed] [Google Scholar]
- 5.Bertone-Johnson ER, Manson JE, Purdue-Smithe AC, et al. Anti-Müllerian hormone levels and incidence of early natural menopause in a prospective study. Hum Reprod Oxf Engl. 2018;33(6):1175–1182. doi: 10.1093/humrep/dey077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Broer SL, Broekmans FJM, Laven JSE, Fauser BCJM. Anti-Müllerian hormone: ovarian reserve testing and its potential clinical implications. Hum Reprod Update. 2014;20(5):688–701. doi: 10.1093/humupd/dmu020 [DOI] [PubMed] [Google Scholar]
- 7.Freeman EW, Sammel MD, Lin H, Gracia CR. Anti-Mullerian Hormone as a Predictor of Time to Menopause in Late Reproductive Age Women. J Clin Endocrinol Metab. 2012;97(5):1673–1680. doi: 10.1210/jc.2011-3032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hansen KR, Hodnett GM, Knowlton N, Craig LB. Correlation of ovarian reserve tests with histologically determined primordial follicle number. Fertil Steril. 2011;95(1):170–175. doi: 10.1016/j.fertnstert.2010.04.006 [DOI] [PubMed] [Google Scholar]
- 9.Rosen MP, Johnstone E, McCulloch CE, et al. A characterization of the relationship of ovarian reserve markers with age. Fertil Steril. 2012;97(1):238–243. doi: 10.1016/j.fertnstert.2011.10.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.de Kat AC, Verschuren WM, Eijkemans MJC, Broekmans FJM, van der Schouw YT. Anti-Müllerian Hormone Trajectories Are Associated With Cardiovascular Disease in Women: Results From the Doetinchem Cohort Study. Circulation. 2017;135(6):556–565. doi: 10.1161/CIRCULATIONAHA.116.025968 [DOI] [PubMed] [Google Scholar]
- 11.Verdiesen RMG, Onland-Moret NC, van Gils CH, et al. Anti-Müllerian hormone levels and risk of type 2 diabetes in women. Diabetologia. 2021;64(2):375–384. doi: 10.1007/s00125-020-05302-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abareshi F, Sharifi Z, Hekmatshoar R, et al. Association of exposure to air pollution and green space with ovarian reserve hormones levels. Environ Res. 2020;184:109342. doi: 10.1016/j.envres.2020.109342 [DOI] [PubMed] [Google Scholar]
- 13.Kim H, Choe SA, Kim OJ, et al. Outdoor air pollution and diminished ovarian reserve among infertile Korean women. Environ Health Prev Med. 2021;26(1):20. doi: 10.1186/s12199-021-00942-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.La Marca A, Spaggiari G, Domenici D, et al. Elevated levels of nitrous dioxide are associated with lower AMH levels: a real-world analysis. Hum Reprod Oxf Engl. 2020;35(11):2589–2597. doi: 10.1093/humrep/deaa214 [DOI] [PubMed] [Google Scholar]
- 15.Li H, Hart JE, Mahalingaiah S, Nethery RC, Bertone-Johnson E, Laden F. Long-term exposure to particulate matter and roadway proximity with age at natural menopause in the Nurses’ Health Study II Cohort. Environ Pollut. 2021;269:116216. doi: 10.1016/j.envpol.2020.116216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Li H, Hart JE, Mahalingaiah S, et al. Ultraviolet radiation and age at natural menopause in a nationwide, prospective US cohort. Environ Res. 2022;203:111929. doi: 10.1016/j.envres.2021.111929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Triebner K, Markevych I, Hustad S, et al. Residential surrounding greenspace and age at menopause: A 20-year European study (ECRHS). Environ Int. 2019;132:105088. doi: 10.1016/j.envint.2019.105088 [DOI] [PubMed] [Google Scholar]
- 18.Hassani S, Namvar M, Ghoreishvandi M, et al. Menstrual disturbances and hormonal changes in women workers exposed to a mixture of organic solvents in a pharmaceutical company. Med J Islam Repub Iran. 2014;28:156. [PMC free article] [PubMed] [Google Scholar]
- 19.Olsen JH, Døssing M. Formaldehyde induced symptoms in day care centers. Am Ind Hyg Assoc J. 1982;43(5):366–370. doi: 10.1080/15298668291409866 [DOI] [PubMed] [Google Scholar]
- 20.Reutman SR, LeMasters GK, Knecht EA, et al. Evidence of reproductive endocrine effects in women with occupational fuel and solvent exposures. Environ Health Perspect. 2002;110(8):805–811. doi: 10.1289/ehp.02110805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Taskinen HK, Kyyrönen P, Sallmén M, et al. Reduced fertility among female wood workers exposed to formaldehyde. Am J Ind Med. 1999;36(1):206–212. doi: 10.1002/(sici)1097-0274(199907)36:1<206::aid-ajim29>3.0.co;2-d [DOI] [PubMed] [Google Scholar]
- 22.Thurston SW, Ryan L, Christiani DC, et al. Petrochemical exposure and menstrual disturbances. Am J Ind Med. 2000;38(5):555–564. doi: 10.1002/1097-0274(200011)38:5<555::aid-ajim8>3.0.co;2-e [DOI] [PubMed] [Google Scholar]
- 23.Eliassen AH, Missmer SA, Tworoger SS, et al. Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women. J Natl Cancer Inst. 2006;98(19):1406–1415. doi: 10.1093/jnci/djj376 [DOI] [PubMed] [Google Scholar]
- 24.Eliassen AH, Zeleniuch-Jacquotte A, Rosner B, Hankinson SE. Plasma Anti-Müllerian Hormone Concentrations and Risk of Breast Cancer among Premenopausal Women in the Nurses’ Health Studies. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2016;25(5):854–860. doi: 10.1158/1055-9965.EPI-15-1240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jung S, Allen N, Arslan AA, et al. Anti-Müllerian hormone and risk of ovarian cancer in nine cohorts. Int J Cancer. 2018;142(2):262–270. doi: 10.1002/ijc.31058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.USGS. NDVI from AVHRR. Published 2018. Accessed June 19, 2020. https://www.usgs.gov/core-science-systems/eros/phenology/science/ndvi-avhrr?qt-science_center_objects=0#qt-science_center_objects
- 27.Klompmaker JO, Hoek G, Bloemsma LD, et al. Green space definition affects associations of green space with overweight and physical activity. Environ Res. 2018;160:531–540. doi: 10.1016/j.envres.2017.10.027 [DOI] [PubMed] [Google Scholar]
- 28.Yanosky JD, Paciorek CJ, Laden F, et al. Spatio-temporal modeling of particulate air pollution in the conterminous United States using geographic and meteorological predictors. Environ Health. 2014;13(1):63. doi: 10.1186/1476-069X-13-63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mennitt DJ, Fristrup KM. Influence factors and spatiotemporal patterns of environmental sound levels in the contiguous United States. Noise Control Eng J. 2016;64(3):342–353. doi: 10.3397/1/376384 [DOI] [Google Scholar]
- 30.NOAA. Version 4 DMSP-OLS Nighttime Lights Time Series. Published 2017. Accessed June 18, 2020. https://ngdc.noaa.gov/eog/dmsp/downloadV4composites.html#AVSLCFC
- 31.VoPham T, Hart JE, Bertrand KA, Sun Z, Tamimi RM, Laden F. Spatiotemporal exposure modeling of ambient erythemal ultraviolet radiation. Environ Health. 2016;15(1):111. doi: 10.1186/s12940-016-0197-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Garcia E, Hurley S, Nelson DO, Hertz A, Reynolds P. Hazardous air pollutants and breast cancer risk in California teachers: a cohort study. Environ Health Glob Access Sci Source. 2015;14:14. doi: 10.1186/1476-069X-14-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hart JE, Bertrand KA, DuPre N, et al. Exposure to hazardous air pollutants and risk of incident breast cancer in the nurses’ health study II. Environ Health Glob Access Sci Source. 2018;17(1):28. doi: 10.1186/s12940-018-0372-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Liu R, Nelson DO, Hurley S, Hertz A, Reynolds P. Residential exposure to estrogen disrupting hazardous air pollutants and breast cancer risk: the California Teachers Study. Epidemiol Camb Mass. 2015;26(3):365–373. doi: 10.1097/EDE.0000000000000277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Schober P, Boer C, Schwarte LA. Correlation Coefficients: Appropriate Use and Interpretation. Anesth Analg. 2018;126(5):1763–1768. doi: 10.1213/ANE.0000000000002864 [DOI] [PubMed] [Google Scholar]
- 36.Schober P, Vetter TR. Correlation Analysis in Medical Research: Anesth Analg. 2020;130(2):332. doi: 10.1213/ANE.0000000000004578 [DOI] [PubMed] [Google Scholar]
- 37.Bobb JF, Valeri L, Claus Henn B, et al. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics. 2015;16(3):493–508. doi: 10.1093/biostatistics/kxu058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bobb JF, Claus Henn B, Valeri L, Coull BA. Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ Health. 2018;17(1):67. doi: 10.1186/s12940-018-0413-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 120, Benzene.; 2019. [PMC free article] [PubMed] [Google Scholar]
- 40.IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 88, Formaldehyde, 2-Butoxyethanol and 1-Tert-Butoxypropan-2-Ol.; 2006. [PMC free article] [PubMed] [Google Scholar]
- 41.Cho SI, Damokosh AI, Ryan LM, et al. Effects of exposure to organic solvents on menstrual cycle length. J Occup Environ Med. 2001;43(6):567–575. doi: 10.1097/00043764-200106000-00012 [DOI] [PubMed] [Google Scholar]
- 42.Duong A, Steinmaus C, McHale CM, Vaughan CP, Zhang L. Reproductive and developmental toxicity of formaldehyde: A systematic review. Mutat Res Mutat Res. 2011;728(3):118–138. doi: 10.1016/j.mrrev.2011.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Natarajan AT, Darroudi F, Bussman CJ, van Kesteren-van Leeuwen AC. Evaluation of the mutagenicity of formaldehyde in mammalian cytogenetic assays in vivo and vitro. Mutat Res. 1983;122(3–4):355–360. doi: 10.1016/0165-7992(83)90019-2 [DOI] [PubMed] [Google Scholar]
- 44.Winn LM. Homologous recombination initiated by benzene metabolites: a potential role of oxidative stress. Toxicol Sci Off J Soc Toxicol. 2003;72(1):143–149. doi: 10.1093/toxsci/kfg008 [DOI] [PubMed] [Google Scholar]
- 45.Ozen OA, Kus MA, Kus I, Alkoc OA, Songur A. Protective Effects of Melatonin Against Formaldehyde-Induced Oxidative Damage and Apoptosis in Rat Testes: An Immunohistochemical and Biochemical Study. Syst Biol Reprod Med. 2008;54(4–5):169–176. doi: 10.1080/19396360802422402 [DOI] [PubMed] [Google Scholar]
- 46.Amin MM, Rafiei N, Poursafa P, et al. Association of benzene exposure with insulin resistance, SOD, and MDA as markers of oxidative stress in children and adolescents. Environ Sci Pollut Res Int. 2018;25(34):34046–34052. doi: 10.1007/s11356-018-3354-7 [DOI] [PubMed] [Google Scholar]
- 47.Costa-Amaral IC, Carvalho LVB, Santos MVC, et al. Environmental Assessment and Evaluation of Oxidative Stress and Genotoxicity Biomarkers Related to Chronic Occupational Exposure to Benzene. Int J Environ Res Public Health. 2019;16(12). doi: 10.3390/ijerph16122240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Fenech M, Nersesyan A, Knasmueller S. A systematic review of the association between occupational exposure to formaldehyde and effects on chromosomal DNA damage measured using the cytokinesis-block micronucleus assay in lymphocytes. Mutat Res. 2016;770(Pt A):46–57. doi: 10.1016/j.mrrev.2016.04.005 [DOI] [PubMed] [Google Scholar]
- 49.Fracasso ME, Doria D, Bartolucci GB, et al. Low air levels of benzene: Correlation between biomarkers of exposure and genotoxic effects. Toxicol Lett. 2010;192(1):22–28. doi: 10.1016/j.toxlet.2009.04.028 [DOI] [PubMed] [Google Scholar]
- 50.Marcon A, Fracasso ME, Marchetti P, et al. Outdoor formaldehyde and NO2 exposures and markers of genotoxicity in children living near chipboard industries. Environ Health Perspect. 2014;122(6):639–645. doi: 10.1289/ehp.1307259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Scholten B, Vlaanderen J, Stierum R, et al. A Quantitative Meta-Analysis of the Relation between Occupational Benzene Exposure and Biomarkers of Cytogenetic Damage. Environ Health Perspect. 2020;128(8):087004. doi: 10.1289/EHP6404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Squillacioti G, Bellisario V, Grosso A, et al. Formaldehyde, Oxidative Stress, and FeNO in Traffic Police Officers Working in Two Cities of Northern Italy. Int J Environ Res Public Health. 2020;17(5). doi: 10.3390/ijerph17051655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Zhou Y, Wang K, Wang B, Pu Y, Zhang J. Occupational benzene exposure and the risk of genetic damage: a systematic review and meta-analysis. BMC Public Health. 2020;20(1):1113. doi: 10.1186/s12889-020-09215-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hsieh GC, Sharma RP, Parker RD. Hypothalamic-pituitary-adrenocortical axis activity and immune function after oral exposure to benzene and toluene. Immunopharmacology. 1991;21(1):23–31. doi: 10.1016/0162-3109(91)90004-i [DOI] [PubMed] [Google Scholar]
- 55.Sari DK, Kuwahara S, Tsukamoto Y, et al. Effect of prolonged exposure to low concentrations of formaldehyde on the corticotropin releasing hormone neurons in the hypothalamus and adrenocorticotropic hormone cells in the pituitary gland in female mice. Brain Res. 2004;1013(1):107–116. doi: 10.1016/j.brainres.2004.03.070 [DOI] [PubMed] [Google Scholar]
- 56.Sorg BA, Bailie TM, Tschirgi ML, Li N, Wu WR. Exposure to repeated low-level formaldehyde in rats increases basal corticosterone levels and enhances the corticosterone response to subsequent formaldehyde. Brain Res. 2001;898(2):314–320. doi: 10.1016/s0006-8993(01)02208-9 [DOI] [PubMed] [Google Scholar]
- 57.Gao Y, Chen F, Kong QQ, et al. Stresses on Female Mice Impair Oocyte Developmental Potential: Effects of Stress Severity and Duration on Oocytes at the Growing Follicle Stage. Reprod Sci. 2016;23(9):1148–1157. doi: 10.1177/1933719116630416 [DOI] [PubMed] [Google Scholar]
- 58.Joseph DN, Whirledge S. Stress and the HPA Axis: Balancing Homeostasis and Fertility. Int J Mol Sci. 2017;18(10). doi: 10.3390/ijms18102224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Yuan HJ, Han X, He N, et al. Glucocorticoids impair oocyte developmental potential by triggering apoptosis of ovarian cells via activating the Fas system. Sci Rep. 2016;6(1):24036. doi: 10.1038/srep24036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Yuan HJ, Li ZB, Zhao XY, et al. Glucocorticoids impair oocyte competence and trigger apoptosis of ovarian cells via activating the TNF-α system. Reproduction. 2020;160(1):129–140. doi: 10.1530/REP-20-0025 [DOI] [PubMed] [Google Scholar]
- 61.Broekmans FJ, Soules MR, Fauser BC. Ovarian Aging: Mechanisms and Clinical Consequences. Endocr Rev. 2009;30(5):465–493. doi: 10.1210/er.2009-0006 [DOI] [PubMed] [Google Scholar]
- 62.Broekmans FJ, Knauff EAH, te Velde ER, Macklon NS, Fauser BC. Female reproductive ageing: current knowledge and future trends. Trends Endocrinol Metab. 2007;18(2):58–65. doi: 10.1016/j.tem.2007.01.004 [DOI] [PubMed] [Google Scholar]
- 63.Dorland M, van Kooij RJ, te Velde ER. General ageing and ovarian ageing. Maturitas. 1998;30(2):113–118. doi: 10.1016/s0378-5122(98)00066-8 [DOI] [PubMed] [Google Scholar]
- 64.Taylor KW, Joubert BR, Braun JM, et al. Statistical Approaches for Assessing Health Effects of Environmental Chemical Mixtures in Epidemiology: Lessons from an Innovative Workshop. Environ Health Perspect. 2016;124(12). doi: 10.1289/EHP547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.US EPA. Comparison of 1999 Model-Predicted Concentrations to Monitored Data. https://archive.epa.gov/airtoxics/nata1999/web/html/99compare.html
- 66.Rustamov O, Smith A, Roberts SA, et al. The Measurement of Anti-Müllerian Hormone: A Critical Appraisal. J Clin Endocrinol Metab. 2014;99(3):723–732. doi: 10.1210/jc.2013-3476 [DOI] [PubMed] [Google Scholar]
- 67.La Marca A, Stabile G, Artenisio AC, Volpe A. Serum anti-Mullerian hormone throughout the human menstrual cycle. Hum Reprod. 2006;21(12):3103–3107. doi: 10.1093/humrep/del291 [DOI] [PubMed] [Google Scholar]
- 68.Gibson EA, Nunez Y, Abuawad A, et al. An overview of methods to address distinct research questions on environmental mixtures: an application to persistent organic pollutants and leukocyte telomere length. Environ Health. 2019;18(1):76. doi: 10.1186/s12940-019-0515-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.