

Abstract
Background & Aims
Research quantifying dietary intake in individuals with bulimia nervosa and binge-eating disorder (i.e., binge-type eating disorders) is surprisingly scant. We assessed the dietary intake of women and men with binge-type eating disorders in a large case-control study and compared them with healthy controls. We also evaluated the extent to which their dietary intake adhered to the Nordic Nutrition Recommendations. Among cases, we assessed the relationship of binge eating frequency with energy and macronutrient intake.
Methods
We derived the total daily energy, macro-, and micronutrient intake of 430 cases with binge-type eating disorders (women: n=391, men: n=39) and 1,227 frequency-matched controls (women: n=1,213, men: n=14) who completed the MiniMeal-Q, a validated food frequency questionnaire. We calculated mean intake for men and women and, in women, compared mean intake of energy and nutrients between cases and controls using linear regression. We calculated the proportion of women and men who met the recommended intake levels from the NNR, and compared these proportions in female cases and controls using logistic regression. We used linear regression to examine energy and macronutrient intake of women with varying frequencies of current binge-eating.
Results
Female, but not male cases, had a higher mean intake of total energy/day compared with controls and higher intake than recommended. The majority in all groups (male and female cases and controls) exceeded saturated fat recommendations, and did not meet recommendations for omega-3 fatty acid intake. Among all groups, adherence was low for vitamin D, selenium, and salt. Iron and folate intake was low among the majority of women, especially controls. Female cases with ≥4 binge-eating episodes in the past 28 days had higher intake of energy and percent carbohydrates, and lower intake of percent fat, compared to cases with no binge-eating episodes in the past month.
Conclusions
Higher than recommended total daily energy intake among women with binge-type eating disorders may lead to weight gain and downstream health complications, if persistent. In most women, iron and folate intake was insufficient, which may have negative consequences for reproductive health. We found suboptimal adherence for key nutrients that are important to limit (saturated fat and salt) or meet (omega-3 fatty acids) for cardiovascular and overall health in all groups. Nutrition counseling should form an important pillar of treatment to assist with normalization of eating patterns and may also benefit individuals without eating disorders to optimize nutrient intake for long term health promotion.
Keywords: eating disorders, diet, nutrition, macronutrients, micronutrients, NNR
INTRODUCTION
Bulimia nervosa (BN) and binge-eating disorder (BED) are eating disorders characterized by recurrent episodes of eating an unusually large amount of food coupled with a sense of feeling out of control (i.e., binge-eating). In BN, but not in BED, binge eating is accompanied by recurrent inappropriate compensatory behaviors to reduce weight gain or counter the binge such as self-induced vomiting, misuse of laxatives or diuretics, fasting, or excessive exercise (1). These dysregulated eating patterns can lead to inadequate intake of micronutrients, but also potentially to an excess intake of some macronutrients, especially fats and carbohydrates.
Comparisons of the dietary intake of women with BN and BED with those of healthy controls are limited and have rarely been compared against published nutrient recommendations. Such comparisons are important in order to better understand how nutrition counseling may be tailored to the unique treatment needs of individuals with BN and BED. Existing studies have focused primarily on total calorie and macronutrient intake. Alpers et al. reported that individuals with BN consume a diet matching dietary guidelines more closely than a control group in terms of macronutrient composition (2). However, several studies report increased total energy intake and absolute amounts of macronutrients consumed—particularly carbohydrates and fat—among individuals with BN (3) and BED (2, 4, 5) compared to controls without an eating disorder, particularly on days when binge eating occurs. In laboratory settings, individuals with BED consume higher amounts of calories compared to control individuals without BED, both when instructed to simulate a binge-eating episode, and when instructed to eat in a normal fashion (6). Laboratory studies have consistently found that individuals with BN and BED have a higher caloric intake than controls without eating disorders both when participants are presented with an array of foods, and in studies using single item test meals (7). Engel et al. combined ecological momentary assessment with dietary recall methods and reported a statistically significant increase in total number of calories consumed, loss of control, overeating, and binge eating among individuals with obesity and BED, compared with individuals with obesity but without BED or healthy normal-weight controls (8).
The literature is deficient in documenting micronutrient intake among individuals with binge-type eating disorders, particularly among men, including comparisons to that of healthy controls. The micronutrient intake of individuals with eating disorders is critical to monitor given the potential for deficiencies, which may lead to worsened health outcomes in an already vulnerable population. Deficiencies are not always reflected in blood levels due to compensatory physiologic mechanisms, food-group specific restriction, and/or self-administered nutrient supplementation, which can lead to laboratory values appearing within normal limits (9). Therefore, self-reported micronutrient intake is an important complement to physiologic levels, as both self-reported intake levels and circulating levels of nutrients have important limitations and may provide an incomplete picture about nutrition status if used in isolation. It may be especially important to monitor nutrition status over the course of disease treatment as an indicator of treatment efficacy given the high risk of mal- or under-nutrition and its associated comorbidities among individuals with eating disorders (10, 11).
Conflicting results in the field can be attributed, in part, to the lack of precision in many methods of assessing dietary intake. Many studies assessing the nutrient intake of individuals with BED and BN (heretofore referred to as “binge-type eating disorders”) have very small samples, limiting the likelihood of finding group differences compared with healthy controls. Furthermore, a very limited number of studies have assessed dietary intake among men with binge-type eating disorders. To our knowledge, virtually no studies have assessed micronutrient intakes among individuals with binge-type eating disorders who are of Scandinavian origin—an important population to study given the increased prevalence of BN in this region compared to other European regions (12). The aims of this study were to: 1) compare the diet quality of a large sample of women and men with binge-type eating disorders to that of control participants without an eating disorder (i.e., mean energy and percent micro- and macronutrient intake and adherence to the Nordic Nutrition recommendations [2012]); and 2) to compare energy and percent macronutrient intake across strata of binge-eating frequency in the past 28 days among women with binge-type eating disorders (13).
MATERIALS & METHODS
Study design and study sample
The Binge Eating Genetics Initiative in Sweden (BEGIN-SE) was a large-scale, case-control study collecting genetic, microbiome, and phenotypic data in individuals with BN and BED as well as in controls. Cases were identified in the pre-existing national quality register (Riksät) for individuals who had ever undergone an initial meeting with a specialized eating disorder treatment unit with a lifetime diagnosis of BN or BED. We were unable to identify their current treatment status. Riksät started in 1999 and is a quality register for individuals in treatment for eating disorders within the universal health care service of Sweden (14). The eating disorder diagnoses recorded in the register are determined using structured diagnostic interviews conducted by a clinician. Individuals with a diagnosis of BN and/or BED who were 18 years old or older were invited to participate in BEGIN-SE (almost 100% coverage, 27% response rate). Individuals reporting to have had a lifetime history of anorexia nervosa were excluded from participation in order to focus our research question on binge-type eating disorders. In this study, individuals with BN and/or BED were included in the analysis as one group. Controls in BEGIN-SE were recruited with the assistance of a professional company from a population sample, and were frequency matched on age and gender, had no prior history or family history of eating disorders, and were not taking any medication for other psychiatric illness at the time of participation. The ratio of cases to controls recruited for the larger BEGIN-SE study was 1:2. Additional exclusion criteria for both cases and controls recruited for BEGIN-SE were weight reduction surgery, inflammatory bowel disease (e.g., ulcerative colitis), current treatment with antibiotics or probiotics, being on hormone replacement therapy, and being pregnant or breastfeeding. Control participants were asked about prior history of an eating disorder during the screening process. We further excluded controls who reported any eating disorder symptoms in the ED100K. A more detailed description of the BEGIN-SE protocol has been described previously (15).
Participants in BEGIN-SE answered several validated, web-based questionnaires and provided a saliva sample for DNA extraction, and one fecal sample for gut microbiota analysis. The BEGIN-SE study was approved by the Regional Ethical Review Board in Stockholm, Sweden. Participants signed an electronic informed consent before entering the study.
Dietary intake data were available for 465 cases (422 women and 43 men) and 1,240 controls (1,226 women and 14 men). Thirty-one participants (15 female cases, 13 female controls, and 3 male cases) with implausible energy intake (<800 kcal/day or >8000 kcal/day) were excluded from the analysis. The minimum threshold of 800 kcal was selected based upon a population-based study of dietary intake conducted in Sweden (16). The upper threshold of 8,000 kcal was selected to allow for inclusion of case participants with large numbers of daily binge-eating episodes. These thresholds were further justified given the absence of differences in the proportions of over- or under reporters that were excluded among cases or controls. Given the need to compute age-specific nutrient requirements, we excluded 10 female cases who were missing information about age. We further excluded 4 cases whose ages were <18 years, given differences in total energy and micronutrient needs for children under the age of 18. We excluded 3 cases whose ages were >51 years, given that this is the mean age of menopause in Sweden, which influences recommended intake for iron (17). Therefore, the final analytic sample for the present case-control analysis included 430 cases (391 women and 39 men) and 1,227 controls (1,213 women and 14 men), recruited between December 2017 and February 2020.
Measures
MiniMeal-Q
The MiniMeal-Q (18, 19) is an interactive, web-based food frequency questionnaire (FFQ) that includes 75-126 questions about food items, beverages, and dishes, but not dietary supplements, for assessing habitual food habits. It has been validated in Scandinavian study samples but not specifically in individuals with eating disorders. However, a prior study successfully detected differences in the dietary intakes of individuals with and without binge eating disorder or bulimia nervosa using a food frequency questionnaire that was not validated among individuals without eating disorders (20). The participants chose how often they consumed different foods and dishes from a predefined list. The number of questions depended on the participant’s previous responses and adapted so that the participant only had to answer questions that were relevant to them. For the three following food groups: 1) rice, potatoes, and pasta; 2) vegetables (raw and cooked); and 3) meat, fish, chicken, and vegetarian substitutes, the participants also defined the portion size they normally ate on a 5-point scale, ranging from small (1) to large (5) illustrated by photos. For all other food items and beverages, a standard portion size was defined by the Swedish National Food Agency, the Swedish Consumer Agency, portion sizes developed by the research group, or used in other studies at Karolinska Institutet.
Nutrient database
The intake of food items, beverages, and dishes reported in MiniMeal-Q were converted into energy per day (kcal/day), macronutrient intake per day (g/day), and micronutrient intake per day (g, mg, μg/day, retinol equivalents [RE]/day, niacin equivalent [NE]/day, or alpha tocopherol equivalent [α-TE]/day) by linkage to the national database of nutrient contents published by the Swedish National Food Agency (21).
Nordic Nutrition Recommendations (NNR)
The NNR 2012 include reference values for recommended daily intake (RDI) for a) absolute intake of energy, macronutrients, and micronutrients; and b) percentage of energy intake (abbreviated %E) from fats (total and saturated, monounsaturated, polyunsaturated, and omega-3 polyunsaturated), carbohydrates, and protein (13).
ED100Kv2
The ED100Kv2 (22) is a self-report questionnaire that captures information on lifetime history of eating disorders and disordered eating behavior. A validation study on the ED100Kv1 confirmed a positive predictive value of binge eating between 0.85 and 0.93 (22).
We classified cases into groups who reported having had a BN and/or BED diagnosis in their lifetime. From the ED100Kv2, we collected information about current and lifetime lowest and highest BMI. Gender was self-reported as male, female, not known, or not applicable.
Eating Disorders Examination Questionnaire (EDE-Q)
The EDE-Qv4 (23) is a validated questionnaire assessing eating disorder symptoms and behaviors over the past 28 days. Responses on the EDE-Qv4 were used to assess the number of recent binge-eating episodes.
Statistical Analysis
All statistical analyses were conducted using R, version 3.6.2 (24). Differences in baseline age and BMI between female cases and controls were tested using Student’s t-test.
To compute reference ranges for total energy, we used age- and gender-specific reference calculations from NNR, which included physical activity levels (PAL) and reference weights. We used age-specific calculations for individuals ages 18-30 and 31-60. Calculations corresponded to a BMI of 23 kg/m2, based on the heights of Nordic populations (13). To compute age- and gender-specific lower and upper reference ranges for total energy, we used a PAL of 1.4 megajoules (MJ)/day and a PAL of 1.8 MJ/day, which correspond to a sedentary and an active lifestyle, respectively. References ranges for PAL were extrapolated from average Swedish data given that we lacked individual-level data for physical activity. Recommendations for macronutrients as percent of energy were used, which in the NNR are the same for all adults irrespective of age.
Means and standard deviations (SD) were calculated for total energy, macronutrients, and micronutrients. We further calculated the proportion of cases and controls who met the recommended intake levels according to the NNR for energy and all micro- and macronutrients. For total energy and most macronutrients (total fat, monounsaturated fat, polyunsaturated fat, total protein, and total carbohydrates), we computed the proportion of participants who met the recommended reference range, but did not exceed it. For saturated fat and salt, we computed the proportion of individuals who did not exceed the recommended upper intake levels. For omega-3 fatty acids, fiber, and all micronutrients except salt, we computed the proportion of participants who achieved minimum recommended intake. Upper intake levels are not shown for micronutrients with the exception of salt, given that we were primarily interested in the proportion of study participants who met the recommended intake, and because reported dietary intake did not include quantitative information about supplements; therefore, the likelihood that participants would exceed upper intake levels for micronutrients was very low. We do not include data on sugar intake, given that our reference database included only sucrose and could therefore not be compared with the NNR for all added sugars.
Analysis was performed separately for women and men. Due to the small sample of male controls, we only computed descriptive statistics for men, and did not conduct analyses to examine differences between male cases and controls. To examine differences in intake between female cases and controls, we used regression models. The Shapiro-Wilk test was used to assess the normality of the data and the assumptions for the regression models were adequately met. First we fitted linear regression models where the predictor was case-status (cases versus controls) and the outcomes were total energy, macro-, and micronutrients, with each outcome included in a separate model. The regression coefficients from these linear regression models represent the mean difference in intake between cases and controls. Second, we fitted logistic regression models to estimate odds ratios (OR), where the exposure was case-status and the outcome was adherence to the NNR for total energy and each nutrient included in separate models. The ORs are interpreted as the ratio between the odds of adherence to the NNR between cases and controls. Then we fitted the same linear and logistic models while adjusting for age, BMI, and total energy intake.
Finally, we compared the total energy and macronutrient intake of four groups of female cases with different frequencies of self-reported binge-eating episodes in the past 28 days from a subset of case women who completed the EDE-Qv4. We first grouped the participants into those reporting no binge-eating episodes, and those reporting under and above the diagnostic threshold for BN and BED (≥4 times in the past 28 days, i.e., at least once per week). In the group reporting above the threshold, we evaluated the distribution of the number of binge-eating episodes and identified additionally appropriate groups. We used linear regression models to compare intake across groups, where the group with no binge-eating episodes was used as the referent. The models were adjusted for current BMI and age.
We tested whether removal of over- and under reporters substantively changed results. To correct for multiple comparisons when analyzing group differences the False Discovery Rate (FDR) procedure was applied and q-values are presented (i.e., p-values adjusted by FDR) (25). The significance level was set at q<0.05.
RESULTS
Table 1 presents the descriptive statistics for age and BMI values for cases and controls, by gender. Female cases were slightly younger than female controls (28.2 years ± 6.9 vs. 30.7 years ± 7.9 years, respectively, q<0.001). The female cases had higher current BMI (26.0 ± 6.2 vs. 24.7 ± 4.1) and lifetime highest BMI (29.2 ± 6.8 vs. 26.3 ± 4.5) than controls (q<0.001 for both), as well as lower lifetime lowest BMI (20.6 ± 4.6 vs. 21.6 ± 2.7, q<0.001).
Table 1.
Means and standard deviations (SD) of age and BMI variables of cases with binge-type eating disorders (BN and BED), and controls, by gender.
| Women | Men | ||||
|---|---|---|---|---|---|
| Cases | Controls | Cases | Controls | ||
| N=391 | N= 1213 | q-value | N= 39 | N= 14 | |
| Age years | 28.2 (6.9) | 30.7 (7.9) | <0.001 | 28.9 (7.3) | 35.7 (8.4) |
| Current BMI kg/m2 | 26.0 (6.2) | 24.7 (4.1) | <0.001 | 26.1 (6.1) | 25.8 (4.2) |
| Lowest BMI kg/m2 | 20.6 (4.6) | 21.6 (2.7) | <0.001 | 20.4 (3.5) | 22.9 (4.3) |
| Highest BMI kg/m2 | 29.2 (6.8) | 26.3 (4.5) | <0.001 | 30.1 (6.5) | 27.6 (4.4) |
T-tests evaluating differences between cases and controls were conducted in women only. The False Discovery Rate (FDR) procedure was applied and q-values represent FDR-adjusted p-values. Q-values are p-values corrected for multiple testing by False Discovery Rate (FDR) procedure
Total energy intake
Mean intake and the proportion of individuals who adhered to the total energy recommendations in the NNR are presented in Table 2 by gender and age. Total mean energy intake was 2,536.8 ± 1,182.2 kcal among younger female cases aged 18-30, for whom recommended intake ranges from 2,000 to 2,500 kilocalories per day; and 2,708.6 ± 1,121.6 kcal among older female cases aged 31-51, for whom the recommended intake range is 1,800 to 2,400 kilocalories per day. A numerically greater proportion of female cases than controls overconsumed relative to recommendations (39.3% of cases and 28.0% of controls aged 18-30, and 51.3% of cases and 31.4% of controls aged 31-51, data not shown). However, a substantial proportion of women in all groups reported underconsuming relative to recommendations, especially younger women aged 18-30 (34.2% of cases and 50.1% of controls).
Table 2.
Mean (SD) intake of energy, macronutrients, and micronutrients, and proportion who met the Nordic Nutrition Recommendations, among female and male cases and controls.
| Recommendations in the NNR | Recommended level (NNR) | Cases (n=430) | Controls (n=1,227) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | % adherence to NNR | N | Mean (SD) | % adherence to NNR | |||||
| Total energy (kcal) | Women 18-30 |
2000-2500§ | 272 | 2536.8 (1182.2) | 26.5 | 668 | 2174.5 (855.8) | 21.9 | ||
| Women 31-51 |
1800-2400 | 119 | 2708.6 (1121.6) | 33.6 | 545 | 2169.2 (863.2) | 30.6 | |||
| Men 18-30 |
2500-3200§ | 25 | 2555.3 (1019.3) | 16.0 | 4 | 2949.0 (853.6) | 25.0 | |||
| Men 31-45 |
2300-3000 | 14 | 2869.3 (1296.5) | 21.4 | 10 | 2504.6 (907.3) | 30.0 | |||
| Mean (SD) | % adherence to NNR | Mean (SD) | % adherence to NNR | |||||||
| Fat | ||||||||||
| Total fat (%E) | Women | 25-40 | 31.9 (6.3) | 79.6 | 33.1 (5.0) | 88.6 | ||||
| Men | 25-40 | 31.6 (7.2) | 64.3 | 32.7 (4.3) | 85.7 | |||||
| Saturated fat (%E) | Women | ≤10 | 12.0 (3.5) | 26.4 | 12.5 (2.7) | 16.2 | ||||
| Men | ≤10 | 11.9 (4.0) | 33.3 | 12.8 (2.8) | 21.4 | |||||
| Monounsaturated fat (%E) | Women | 10-20 | 11.7 (2.7) | 73.6 | 12.3 (2.1) | 88.3 | ||||
| Men | 10-20 | 11.6 (3.0) | 71.4 | 11.9 (1.3) | 92.9 | |||||
| Polyunsaturated fat (%E) | Women | 5-10 | 5.2 (1.5) | 46.5 | 5.2 (1.1) | 50.3 | ||||
| Men | 5-10 | 5.1 (1.4) | 45.2 | 5.2 (1.3) | 50.0 | |||||
| Omega-3 fatty acids (%E) | Women | ≥1 | 0.6 (0.6) | 13.3 | 0.5 (0.4) | 9.6 | ||||
| Men | ≥1 | 0.6 (0.4) | 16.7 | 0.5 (0.3) | 7.1 | |||||
| Protein | ||||||||||
| Total protein (%E) | Women | 10-20 | 15.9 (3.7) | 87.4 | 16.6 (2.7) | 91.2 | ||||
| Men | 10-20 | 15.4 (3.5) | 85.7 | 16.6 (1.5) | 100 | |||||
| Carbohydrates | ||||||||||
| Total carbohydrates (%E) | Women | 45-60 | 49.2 (8.4) | 63.1 | 47.6 (6.5) | 66.6 | ||||
| Men | 45-60 | 49.9 (9.0) | 61.9 | 48.1 (5.0) | 85.7 | |||||
| Dietary fiber (g/d) | Women | ≥25 | 33.4 (21.8) | 64.8 | 26.1 (12.9) | 44.4 | ||||
| Men | ≥25 | 35.6 (25.0) | 69.0 | 28.6 (10.7) | 64.3 | |||||
| Vitamins | ||||||||||
| Vitamin A (μg RE/d) | Women | ≥700 | 1067.2 (621.0) | 68.8 | 860.3 (466.4) | 60.3 | ||||
| Men | ≥900 | 977.7 (537.8) | 54.8 | 892.4 (430.9) | 50.0 | |||||
| Vitamin B1/Thiamine (mg/d) | Women | ≥1.1 | 1.6 (0.9) | 71.4 | 1.4 (0.6) | 60.9 | ||||
| Men | ≥1.4 | 1.6 (1.0) | 59.5 | 1.6 (0.6) | 64.3 | |||||
| Vitamin B2/Riboflavin (mg/d) | Women | ≥1.3 | 1.9 (1.1) | 72.6 | 1.6 (0.8) | 61.0 | ||||
| Men | ≥1.7 | 1.9 (1.1) | 53.8 | 1.9 (0.7) | 64.3 | |||||
| Vitamin B3/Niacin (NE/d) | Women | ≥15 | 43.6 (23.2) | 96.2 | 38.6 (16.4) | 98.0 | ||||
| Men | ≥19 | 42.0 (21.8) | 90.5 | 47.1 (16.4) | 100 | |||||
| Vitamin B6 (mg/d) | Women | ≥1.2 | 2.2 (1.0) | 88.4 | 1.9 (0.7) | 84.3 | ||||
| Men | ≥1.5 | 2.2 (1.1) | 84.6 | 2.2 (0.6) | 92.9 | |||||
| Vitamin B9/Folate (μg/d) | Women | ≥400 | 433.1 (215.4) | 48.5 | 348.2 (157.6) | 30.4 | ||||
| Men | ≥300 | 429.0 (180.8) | 76.7 | 351.9 (134.1) | 64.3 | |||||
| Vitamin B12 (μg/d) | Women | ≥2.0 | 4.6 (3.2) | 81.7 | 4.3 (2.4) | 86.2 | ||||
| Men | ≥2.0 | 4.5 (2.7) | 81.0 | 5.1 (2.0) | 100 | |||||
| Vitamin C (mg/d) | Women | ≥75 | 89.1 (51.9) | 54.8 | 80.2 (45.4) | 48.4 | ||||
| Men | ≥75 | 89.2 (49.0) | 50.0 | 76.3 (29.4) | 50.0 | |||||
| Vitamin D (μg/d) | Women | ≥10 | 5.6 (3.9) | 10.8 | 5.3 (3.1) | 6.8 | ||||
| Men | ≥10 | 5.8 (3.7) | 9.5 | 5.9 (2.5) | 14.3 | |||||
| Vitamin E (α-TE/d) | Women | ≥8 | 14.9 (7.0) | 88.7 | 12.9 (5.4) | 82.7 | ||||
| Men | ≥10 | 14.9 (6.9) | 71.4 | 13.7 (4.6) | 78.6 | |||||
| Minerals | ||||||||||
| Calcium Ca (mg/d) | Women | ≥800 | 1109.0 (648.8) | 67.1 | 915.7 (470.7) | 53.4 | ||||
| Men | ≥800 | 1082.6 (564.1) | 66.7 | 1172.5 (506.5) | 78.6 | |||||
| Phosphorus P (mg/d) | Women | ≥600 | 1775.5 (910.6) | 97.5 | 1525.0 (654.5) | 98.2 | ||||
| Men | ≥600 | 1763.8 (832.7) | 95.2 | 1829.8 (627.3) | 100 | |||||
| Magnesium Mg (mg/d) | Women | ≥280 | 479.3 (229.7) | 88.2 | 391.6 (153.4) | 77.6 | ||||
| Men | ≥350 | 491.3 (149.2) | 73.8 | 440.3 (149.2) | 78.6 | |||||
| Potassium K (mg/d) | Women | ≥3100 | 3574.4 (1503.5) | 60.3 | 3071.7 (1112.0) | 43.3 | ||||
| Men | ≥3500 | 3555.3 (1326.4) | 45.2 | 3491.2 (1046.4) | 50.0 | |||||
| Iron Fe (mg/d) | Women | ≥15 | 15.3 (8.4) | 40.5 | 12.5 (5.7) | 25.3 | ||||
| Men | ≥9 | 15.7 (8.6) | 83.3 | 13.8 (5.4) | 85.7 | |||||
| Zinc Zn (mg/d) | Women | ≥7 | 15.4 (8.3) | 92.2 | 12.9 (5.7) | 90.6 | ||||
| Men | ≥9 | 14.9 (7.2) | 88.1 | 15.7 (5.3) | 100 | |||||
| Selenium Se (μg/d) | Women | ≥50 | 55.2 (32.2) | 48.1 | 48.9 (23.5) | 40.2 | ||||
| Men | ≥60 | 55.9 (29.8) | 37.2 | 51.6 (15.9) | 21.4 | |||||
| Iodine I (μg/d) | Women | ≥150 | 267.4 (133.2) | 84.2 | 237.9 (105.8) | 83.5 | ||||
| Men | ≥150 | 255.6 (100.6) | 88.1 | 251.2 (85.5) | 92.9 | |||||
| Copper Cu (mg/d) | Women | ≥0.9 | 1.0 (0.6) | 53.5 | 0.8 (0.4) | 33.0 | ||||
| Men | ≥0.9 | 1.1 (0.5) | 66.7 | 0.8 (0.3) | 21.4 | |||||
| Salt (g/d) | Women | ≤6 | 8.6 (4.5) | 25.9 | 7.7 (3.2) | 34.5 | ||||
| Men | ≤6 | 8.5 (4.2) | 23.8 | 9.3 (3.4) | 0 | |||||
Female cases in both age groups reported statistically significantly higher intake of mean total daily energy than controls, even after adjustment for age and BMI (Table 3). The difference was substantial in both age groups, but was larger among older women (adjusted regression coefficient 437.18 kcal [95% CI [252.87; 621.49], q<0.001). However, the ORs for adherence to total energy recommendations among female cases as compared to controls did not reach statistical significance (Table 4).
Table 3.
Regression coefficients (β) with corresponding 95%CI from crude and adjusted regression models comparing female cases (n=391) to female controls (n=1,213) on mean intake of each nutrient, with female controls as the reference group.
| Recommendations in the NNR | Crude β estimate (95% CI) | q-value | Adjusted β estimate (95% CI) | q-value |
|---|---|---|---|---|
| Total energy (kcal) age 18-30; n=272 cases, n=668 controls | 362.30 (226.57; 5498.02) | <0.001 | 357.01 (220.89; 493.12) | <0.001 |
| Total energy (kcal) age 31-60; n=119 cases, n=545 controls | 539.40 (357.69; 721.11) | <0.001 | 437.18 (252.87; 621.49) | <0.001 |
| Fat | ||||
| Total fat (%E) | −1.31 (−1.91, −0.71) | <0.001 | −0.89 (−1.48, −0.30) | 0.006 |
| Saturated fat (%E) | −0.49 (−0.81, −0.16) | 0.007 | −0.40 (−0.73, −0.07) | 0.027 |
| Monounsaturated fat (%E) | −0.67 (−0.92, −0.42) | <0.001 | −0.48 (−0.73, −0.23) | <0.001 |
| Polyunsaturated fat (%E) | −0.06 (−0.20, 0.07) | 0.399 | 0.06 (−0.08, 0.19) | 0.450 |
| Omega-3 fatty acids (%E) | 0.05 (−0.01, 0.10) | 0.113 | −0.03 (−0.07, 0.02) | 0.332 |
| Protein | ||||
| Total protein (%E) | −0.73 (−1.07, −0.40) | <0.001 | −0.61 (−0.95, −0.27) | <0.001 |
| Carbohydrates | ||||
| Carbohydrates (%E) | 1.78 (1.00, 2.56) | <0.001 | 1.25 (0.47, 2.03) | 0.003 |
| Dietary fiber (g/d) | 6.80 (5.18, 8.41) | <0.001 | 2.17 (1.17, 3.10) | <0.001 |
| Vitamins | ||||
| Vitamin A (μg RE/d) | 212.50 (154.95, 270.04) | <0.001 | 115.06 (68.19, 166.22) | <0.001 |
| Vitamin B1/Thiamine (mg/d) | 0.19 (0.12, 0.27) | <0.001 | −0.05 (−0.08, −0.02) | 0.007 |
| Vitamin B2/Riboflavin (mg/d) | 0.29 (0.20, 0.39) | <0.001 | 0.02 (−0.04, 0.07) | 0.578 |
| Vitamin B3/Niacin (RE/d) | 4.69 (2.71, 6.67) | <0.001 | −1.38 (−2.50, −0.27) | 0.026 |
| Vitamin B6 (mg/d) | 0.32 (0.23, 0.41) | <0.001 | 0.06 (0.01, 0.10) | 0.040 |
| Vitamin B9/Folate (μg/d) | 85.13 (65.83, 104.43) | <0.001 | 41.74 (27.61, 55.87) | <0.001 |
| Vitamin B12 (μg/d) | 0.34 (0.05, 0.63) | 0.037 | −0.39 (−0.60, −0.18) | <0.001 |
| Vitamin C (mg/d) | 9.84 (4.50, 15.17) | <0.001 | 2.94 (−2.09, 7.97) | 0.306 |
| Vitamin D (μg/d) | 0.29 (−0.08, 0.65) | 0.158 | −0.58 (−0.84, −0.31) | <0.001 |
| Vitamin E (α-TE/d) | 1.98 (1.34, 2.62) | <0.001 | 0.33 (−0.07, 0.72) | 0.143 |
| Minerals | ||||
| Calcium Ca (mg/d) | 194.19 (136.80, 251.57) | <0.001 | 29.22 (−6.56, 65.00) | 0.150 |
| Phosphorus P (mg/d) | 244.28 (166.03, 322.53) | <0.001 | −17.33 (−48.61, 13.95) | 0.331 |
| Magnesium Mg (mg/d) | 84.92 (66.28, 103.55) | <0.001 | 27.69 (19.51, 35.88) | <0.001 |
| Potassium K (mg/d) | 493.94 (361.93, 625.96) | <0.001 | 128.46 (58.14, 198.79) | <0.001 |
| Iron Fe (mg/d) | 2.69 (2.00: 3.37) | <0.001 | 0.54 (0.20, 0.89) | 0.004 |
| Zinc Zn (mg/d) | 2.41 (1.72, 3.09) | <0.001 | 0.25 (−0.07, 0.56) | 0.168 |
| Selenium Se (μg/d) | 6.40 (3.51, 9.30) | <0.001 | −0.11 (−2.36, 2.14) | 0.951 |
| Iodine I (μg/d) | 28.76 (15.99, 41.52) | <0.001 | 0.27 (−9.60, 10.13) | 0.958 |
| Copper Cu (mg/d) | 0.23 (0.19, 0.28) | <0.001 | 0.12 (0.09, 0.15) | <0.001 |
| Salt (g/d) | 0.89 (0.51, 1.26) | <0.001 | −0.43 (−0.59, −0.26) | <0.001 |
Abbreviations: RE: Retinol Equivalents, 1 RE=1 μg retinol=12 μg ß-carotene, α-TE: α-Tocopherol Equivalents; 1 α-TE=1 mg RRR-α-tocopherol, NE: Niacin Equivalents, 1 NE=1 mg niacin=60 mg tryptophan
All adjusted models included age, BMI, and energy intake/day as potential confounders. β regression coefficients from linear regression models represent the mean difference in intakes between cases and controls.
The False Discovery Rate (FDR) procedure was applied and q-values represent FDR-adjusted p-values. The significance level was set at q=0.05.
Table 4.
Odds ratios (OR) with corresponding 95%CI from crude and adjusted regression models comparing female cases (n=391) to female controls (n=1,213) on the proportion who adhered to the recommended intake of each nutrient, with female controls as the reference group.
| Recommendations in the NNR | Crude OR (95% CI) | q-value | Adjusted OR (95% CI) | q-value |
|---|---|---|---|---|
| Total energy (kcal) age 18-30; n=272 cases, n=668 controls | 1.29 (0.93; 1.78) | 0.167 | 1.30 (0.93; 1.80) | 0.155 |
| Total energy (kcal) age 31-60; n=119 cases, n=545 controls | 1.29 (0.93; 1.78) | 0.167 | 1.30 (0.93; 1.80) | 0.155 |
| Fat | ||||
| Total fat (%E) | 0.52 (0.38, 0.70) | <0.001 | 0.48 (0.35, 0.66) | <0.001 |
| Saturated fat (%E) | 2.36 (1.78, 3.12) | <0.001 | 2.21 (1.65, 2.95) | <0.001 |
| Monounsaturated fat (%E) | 0.37 (0.28, 0.50) | <0.001 | 0.41 (0.30, 0.54) | <0.001 |
| Polyunsaturated fat (%E) | 0.88 (0.70, 1.10) | 0.320 | 1.03 (0.82, 1.31) | 0.828 |
| Omega-3 fatty acids (%E) | 1.45 (1.02, 2.05) | 0.057 | 0.99 (0.66, 1.46) | 0.958 |
| Protein | ||||
| Total protein (%E) | 0.70 (0.49, 1.02) | 0.081 | 0.64 (0.45, 0.94) | 0.035 |
| Carbohydrates | ||||
| Carbohydrates (%E) | 0.89 (0.70, 1.13) | 0.398 | 0.81 (0.63, 1.03) | 0.125 |
| Dietary fiber (g/d) | 2.46 (1.94, 3.13) | <0.001 | 2.07 (1.51, 2.83) | <0.001 |
| Vitamins | ||||
| Vitamin A (μg RE/d) | 1.86 (1.46, 2.39) | <0.001 | 1.55 (1.16, 2.08) | 0.005 |
| Vitamin B1/Thiamine (mg/d) | 1.54 (1.34, 2.22) | <0.001 | 0.88 (0.59, 1.31) | 0.565 |
| Vitamin B2/Riboflavin (mg/d) | 1.78 (1.39, 2.31) | <0.001 | 1.14 (0.80, 1.62) | 0.516 |
| Vitamin B3/Niacin (RE/d) | 0.64 (0.28, 1.59) | 0.360 | 0.43 (0.14, 1.36) | 0.174 |
| Vitamin B6 (mg/d) | 1.77 (1.22, 2.23) | 0.006 | 1.08 (0.66, 1.83) | 0.810 |
| Folate (μg/d) | 2.20 (1.75, 2.78) | <0.001 | 1.97 (1.50, 2.60) | <0.001 |
| Vitamin B12 (μg/d) | 0.77 (0.56, 1.05) | 0.137 | 0.48 (0.33, 0.70) | <0.001 |
| Vitamin C (mg/d) | 1.33 (1.06, 1.68) | 0.025 | 1.11 (0.86, 1.42) | 0.478 |
| Vitamin D (μg/d) | 1.57 (1.05, 2.32) | 0.040 | 0.68 (0.38, 1.17) | 0.214 |
| Vitamin E (α-TE/d) | 2.01 (1.39, 2.98) | <0.001 | 1.48 (0.92, 2.43) | 0.150 |
| Minerals | ||||
| Calcium Ca (mg/d) | 1.84 (1.45, 2.35) | <0.001 | 1.26 (0.92, 1.73) | 0.188 |
| Phosphorus P (mg/d) | 2.11 (0.58, 13.51) | 0.381 | 1.31 (0.23, 11.21) | 0.827 |
| Magnesium Mg (mg/d) | 0.37 (0.25, 0.53) | <0.001 | 0.39 (0.23, 0.66) | 0.001 |
| Potassium K (mg/d) | 2.04 (1.62, 2.58) | <0.001 | 1.71 (1.22, 2.39) | 0.003 |
| Iron Fe (mg/d) | 2.06 (1.62, 2.61) | <0.001 | 1.60 (1.09, 2.35) | 0.027 |
| Zinc Zn (mg/d) | 1.63 (1.03, 1.72) | 0.069 | 1.03 (0.50, 2.23) | 0.953 |
| Selenium Se (μg/d) | 1.46 (1.16, 1.83) | 0.003 | 0.97 (0.72, 1.29) | 0.855 |
| Iodine I (μg/d) | 1.23 (0.89, 1.72) | 0.277 | 0.71 (0.48, 1.07) | 0.143 |
| Copper Cu (mg/d) | 2.44 (1.93, 3.08) | <0.001 | 2.25 (1.68, 3.03) | <0.001 |
| Salt (g/d) | 0.60 (0.46, 0.78) | <0.001 | 1.35 (0.90, 2.04) | 0.184 |
Abbreviations: OR, Odds ratio, RE: Retinol Equivalents, 1 RE=1 μg retinol=12 μg ß-carotene, α-TE: α-Tocopherol Equivalents; 1 α-TE=1 mg RRR-α-tocopherol, NE: Niacin Equivalents, 1 NE=1 mg niacin=60 mg tryptophan
All adjusted models included age, BMI, and energy intake/day as potential confounders. ORs for total energy, total fat, monounsaturated fat, polyunsaturated fat, total protein, and total carbohydrates compare the odds of adhering to minimum recommended intake levels and not exceeding upper intake levels between cases and controls. ORs for saturated fat and salt compare the odds of not exceeding recommended upper intake levels between cases and controls. ORs for omega-3 fatty acids, fiber, and all micronutrients except salt compare the odds of meeting minimum recommended intake levels between cases and controls.
The False Discovery Rate (FDR) procedure was applied and q-values represent FDR-adjusted p-values. The significance level was set at q=0.05.
For all groups of men, total daily energy intake was within recommended levels. However, standard deviations were large, indicating both over- and underconsumption of total energy by some individuals in all groups. Adherence to total energy recommendations was numerically lower for case than control men in both age groups. 64.0% of younger case men aged 18-30 underconsumed relative to total energy recommendations, whereas 42.9% of older case men aged 31-45 overconsumed relative to recommendations.
Macronutrient intake
The mean intake of macronutrients expressed as a percent of energy coming from fat, protein and carbohydrates, as well as the proportion of individuals who adhered to recommendations, are shown in Table 2, by gender. Individuals in all groups met recommendation mean intake for all macronutrients, except for saturated fat (too high) and omega-3-fatty acids (too low). A greater proportion of female cases than controls adhered to the recommendation to maintain a saturated fat intake at or below 10% of total energy, although the proportion of individuals who adhered to upper intake levels for saturated fat was low in all groups (male and female cases and controls). Although greater proportions of female cases compared with controls met the NNR for omega-3-fatty acids, adherence was low among all groups. Only 13.3% of case women and 9.6% of control women met the recommendation for omega-3-fatty acids.
Mean intake and the proportion of individuals who adhered to the fiber recommendation of 25 grams per day were higher among female cases compared to controls, and the difference in the proportion of women adhering to recommendations was large (64.8% among cases vs. 44.4% among controls).
According to age- and BMI-adjusted regression models, female cases had slightly lower intake of percent total fat, saturated fat, and monounsaturated fat, as well as protein, but higher intake of percent carbohydrate, compared with controls. Although statistically significant, all covariate-adjusted β coefficients comparing mean intake of these nutrients were < 1.5, Table 3). In the adjusted regression model comparing adherence to fiber recommendations between female cases and controls, the magnitude of the differences was attenuated but remained statistically significant (adjusted OR 2.17 [95%CI 1.17, 3.10], q<0.001 Table 4).
The adjusted OR comparing the odds of adhering to the saturated fat recommendation between female cases and controls was 2.21 [95%CI 1.65, 2.95], q<0.001. Among women, the age- and BMI-adjusted differences in mean intake and adherence to the omega-3 fatty acid recommendations between cases and controls did not reach statistical significance.
Micronutrient intake
The mean intake of micronutrients, including vitamins and minerals, and the proportion of individuals who adhered to the recommended intake levels are presented in Table 2. Mean intake did not reach the recommended levels for vitamin D among any of the groups. Among women, only 10.2% of cases and 6.8% of controls met the recommendation. Among men, 7.7% of cases and 14.3% of controls met the recommendation. The mean intake of all groups exceeded recommendations for salt, and the proportion of individuals who adhered to the recommendation was low for all groups. A greater proportion of control compared to case women adhered to the salt recommendation (23.5% and 33.9% among case and control women, respectively).
The majority of female cases and controls did not consume adequate amounts of folate, iron, or selenium, although female cases but not controls achieved adequate mean intake. Additionally, the majority of female controls did not achieve the recommended intake of potassium or copper. Neither male cases nor controls met mean intake recommendations for selenium. The majority of male controls did not achieve the recommended intake levels for potassium and copper, and half did not meet the recommendation for vitamin A.
According to the results of adjusted models, female cases had statistically significantly higher intake of vitamins A, B6, B9 (folate), magnesium, potassium, iron, copper, but lower intake of vitamin B1, B3, B12, D, and salt, compared with female controls (Table 3). Differences were substantively small, except for Vitamin A, folate, and potassium, for which female cases reported consuming 115.06 more μg RE/d (95% CI 68.19; 166.22); 41.74 more μg/d (95% CI 27.61, 55.87); and 128.46 more mg/day (95% CI 58.14; 198.79), respectively, compared with controls (all q<0.001). The difference in the odds of adherence to salt intake recommendations was no longer statistically significantly different between female cases and controls after adjustment for age, BMI, and total energy intake.
Binge Eating Frequency: Energy and Macronutrient Intake
EDE-Qv4 data were available for 365 female cases. Evaluation of the distribution of binge-eating frequencies in the past 28 days led to identification of the following groups: 1) no binge-eating episodes (n=115), 2) 1-3 episodes (n=73), 3) 4-10 episodes (n=98), and 4) 11 or more episodes (n=79) (Figure 1). Age and BMI-adjusted models revealed higher intake of total energy and percent carbohydrates and lower intake of percent fat among female cases with ≥4-10 or ≥11 reported binge-eating episodes compared to female cases with no binge-eating episodes. Female cases with ≥4-10 reported binge-eating episodes consumed 361.4 more kcal (95% CI 48.1; 674.7, q=0.04); and female cases with ≥11 reported binge-eating episodes reported consuming 806.4 more kcal (95% CI 467.8; 1145.0, q<0.001) than cases with no binge-eating episodes (Figure 1a). There was a trend towards increased total daily energy intake among female cases reporting 1-3 binge-eating episodes compared with cases reporting no binge-eating episodes that did not reach statistical significance (351.5 kcal [95% CI 12.1; 691.0, q=0.063]). Differences in percent carbohydrate and fat intake were small (Figure 1b).
Figure 1.
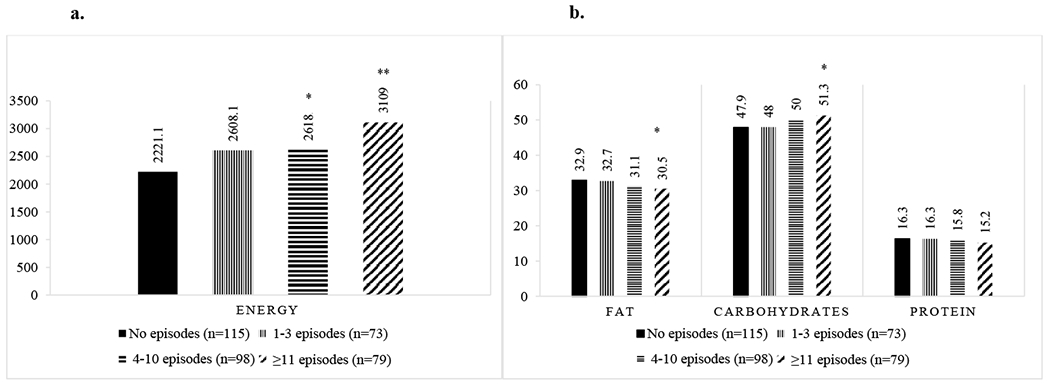
Mean intake is presented for energy (Figure 1a) and percent energy from macronutrients (Figure 1b) among a subset of female cases for whom EDE-Qv4 data were available, with different frequencies of binge-eating episodes in the past 28 days (n=365). The group reporting no episodes in the past 28 days was used as the reference and differences in intakes according to binge-eating frequency were examined using linear regression models adjusted for age and BMI.
* q<0.05
** q<0.001
DISCUSSION
In this large case-control comparison of individuals with and without binge-type eating disorders, we found, in line with previous literature, that women with binge-type eating disorders, especially older women, had higher intake of total energy per day compared to controls and higher than recommendations (2–5). We observed a strong and positive relationship between the number of recent binge-eating episodes and total intake of calories among female cases, suggesting the urgent need for dietary intervention among patients exhibiting heightened eating disorder symptomatology. Sustained excess intake of energy, even if numerically small on a daily basis, cumulatively can lead to weight gain and associated metabolic risk if energy balance is not maintained (26). Longitudinal studies are needed to confirm whether the observed phenomenon of excess caloric intake in women with binge-type eating disorders persists over time. Importantly, nutritional counseling for individuals with current or past eating disorders should avoid interventions that could trigger or exacerbate eating disorder symptoms (e.g., caloric restriction for weight loss) (27). If weight management is indicated, a focus on health promoting behaviors such as an overall healthful dietary pattern, intuitive eating approaches, and moderate levels of regular exercise may be recommended for individuals with a current or historical diagnosis of an eating disorder to avoid potential relapse (28).
To the best of our knowledge, this is the first study to describe nutrient intake in men with eating disorders. Although our sample was small and results should be interpreted with caution, we found that younger case men had insufficient caloric intake. Some, but not all, prior studies suggest that men may be more likely to underreport energy intake than women (29, 30). Larger, adequately powered studies assessing dietary intake among men with binge-type eating disorders are needed to confirm our findings, which raise the possibility that recommended intake of key macro- and micronutrients needed to promote optimal health are not being met by men with binge-type eating disorders. Public health and individualized clinical recommendations must balance the need to maintain energy balance while achieving minimum intake for nutrients of concern.
Macronutrients
Mean macronutrient intake in women and men with binge-type eating disorders was adequate, except in the case of excess saturated fat and inadequate omega-3 fatty acid consumption. Although the purported detrimental health effects of excess saturated fat intake are still debated (31), it is well-established that consumption of essential omega-3 fatty acids is critical for numerous physiological processes, but is generally low among Western populations (32). A low ratio of omega-3 to omega-6 fatty acids may contribute to inflammation and insulin resistance (33). Public health messaging should continue to encourage substitution of animal (i.e., saturated) for unsaturated (i.e., plant-based polyunsaturated, including omega-3) fats to promote optimal health.
Female cases had a higher age- and energy-adjusted intake of percent carbohydrate, but lower adjusted intake of percent fat and protein, compared with female controls. However, differences were small. These results are in line with one prior study in which participants with BN reported increased carbohydrate intake compared to controls without BN (2), but contradictory to another study in which calorie and carbohydrate intake did not differ among individuals with BN or BED compared to controls without an eating disorder (34). These differences in outcomes may be attributable to variability in the method of dietary assessment (e.g., a computer program and daily food records). Future studies should confirm these results and examine the quality of carbohydrates consumed by individuals with binge-type eating disorders, given the variability of effects of simple compared to complex carbohydrate intake on blood glucose homeostasis (35).
Mean fiber intake was adequate for all groups and adherence to recommendations was high, although standard deviations were relatively large. Fiber intake is important for well-functioning gut motility. Since individuals with eating disorders often report gastrointestinal problems (15), adequate fiber intake is important to monitor during treatment if total energy intake per day is reduced (36). It is equally important to avoid excess fiber intake, which may contribute to feelings of bloating and raise body image concerns during the acute treatment phase.
Micronutrients
Individuals with binge-type eating disorders and control participants had adequate mean intake of all vitamins and minerals, except for excess salt and inadequate vitamin D. Excess salt intake may increase blood pressure and the risk of cardiovascular and kidney disease (37). This is particularly relevant to individuals with BN, who may be at higher long-term risk for cardiovascular disease and should therefore be cautioned regarding excessive intake of salt (38). Insufficient vitamin D intake results in low absorption of calcium and phosphorous, which may increase risk of osteopenia and osteoporosis (39). The basic vitamin D requirement can be satisfied by sun exposure; however, under Nordic living conditions, this cannot be accomplished during the winter season due to the high latitude. Efforts should be made to assure adequate intake of vitamin D-rich foods, including fatty fish and fortified dairy products. Supplementation may be recommended on an individual basis (e.g., for vegans).
The proportion of individuals who adhered to recommendations for folate and iron was low among female cases. In the case of selenium, adherence was low among both male and female cases. These findings mirrors those of a study of Swedish adult women of childbearing age (40), and underscore the need for dietary intervention to prevent anemia among women overall, and pregnancy complications and poor birth outcomes among women of reproductive age. These patterns were mirrored in both male and female controls, who, in addition, underconsumed copper. Selenium and copper are vital co-factors that participate in the body’s antioxidant defense systems (41). These micronutrients may be particularly critical to consume in the setting of binge-type eating disorders, where increased stress signals may trigger inflammation (42), resulting in a greater need for free radical neutralization.
Limitations
The findings of this study should be interpreted in light of limitations. First, case-control studies may be subject to selection bias, as cases are more likely to participate than eligible controls (43). Second, the small sample of males precluded inferential statistics, and descriptive comparisons among men should be interpreted with caution. Future studies should bolster recruitment of men—an understudied group in eating disorders. Generalizability of findings to the broader population of individuals with eating disorders may be further limited by the modest response rate of 27% for the larger BEGIN-SE study. All cases in BEGIN-SE were recruited from a register of treatment-seeking individuals who may not represent the general BN and BED population as many individuals do not seek treatment (44).
Third, although the MiniMeal-Q has been validated, we cannot rule out potential measurement error as FFQs commonly underestimate energy and nutrient intake (45). Self-reported dietary data are subject to underreporting, especially of foods considered to be unhealthy due to social desirability bias (46). We cannot rule out the possibility that case participants misreported dietary intake to a greater degree than healthy controls (47). However, we were able to detect statistically significant differences in both energy and nutrient intake between female cases and controls, suggesting that our dietary intake measure was sensitive to the observed differences. This is in line with the principle that FFQs may underestimate individual-level nutrient intake but that they provide reasonable estimates of intake at the population level, allowing for discrimination between groups (48). Future studies should assess nutrient intake during meals compared with binges, account for loss of nutrients via purging, and capture quantitative supplement intake (49). To reduce the risk of confounding bias, future studies should collect and adjust for sociodemographic variables such as smoking, education, and socioeconomic status. Individualized PAL in the estimation of energy requirements would produce more accurate estimates of effect.
We were unable to conduct subgroup analyses by eating disorder diagnosis, given that all but five case participants met criteria for lifetime diagnosis of both BED and BN. This is consistent with prior evidence that BN and BED have the highest comorbid lifetime prevalence of any two eating disorders, which makes comparisons between the two groups difficult to achieve (50).
CONCLUSION
Overall in this sample of individuals with binge-type eating disorders and healthy controls, the majority of female cases reported excess energy intake. At the macronutrient level, dietary intake appears to be appropriately balanced with respect to the major macronutrients. However, all groups reported consumption of percent saturated fats above recommended intake levels, and inadequate intake of omega-3 fatty acids, both of which influence cardiometabolic health (51).
With regard to micronutrients, low adherence to intake of folate and iron in both female cases and controls is of considerable concern as a large proportion of the women in this sample are of reproductive age. This represents a critical intervention point for women with binge-type eating disorders, but also for public health more broadly. Overall, the results demonstrating low intake of key micronutrients among both case and control women suggests a need for greater attention towards improving overall diet quality and avoidance of micronutrient deficiencies to lower risk of associated disorders.
Nutrition counseling strategies in the setting of binge-type eating disorders may include encouragement of appropriate energy balance, while maintaining a nutrient-dense dietary pattern. Nutrition counseling can and should form an important pillar of eating disorder treatment, not only to assist patients with normalizing eating patterns, but also to ensure that their diets are optimized for long term health benefits.
ACKNOWLEDGEMENTS
We thank Malin Rådström, Virpi Leppä, Peter Lind, Bengt Fundin, Emma Forsén Mantilla, Stina Borg, and the entire BEGIN-SE working group for all the work and effort put in to the BEGIN Sweden study.
FUNDING STATEMENT
Funding: This work was supported by the Swedish Research Council (VR Dnr: 538-2013-8864).
CMB is supported by NIMH (R01MH120170; R01MH124871; R01MH119084; R01MH118278; R01 MH124871); Brain and Behavior Research Foundation Distinguished Investigator Grant; Swedish Research Council (VR, award: 538-2013-8864); Lundbeck Foundation (Grant no. R276-2018-4581).
DI is supported by the Global Cardiometabolic Disease training grant (National Heart, Lung, and Blood Institute of the National Institutes of Health) awarded to the Department of Nutrition at the University of North Carolina at Chapel Hill, USA, under Award Number HL129969.
Footnotes
CONFLICTS OF INTEREST
CMB reports: Shire (grant recipient, Scientific Advisory Board member); Idorsia, consultant; Pearson (author, royalty recipient). No other authors have conflicts to disclose.
REFERENCES
- 1.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: 2013. [Google Scholar]
- 2.Alpers GW, Tuschen-Caffier B. Energy and macronutrient intake in bulimia nervosa. Eat Behav. 2004;5(3):241–9. [DOI] [PubMed] [Google Scholar]
- 3.Weltzin TE, Hsu LK, Pollice C, Kaye WH. Feeding patterns in bulimia nervosa. Biol Psychiatry. 1991;30(11):1093–110. [DOI] [PubMed] [Google Scholar]
- 4.Reeves RS, McPherson RS, Nichaman MZ, Harrist RB, Foreyt JP, Goodrick GK. Nutrient intake of obese female binge eaters. J Am Diet Assoc. 2001;101(2):209–15. [DOI] [PubMed] [Google Scholar]
- 5.Raymond NC, Neumeyer B, Warren CS, Lee SS, Peterson CB. Energy intake patterns in obese women with binge eating disorder. Obes Res. 2003;11(7):869–79. [DOI] [PubMed] [Google Scholar]
- 6.Yanovski SZ, Leet M, Yanovski JA, Flood M, Gold PW, Kissileff HR, et al. Food selection and intake of obese women with binge-eating disorder. Am J Clin Nutr. 1992;56(6):975–80. [DOI] [PubMed] [Google Scholar]
- 7.Sysko R, Devlin MJ, Walsh BT, Zimmerli E, Kissileff HR. Satiety and test meal intake among women with binge eating disorder. Int J Eat Disord. 2007;40(6):554–61. [DOI] [PubMed] [Google Scholar]
- 8.Engel SG, Kahler KA, Lystad CM, Crosby RD, Simonich HK, Wonderlich SA, et al. Eating behavior in obese BED, obese non-BED, and non-obese control participants: a naturalistic study. Behav Res Ther. 2009;47(10):897–900. [DOI] [PubMed] [Google Scholar]
- 9.Setnick J Micronutrient deficiencies and supplementation in anorexia and bulimia nervosa: a review of literature. Nutr Clin Pract. 2010;25(2):137–42. [DOI] [PubMed] [Google Scholar]
- 10.Nova E, Samartín S, Gómez S, Morandé G, Marcos A. The adaptive response of the immune system to the particular malnutrition of eating disorders. European Journal of Clinical Nutrition. 2002;56(3):S34–S7. [DOI] [PubMed] [Google Scholar]
- 11.Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia. The American Journal of Medicine. 2016;129(1):30–7. [DOI] [PubMed] [Google Scholar]
- 12.Dahlgren CL, Stedal K, Wisting L. A systematic review of eating disorder prevalence in the Nordic countries: 1994–2016. Nordic Psychology. 2018;70(3):209–27. [Google Scholar]
- 13.Nordic Council of Ministers. Nordic Nutrition Recommendations 2012. Integrating nutrition and physical activity. 5th ed. Copenhagen: Norden; 2014. [Google Scholar]
- 14.Swedish Association of Local Authorities and Regions. National Healthcare Quality Registries in Sweden. Stockholm: Edita; 2007. [Google Scholar]
- 15.Wiklund CA, Rania M, Kuja-Halkola R, Thornton LM, Bulik CM. Evaluating disorders of gut-brain interaction in eating disorders. Int J Eat Disord. 2021;54(6):925–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Möller E, Galeone C, Adami HO, Adolfsson J, Andersson TM, Bellocco R, et al. The Nordic Nutrition Recommendations and prostate cancer risk in the Cancer of the Prostate in Sweden (CAPS) study. Public Health Nutr. 2012;15(10):1897–908. [DOI] [PubMed] [Google Scholar]
- 17.Dratva J, Gómez Real F, Schindler C, Ackermann-Liebrich U, Gerbase MW, Probst-Hensch NM, et al. Is age at menopause increasing across Europe? Results on age at menopause and determinants from two population-based studies. Menopause. 2009;16(2):385–94. [DOI] [PubMed] [Google Scholar]
- 18.Christensen SE, Möller E, Bonn SE, Ploner A, Bälter O, Lissner L, et al. Relative validity of micronutrient and fiber intake assessed with two new interactive meal- and Web-based food frequency questionnaires. J Med Internet Res. 2014;16(2):e59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Christensen SE, Möller E, Bonn SE, Ploner A, Wright A, Sjölander A, et al. Two new meal- and web-based interactive food frequency questionnaires: validation of energy and macronutrient intake. J Med Internet Res. 2013;15(6):e109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Siega-Riz AM, Haugen M, Meltzer HM, Von Holle A, Hamer R, Torgersen L, et al. Nutrient and food group intakes of women with and without bulimia nervosa and binge eating disorder during pregnancy. Am J Clin Nutr. 2008;87(5):1346–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.National Food Agency. Food database [Swedish]. Available from: http://www7.slv.se/SokNaringsinnehall/. [
- 22.Thornton LM, Munn-Chernoff MA, Baker JH, Juréus A, Parker R, Henders AK, et al. The Anorexia Nervosa Genetics Initiative (ANGI): Overview and methods. Contemp Clin Trials. 2018;74:61–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fairburn CG, Beglin SJ. Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord. 1994;16(4):363–70. [PubMed] [Google Scholar]
- 24.R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2017. [Google Scholar]
- 25.Storey JD. A Direct Approach to False Discovery Rates. J R Stat Soc Series B Stat Methodol 2002;64(3):479–98. [Google Scholar]
- 26.Hall KD, Sacks G, Chandramohan D, Chow CC, Wang YC, Gortmaker SL, et al. Quantification of the effect of energy imbalance on bodyweight. Lancet (London, England). 2011;378(9793):826–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cardel MI, Newsome FA, Pearl RL, Ross KM, Dillard JR, Miller DR, et al. Patient-Centered Care for Obesity: How Healthcare Providers Can Treat Obesity While Actively Addressing Weight Stigma and Eating Disorder Risk. Journal of the Academy of Nutrition and Dietetics. 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.da Luz FQ, Swinbourne J, Sainsbury A, Touyz S, Palavras M, Claudino A, et al. Hapifed: A healthy approach to weight management and food in eating disorders: A case series and manual development. Journal of eating disorders. 2017;5(1):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bedard D, Shatenstein B, Nadon S. Underreporting of energy intake from a self-administered food-frequency questionnaire completed by adults in Montreal. Public Health Nutr. 2004;7(5):675–81. [DOI] [PubMed] [Google Scholar]
- 30.Stice E, Palmrose CA, Burger KS. Elevated BMI and Male Sex Are Associated with Greater Underreporting of Caloric Intake as Assessed by Doubly Labeled Water. J Nutr. 2015;145(10):2412–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Szajewska H, Szajewski T. Saturated Fat Controversy: Importance of Systematic Reviews and Meta-analyses. Crit Rev Food Sci Nutr. 2016;56(12):1947–51. [DOI] [PubMed] [Google Scholar]
- 32.Simopoulos AP. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients. 2016;8(3):128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Albracht-Schulte K, Kalupahana NS, Ramalingam L, Wang S, Rahman SM, Robert-McComb J, et al. Omega-3 fatty acids in obesity and metabolic syndrome: a mechanistic update. J Nutr Biochem. 2018;58:1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Segura-García C, De Fazio P, Sinopoli F, De Masi R, Brambilla F. Food choice in disorders of eating behavior: correlations with the psychopathological aspects of the diseases. Compr Psychiatry. 2014;55(5):1203–11. [DOI] [PubMed] [Google Scholar]
- 35.Sievenpiper JL. Low-carbohydrate diets and cardiometabolic health: the importance of carbohydrate quality over quantity. Nutr Rev. 2020;78(Suppl 1):69–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Riedlinger C, Schmidt G, Weiland A, Stengel A, Giel KE, Zipfel S, et al. Which Symptoms, Complaints and Complications of the Gastrointestinal Tract Occur in Patients With Eating Disorders? A Systematic Review and Quantitative Analysis. Front Psychiatry. 2020;11:195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rust P, Ekmekcioglu C. Impact of Salt Intake on the Pathogenesis and Treatment of Hypertension. Adv Exp Med Biol. 2017;956:61–84. [DOI] [PubMed] [Google Scholar]
- 38.Tith RM, Paradis G, Potter BJ, Low N, Healy-Profitós J, He S, et al. Association of Bulimia Nervosa With Long-term Risk of Cardiovascular Disease and Mortality Among Women. JAMA Psychiatry. 2020;77(1):44–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Holick MF. Optimal vitamin D status for the prevention and treatment of osteoporosis. Drugs Aging. 2007;24(12):1017–29. [DOI] [PubMed] [Google Scholar]
- 40.Becker W, Lindroos AK, Nälsén C, Warensjö Lemming E, Öhrvik V. Dietary habits, nutrient intake and biomarkers for folate, vitamin D, iodine and iron status among women of childbearing age in Sweden. Ups J Med Sci. 2016;121(4):271–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Battin EE, Perron NR, Brumaghim JL. The central role of metal coordination in selenium antioxidant activity. Inorg Chem. 2006;45(2):499–501. [DOI] [PubMed] [Google Scholar]
- 42.Black PH, Garbutt LD. Stress, inflammation and cardiovascular disease. J Psychosom Res. 2002;52(1):1–23. [DOI] [PubMed] [Google Scholar]
- 43.Hernán MA, Hernández-Díaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15(5):615–25. [DOI] [PubMed] [Google Scholar]
- 44.Austin A, Flynn M, Richards K, Hodsoll J, Duarte TA, Robinson P, et al. Duration of untreated eating disorder and relationship to outcomes: A systematic review of the literature. Eur Eat Disord Rev. 2021;29(3):329–45. [DOI] [PubMed] [Google Scholar]
- 45.Pérez Rodrigo C, Aranceta J, Salvador G, Varela-Moreiras G. Food frequency questionnaires. Nutr Hosp. 2015;31 Suppl 3:49–56. [DOI] [PubMed] [Google Scholar]
- 46.Macdiarmid J, Blundell J. Assessing dietary intake: Who, what and why of under-reporting. Nutr Res Rev. 1998;11(2):231–53. [DOI] [PubMed] [Google Scholar]
- 47.Bartholome LT, Peterson RE, Raatz SK, Raymond NC. A comparison of the accuracy of self-reported intake with measured intake of a laboratory overeating episode in overweight and obese women with and without binge eating disorder. Eur J Nutr. 2013;52(1):193–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Willett W, Lenart E . Reproducibility and validity of food-frequency questionnaires. Nutritional epidemiology. 2013;3. [Google Scholar]
- 49.Hadigan CM, LaChaussée JL, Walsh BT, Kissileff HR. 24-hour dietary recall in patients with bulimia nervosa. Int J Eat Disord. 1992;12(1):107–11. [Google Scholar]
- 50.Udo T, Grilo CM. Prevalence and Correlates of DSM-5-Defined Eating Disorders in a Nationally Representative Sample of U.S. Adults. Biol Psychiatry. 2018;84(5):345–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Elagizi A, Lavie CJ, O’Keefe E, Marshall K, O’Keefe JH, Milani RV. An Update on Omega-3 Polyunsaturated Fatty Acids and Cardiovascular Health. Nutrients. 2021;13(1). [DOI] [PMC free article] [PubMed] [Google Scholar]