

ABSTRACT
Refugees, immigrants, and migrants (RIM) in the United States (US) have been identified as an underimmunized population prior to the COVID-19 pandemic. Vaccine acceptance is critical to combat the public health threat incited by COVID-19 and other vaccine-preventable disease. To better understand escalating vaccine hesitancy among US RIM, a comprehensive evaluation of the problem and solutions is necessary. In this systematic review, we included 57 studies to describe vaccination rates, barriers, and interventions addressing vaccine hesitancy over the past decade. Meta-analysis was performed among 22 studies, concluding that RIM represent an underimmunized population compared to the general US population. Narrative synthesis and qualitative methods were used to identify critical barriers, including gaps in knowledge, poor access to medical care, and heightened distrust of the medical system. Our results demonstrate the need for effective, evidence-based interventions to increase vaccination rates among diverse RIM populations.
KEYWORDS: Vaccination, refugee, immigrant, migrant, systematic review, vaccine hesitancy
Introduction
Recent outbreaks of vaccine-preventable diseases (VPD) in the United States (US) reveal the critical need to combat vaccine hesitancy. The reemergence of measles and poliovirus, along with continued morbidity and mortality associated with COVID-19, emphasizes the necessity for increased vaccination efforts.1–4 The US is home to an increasingly global community, with over 44 million refugees, immigrants, and migrants (RIM).5 This global patient population carries risks for VPD from host countries, sociocultural and environmental influences that have significant impacts on their health.6 Low immunization rates have been reported within RIM communities, placing them at increased risk for VPD.7–9 This risk may be amplified during the COVID-19 pandemic amid rising vaccine hesitancy and health inequities that have been linked to a disproportionate burden of disease.10 The health of this global community directly impacts the health of the entire nation, emphasizing the need for an effective national public health response.
The increased vulnerability of RIM to VPD results from the combination of increased exposure to disease, as well as distinct barriers to vaccination.8 Hesitancy within the RIM population has previously been attributed to cultural norm barriers, poor access to medical care, knowledge gaps, and mistrust of institutions.8 Additional mistrust in the healthcare system and vaccine safety concerns have developed following the introduction of the COVID-19 vaccines.10,11 The ultimate impact of the COVID-19 pandemic on vaccine hesitancy among RIM, however, is yet to be determined. To fully understand the problem and effectively intervene, a timely understanding of vaccine hesitancy among RIM must be considered a public health priority.
While previous reviews have focused on select vaccines or a subset of the RIM community, a systematic review addressing vaccine hesitancy within the entire US RIM population is lacking. The inclusion of all RIM, in addition to the relevant inclusion of COVID-19 literature, distinguishes this review from previous work. To provide a comprehensive review of the problem and potential solutions, and to inform critical public health policy, this review has three objectives: 1) to quantify the burden by describing vaccination rates, 2) to identify key barriers to vaccination, and 3) to describe effective interventions addressing vaccine hesitancy in the RIM population within the US.
Materials and methods
Criteria for considering studies for review
Studies were considered for inclusion if they addressed one of the three primary objectives: 1) vaccination rates, 2) barriers to vaccination, or 3) interventions addressing vaccination among foreign-born individuals residing within the US. In addition, included studies were expected to meet the following criteria: 1) original research (randomized controlled trials (RCT), quasi-experimental studies, cohort studies, cross-sectional studies, and qualitative studies); 2) published between April 2012 and May 2022; 3) inclusion of adults 18 y and older; 4) inclusion of foreign-born individuals, including refugees, immigrants, migrants, and asylees, from all countries of origin resettling within the United States; and 5) conducted in English. Studies focusing on the perspective of the healthcare provider or children and adolescents alone were excluded. Non-original research pieces, such as case reports, case series, reviews, or perspectives, were also excluded.
Search strategy and article selection
The search strategy was developed in collaboration with an experienced medical librarian (ED) and conducted using the PubMed Medline electronic database. The following search term combination was used on two occasions during May 2022:
(Vaccin* OR immunization OR vaccines[mh] OR vaccination[mh] OR vaccination hesitancy[mh] OR vaccination refusal[mh] OR immunization programs[mh] OR vaccination coverage[mh] OR immunization[mh])
AND
(Immigrants OR migrants OR refugees OR asylum OR foreign-born OR internally displaced OR transients and migrants[mh] OR emigrants and immigrants[mh] OR refugees[mh] OR undocumented immigrants[mh] OR emigration and immigration[mh])
Additional review through “similar articles” and manual review of included references were used to identify potentially relevant literature.
Data collection and analysis
Selection of studies
Initial search results were screened to determine relevance based on prespecified inclusion/exclusion criteria. Following initial screening, potential articles were uploaded into Covidence, a web-based software system, for additional screening, extraction, and quality assessment.12 Two authors independently completed title, abstract, and full-text screening using Covidence. Disagreements were settled through consensus.
Data extraction and quality assessment
Data were independently extracted in duplication using a standardized data abstraction form. The data abstraction form was previously described by Rani et al.13 and included general publication data, methodology, and information regarding participants and outcomes.
Quality assessment for observational studies was performed using the National Institutes of Health (NIH) tools for the assessment of the risk of bias, while qualitative studies were assessed using the Critical Appraisal Skills Programme (CASP) qualitative study checklist.14,15
Two reviewers independently assessed each of the included studies for risk of bias. The questions provided by these tools allowed the reviewer to critically appraise each study, focusing on key concepts to evaluate the internal validity of a study and identify potential risk for bias. The quality of each quantitative article was deemed to be “good,” “fair,” or “poor” following reflection and consensus among reviewers.14 Although studies were not excluded on the basis of these scores, study quality was considered when synthesizing and interpreting results.
Data synthesis
We sought to provide a comprehensive review of vaccine hesitancy within the RIM population by addressing three domains: the burden, barriers, and interventions to overcome vaccine hesitancy. We describe the methods for each of these objectives below.
To address the burden, we compared vaccination rates for the RIM population to the US-born population. For vaccines with two or more eligible studies, we pooled the data with the help of meta-analysis using Review Manager 5 (RevMan) software 5.4.16 Dichotomous outcomes were pooled to obtain an odds ratio with a 95% confidence interval (CI). To account for significant heterogeneity within the studies, we used the random effects model to conduct the meta-analyses.
Statistical heterogeneity was assessed by visual inspection of forest plots, the tau2 statistic, and the I2 statistic. The calculated effect measure was considered significantly heterogeneous when the I2 value was greater than 50%. Clinical heterogeneity was assessed by comparing differences among participants and outcomes, while methodological heterogeneity was considered by comparing study design and risk of bias.
Substantial heterogeneity among studies addressing barriers and interventions for vaccination precluded meta-analysis. To address the second and third objectives, data were collated and summarized using narrative synthesis. The process of narrative synthesis began by extraction of key results, summary statistics, confidence intervals, and p-values (when provided). The studies were categorized according to the vaccine they addressed, followed by their objective (describing vaccination rates, barriers, or interventions). Once categorized, preliminary summary statements were created that allowed for exploration of the relationships in the data. Finally, summary statements from individual studies were collated to describe the overall themes found within the literature.
The qualitative studies addressed the second and third objectives: barriers to vaccination and interventions to overcome vaccine hesitancy. Grounded theory methodology was applied to identify themes. The authors used an inductive process for identifying and coding themes as they emerged from the extracted data. Interrater reliability was performed among two coders to ensure reliability of the results with disagreements settled through consensus. Following discussion of disagreements, an interrater agreement of over 95% was reached.
Results
The initial PubMed search identified 2,359 records published April 2012 through May 2022. Viewing “similar articles” and reference lists of selected articles expanded retrieval, with 63 additional records considered through this approach. The initial broad screening for congruence to inclusion/exclusion criteria performed by a medical librarian was followed by focused reviewer screening, involving 350 studies imported into Covidence. Following removal of duplicates, title, abstract, and full-text screening, 57 studies were deemed eligible for inclusion (Figure 1).18–73
Figure 1.
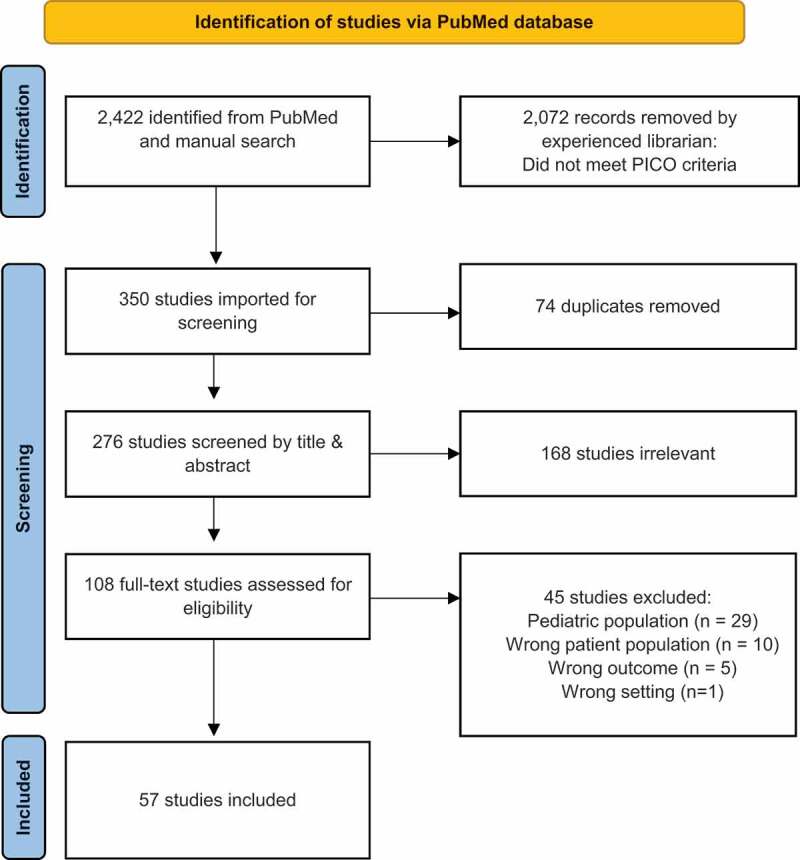
PRISMA diagram17.
Overview of included studies
The included studies addressed human papillomavirus (HPV) (n = 25),21,29–31,35,37,40,42,44,46–48,50,53,55,57,60,61,65–68,71,72,74 influenza (n = 14),20,24–26,28,36,41,46,47,52,58,59,63,64 hepatitis B (n = 11),22,27,34,39,42,43,46,49,51,56,75 COVID-19 (n = 9),18,19,23,32,38,45,54,69,73 pneumococcal (n = 6),26,41,46,47,58,59 tetanus, diphtheria, pertussis/tetanus diphtheria (Tdap/Td) (n = 6),33,41,42,46,47,62 hepatitis A (n = 2),42,46 measles, mumps and rubella (MMR) (n = 2),42,62 and shingles (n = 1)47 vaccines. Several of the included studies covered multiple vaccinations. All studies included data for adults aged 18 y and older and were conducted within the US (Page et al.38 included sites outside of US; however, only US data were extracted). For studies that included minors, data specific to adults was extracted.43,63 The majority of studies included both men and women (n = 43), while 12 focused on women,28,40,44,48,58,51,61,66–68,70,71 and 2 on men.50,59 The study aims included description of vaccination rates (n = 33),18–20,22,24–27,29,30,32–34,36,37,39,41–43,46,47,49,51 ,57–62,64,65,69,72 barriers to vaccination (n = 34),18,19,21–23,28,30–33,35,38–41,44,50–53,55,60,61,63–70,73,75 and interventions to improve vaccination (n = 6).35,36,45,48,56,71 The majority of studies were designed as cross-sectional (n = 41),18–31,33,34,37–41,43,44,46,47,49,51,52,55,57–61,64–67,69,72,75 followed by qualitative (n = 10),32,35,50,53,63,68,70,71,73,76 cohort (n = 3),32,42,62 program evaluation (n = 2),36,45 and quasi-experimental (n = 1).56 Meta-analysis was performed for four vaccines: HPV (n = 7),29,37,46,57,60,61,64 influenza (n = 7),20,25,26,48,58,59,64 hepatitis B (n = 4),27,46,49,51 and pneumococcal (n = 4).26,46,58,59
Critical appraisal of the 47 quantitative studies was conducted using the NIH tools for the assessment of the risk of bias. Studies were appraised after considering study design, sample size, blinding, follow-up, and intrinsic bias. Scores ranged from “poor to good,” with all but two studies classified as “fair” or “good” (supplemental Table S1). Critical appraisal of the 10 qualitative studies was conducted using the Critical Appraisal Skills Programme (CASP) qualitative study checklist (supplemental Table S2). Although a score was not assigned, all 10 studies were appropriately designed to address the study objective, resulting in a clear statement of findings.
Ten qualitative studies were included.33,36,51,54,55,64,69,71,72,74 Eight studies were conducted using focus groups (range: 16–90 participants)36,54,55,64,69,71,72,74 and 2 using semi-structured interviews (13 and 33 participants).33,51 All ten addressed barriers to vaccination, while only six addressed potential interventions.33,51,54,64,69,72 The majority addressed the HPV vaccine (6/10),36,51,54,69,71,72 followed by COVID-19 vaccine (3/10),33,55,74 and influenza vaccine (1/10).64 Definitions and an example quote for each of the themes can be found in Table 1.
Table 1.
Themes addressing barriers and interventions from qualitative studies.
| Theme | Definition | Example quote | N |
|---|---|---|---|
| Barriers | |||
| Lack of knowledge | Knowledge gaps about vaccine preventable disease and/or not knowing that a vaccine exists to prevent the disease | “The greatest barrier to receiving the vaccine was lack of knowledge about this resource.”52 (p5) (Q2, R2, P2) | 7 |
| Misinformation | Incorrect or misleading information resulting in vaccine hesitancy | “Lacking reliable and trustworthy information sources while having access to misinformation was common. Sources of misinformation contributed to the commonly held belief that people would get infected by going to testing sites.”74 (p9) (Q1, R2, P2) | 5 |
| Access | Physical or logistical barriers preventing use of vaccine services, including lack of insurance coverage, lack of primary care physician, or unable to time off work to get vaccinated | “Others were remarkably consistent in their reasons for not getting the vaccine… they experienced inflexible working conditions that did not allow time off to get vaccinated…”64 (p1114) (Q4, R5, P1) | 4 |
| Safety concerns | Concern for harmful, unintended side effects as a result of vaccination | “Personal barriers that were commonly discussed by HNs and CLs included: (1a) Fears related to the vaccine… rumors about the potential side effects of the vaccine were quite common and traveled quickly, saying ‘The bad news goes very fast that the vaccine will cause death or the vaccine will cause this symptom, the vaccine will make you sick, the vaccine will not cure the virus. So those kinds of things I often hear all the time in the community. So, it is challenging for us.’”33 (p1233) (Q10, R6, P2) | 4 |
| Distrust | Lack of confidence in government entities or public health authorities resulting in vaccine hesitancy | “Lack of confidence in government entities (e.g., the political administration, public health), due to the anti-immigrant political context, played a major role in the attitudes and beliefs held by community members.”74 (p9) (Q1, R4, P1) | 4 |
| Cultural bias | Negative attitudes based on cultural norms, practices or beliefs, pressure from family or peers, or fatalism | “Participants were influenced by the people around them, including mothers, physicians, and friends, when considering undergoing a Pap test or HPV vaccination. Others’ negative attitudes toward Pap tests and the HPV vaccine discouraged participants from undergoing the procedures.”71 (p356) (Q5, R4, P1) | 4 |
| Insecurity | Loss of autonomy and stability due the inability to make independent decisions, feeling pressured due to language barriers or immigration status | “Immigration and citizenship status create barriers to COVID-19 testing services and shape ideas around anticipated vaccination. Identification and being identified as undocumented are significant concerns.”55 (p10) (Q8, R4, P3) | 2 |
| Interventions | |||
| Receiving information from a trusted source | Where knowledge gaps or misinformation existed, participants sought a trusted source of information to overcome these barriers. Physicians (4), family members (1), and community leaders (1) were listed trusted sources of information in the studies | “The majority of participants reported that the most influential person on their health decisions is themselves, their family, and their doctor.”69 (p58) (Q6, R3, P2) | 6 |
| Providing culturally tailored education | Participants sought education that provides culturally sensitive, age appropriate, and language congruent content. Social media or trusted news outlets in the community were considered appropriate mediums for transmitting education | “Participants expressed a variety of ideas about the most effective methods to engage the Somali community and increase HPV immunization rates. Many mentioned advertisements in the form of flyers and pamphlets in both English and Somali … Participants suggested using community events and forums in community centers to provide information about HPV and HPV vaccination. Many felt that face-to-face outreach would be the most valuable. These interactions could be between a medical provider and patients; however, participants stressed the value of having someone from within their community, such as a Somali health care provider, involved in the communication effort.”36 (p2047) (Q9, R6, P1) | 5 |
| Facilitating access | Eliminating physical or logistical barriers to vaccination, such as offering vaccine clinics within communities, making appointments widely available, or having language congruent services on site. This may also involve providing incentive for participation | “Both HN [health navigators] and CL [community leaders] respondents offered a variety of potential interventions or suggestions for how to increase vaccine uptake among refugees. These included… (3c) offering a vaccine clinic in the community.”33 (p1235) (Q10, R7, P1) | 3 |
The extracted themes address barriers and interventions to vaccination in the RIM population. The coding system was used by the reviewers through the extraction process and refers to the location of the quote within the original article (article number (Q), subheading within results section (R), and paragraph number below subheading (P)).
Vaccination rates in the RIM population
Meta-analysis was performed to compare vaccination rates for HPV, influenza, hepatitis B, and pneumococcal between foreign-born and US-born participants. The direction of effect was the same for all vaccines, favoring foreign-born participants as an underimmunized population (Figure 2). Pooled data showed that the odds of vaccination were 38% less for HPV vaccination (OR: 0.62, 95% CI: 0.56–0.69, I2 = 0%, Tau2 = 0.00, supplemental Figure S1), 25% less for influenza vaccination (OR 0.75, 95% CI: 0.67–0.84, I2 = 84%, Tau2 = 0.02, supplemental Figure S2), 41% less for hepatitis B vaccination (OR 0.59, 95% CI: 0.39–0.88, p < .0001, I2 = 94%, Tau2 = 0.14, supplemental Figure S3), and 34% less for pneumococcal vaccination (OR 0.66, 95% CI: 0.51–0.85, p < .0001, I2 = 77%, Tau2 = 0.06, supplemental Figure S4). The characteristics for the studies included in the meta-analysis can be found in Table 2.
Figure 2.

Summary of meta-analyses for rates of vaccination for Foreign-born participants compared to US-born.
The figure shows summary estimates for meta-analysis for rates of vaccination between US-born (control) and foreign-born. The summary estimate is odds ratio and reported with 95% confidence interval. The result shows that odds of vaccination was low in a range of 25% to 38% depending on the type of vaccination offered.
Table 2.
Characteristics of studies included within meta-analysis.
| Study | Study Design | Study Time Period | Intervention Group | Comparison Group | N | Effect measure | |
|---|---|---|---|---|---|---|---|
| HPV | Budhwani 2017 | Cross sectional | 2008–2013, except 2010 (data from National Health Interview Survey (NHIS)) | Foreign-born adults across the US | US-born adults | 20,040 | Adjusted odds ratio=0.812, 95% CI: 0.571–1.155 Adjusted for demographics, health variables and economic variables |
| Cofie 2018 | Cross sectional | 2013–2015 (NHIS) | Foreign-born women across the US | US-born women | 15,890 | Adjusted odds ratio=0.58, 95% CI: 0.49–0.70, p<.001 Adjusted for age, education, race/ethnicity, income level, marriage, region, self-rated health status, and OB/GYN visit/Pap test in the past 12months |
|
| Cofie 2022 | Cross sectional | 2013–2017 (NHIS) | Foreign-born Black participants in the US originating from Mexico/Central America/Caribbean Islands/South America, or Africa | US-born Black participants | 5,246 | Adjusted odds ratio=0.73, 95% CI: 0.53–1.01 Adjusted for survey years, sex, age at HPV vaccination eligibility, degree, FPL (federal poverty level), and marital status, insurance stats, self-reported health status, and usual source of care |
|
| De 2017 | Cross sectional | 2013 (NHIS) | Foreign-born adults nationally located throughout the US | US-born adults | 34,557 | Adjusted odds ratio=0.617, 95%: 0.390–0.975, p<.05 Adjusted for race, economic and healthcare access |
|
| Lu 2014 | Cross sectional | 2012 (NHIS) | Foreign- born American adults originating from Mexico/Central America/Caribbean Islands, South America, Europe, or Asia nationally located throughout the US | US-born adults, aged 18-49 | 34,525 | Adjusted prevalence ratio=0.6, 95% CI: 0.4–0.9 Adjusted for age, gender, race/ethnicity, marital status, education, employment status, poverty level, health insurance, number of doctor visits, self-reported health status, region of residence |
|
| McElfish 2021 | Cross sectional | 2014 (NHIS) | Foreign-born Native Hawaiian and Pacific Islanders (NHPI) aged 18–26 in the US | White respondents | 4,602 | Prevalence ratio=0.67, 95% CI: 0.50–0.90, p=.007 Adjusted for race/ethnicity, nativity status, and age |
|
| Perez 2018 | Cross sectional | 2011–2015 (NHIS) | Foreign- born adults nationally located throughout the US | US-born adults | 39,761 | Unadjusted odds ratio=0.57, 95% CI: 0.45–0.73, p<.05 Adjusted odds ratio: Male=0.63, 95% CI: 0.47–0.85 Female=0.57, 95% CI: 0.49–0.66 Adjusted for survey year, age at HPV vaccination eligibility, race/ethnicity, geographic region, and relationship status, educational attainment, employment status, insurance status and usual source of care |
|
| Influenza | Budhwani 2016 | Cross sectional | 2013 (NHIS) | Foreign-born Asian Indians, Blacks, Whites, and other Asians adults nationally located throughout the US | US-born adults | 104,520 | Adjusted odds ratio=0.812, 95% CI: 0.571–1.155, p>.05 Adjusted for interaction between economic and health variables |
| Chuey 2022 | Cross sectional | 2012–2018 (NHIS) | Foreign-born adults from the 2012–2018 NHIS survey nationally located in the US | US-born adults | 29,673 | 2012–2013 US- born=43.8, 95% CI: 42.6–44.9 Foreign- born=37.5, 95% CI: 35.0–40.0, p<.05 2013–2014 US-born=44.0, 95% CI: 42.8–45.3, p<.05 Foreign-born=38.1, 95% CI: 35.7–40.5, p<.05 2014–2015 US-born=45.9, 95% CI: 44.8–47.1 Foreign- born=38.8, 95% CI: 36.5–41.3, p<.05 2015–2016 US-born=44.8, 95% CI: 43.6–46.0 Foreign- born=37.5, 95% CI: 34.8–40.3, p<.05 2016–2017 US-born=45.6, 95% CI: 44.4–46.8 Foreign- born=43.5, 95% CI: 40.6–46.5 2017–2018 US-born=46.9, 95% CI: 45.7–48.1 Foreign- born=42.4, 95% CI: 39.6–45.3, p<.05 Vaccinated: Foreign-born= 39.6% avg (2,023/5,109) US-born = 45.2% avg (11,102/24,564) |
|
| Dallo 2015 (men) | Cross sectional | 2000–2011 (NHIS) | Non-Hispanic white, foreign-born American men from Arab and European nations | Non- Hispanic white US-born men | 91,636 | Adjusted odds ratio: Europe born = 0.47, 95% CI: 0.36–0.62) Arab = 0.38, 95% CI: 0.21–0.67 Adjusted for demographic, socioeconomic, health access, risk factor and acculturation effects |
|
| Dallo 2015 (women) | Cross sectional | 2000–2011 (NHIS) | Non-Hispanic white, foreign-born women originating from Arab and European nations and nationally located throughout the US | Non- Hispanic White US-born women | 117,893 | Adjusted odds ratio: Europe born = 0.48, 95% CI: 0.38–0.60 Arab born = 0.34, 95% CI: 0.21–0.58 Adjusted for demographic, socioeconomic, health access, risk factor and acculturation effects |
|
| Lu 2014 | Cross sectional | 2012 (NHIS) | Foreign- born American adults originating from Mexico/Central America/Caribbean Islands, South America, Europe, or Asia nationally located throughout the US | US-born adults, aged 18-49 | 34,525 | Adjusted Prevalence Ratio=1.0, 95% CI: 0.9–1.0 Adjusted for age, gender, race/ethnicity, marital status, education, employment status, poverty level, health insurance, number of doctor visits, self-reported health status, region of residence |
|
| Tse 2018 | Cross sectional | 2009– 2012 | Foreign-born non-Hispanic blacks, Hispanic, Chinese, Korean, Filipino, or Vietnamese American adults in New York City or Los Angeles and Orange counties in California | US-born adults in New York City or Los Angeles and Orange counties in California | 14,139 | Adjusted odds ratio NYC=1.0, 95% CI: 0.9–1.2, p=.87 LA/Orange County=1.2, 95% CI: 1.1–1.5, p=.01 Adjusted for sociodemographic and health-related factors |
|
| Vashist 2018 | Cross sectional | 2018 (NHIS) | Foreign- born American adults from the 2018 NHIS survey | US-born adults | 24,772 | Adjusted odds ratio=0.91, 95% CI: 0.80–1.04 Adjusted for associations of COVID-19 priority grouping and socioeconomic and health-related factors |
|
| Hepatitis B | Kilmer 2019 | Cross sectional | 2013–2015 (NHIS) | Foreign-born American women of reproductive age (aged 18–44) originating from Mexico, Central America, Caribbean, Indian subcontinent, Southeast Asia, South America, Asia, Africa, or Europe nationally located throughout the US | US-born women (aged 18–44) | 24,216 | Odds ratio: 1.85, 95% CI: 1.67–2.04 (Foreign-born reference) |
| Lee 2013 | Cross sectional | 2010 | Foreign-born, self-identified Asian Pacific Islander college students (aged 18+) in Boston, Massachusetts | US-born college students (aged 18+) | 208 | Odds ratio: 1.4, 95% CI:0.7–2.6 (Foreign-born reference) | |
| Lu 2014 | Cross sectional | 2012 (NHIS) | Foreign- born American adults originating from Mexico/Central America/Caribbean Islands, South America, Europe, or Asia nationally located throughout the US | US-born adults, aged 18-49 | 34, 525 | Adjusted Prevalence Ratio=0.9, 95% CI: 0.8–1.0 Adjusted for age, gender, race/ethnicity, marital status, education, employment status, poverty level, health insurance, number of doctor visits, self-reported health status, region of residence |
|
| Tang 2018 | Cross sectional | 1997–2007 | Foreign-born Asian American adults in NYC | US-born Asian American adults in NYC | 19,816 | Adjusted odds ratio: Birth China=0.22, 95% CI: 0.16–0.31 Birth other non-US=0.33, 95% CI: 0.22–0.48 Adjusted for age, sex, region of birth, language preference, insurances, reported family history of hepatitis B virus |
|
| Pneumococcal | Dallo 2015 (men) | Cross sectional | 2000–2011 (NHIS) | Non-Hispanic white, foreign-born American men from Arab and European nations | Non- Hispanic white US-born men | 91,636 | Adjusted odds ratio: Europe born=0.42, 95% CI: 0.29–0.60 Arab=0.33, 95% CI: 0.16–0.70 Adjusted for demographic, socioeconomic, health access, risk factor and acculturation effects |
| Dallo 2015 (women) | Cross sectional | 2000–2011 (NHIS) | Non-Hispanic white, foreign-born women originating from Arab and European nations and nationally located throughout the US | Non- Hispanic White US-born women | 117,893 | Adjusted odds ratio: Europe born=0.43, 95% CI: 0.28–0.64 Arab born=0.14, 95% CI: 0.06–0.32 Adjusted for demographic, socioeconomic, health access, risk factor and acculturation effects |
|
| Lu 2014 | Cross sectional | 2012 (NHIS) | Foreign-born adults (aged 18+) originating from Mexico/Central America/Caribbean Islands, South America, Europe, or Asia nationally located through the US | US-born adults (aged 18+) | 34, 525 | Adjusted prevalence ratio=0.8, 95% CI: 0.7–1.0 Adjusted for age, gender, race/ethnicity, marital status, education, employment status, poverty level, health insurance, number of doctor visits, self-reported health status, region of residence |
|
| Tse 2018 | Cross sectional | 2009– 2012 | Foreign-born non-Hispanic blacks, Hispanic, Chinese, Korean, Filipino, or Vietnamese American adults in New York City or Los Angeles and Orange counties in California | US-born adults in New York City or Los Angeles and Orange counties in California | 14,139 | Adjusted odds ratio: NYC=1.3, 95% CI: 1.0–1.6, p=.046 LA/Orange County=1.1, 95% CI: 0.7–1.6, p=.81 Adjusted for sociodemographic and health-related factors) |
Heterogeneity within the remaining studies precluded meta-analysis, however a similar trend was observed. Exceptions to this trend were noted for studies evaluating tetanus42,43 and hepatitis A.47
Comparisons between foreign and US-born population were not available for MMR or COVID-19. The characteristics for the studies not included in the meta-analysis can be found in Table 3.
Table 3.
Characteristics of studies excluded from meta-analysis.
| Study | Study Design | Study Time Period | Target population | Comparator | N | Results | |
|---|---|---|---|---|---|---|---|
| HPV | Beltran 2016 | Cross sectional | 2015 | Hmong Americans in Minnesota | None | 192 | HPV initiation: 46.3% HPV completion: 32.7% |
| Lee 2015 | Cross sectional | 2012–2013 | Asian American and Pacific Islander (AAPI) college students in the Midwest US | Non-Latino white students | 2,270 | HPV completion: 38.6% (which was significantly higher than non-Latino white students at 60.7%, p < .001) | |
| Lu 2015* | Cross sectional | 2012 | Foreign-born participants age 19–26 y responding to National Health Interview Survey (NHIS) | US-born | 34,218 | HPV initiation:
|
|
| Mohareb 2021 | Retrospective cohort | 2013–2015 | Adult refugees in Connecticut | None | 111 | HPV initiation within 1 y of resettlement: 15% | |
| Influenza | Lu 2015 | Cross sectional | 2012 | Foreign-born participants responding to National Health Interview Survey (NHIS) | US-born | 34,218 | Influenza vaccination (past 12 months):
|
| Morrison 2012 | Cross sectional | 2008 | Somalian refugees in Minnesota | Non-Somalian clinic patients | 91,557 | Influenza vaccination: 41.45% for Somalian patients (vs. 53.73% for non-Somalian patients, p < .001) | |
| Vlahov 2012 | Cross sectional | 2010 | Foreign-born individuals in an underserved community in New York | US-born individuals in an underserved community in New York | 991 | Interest in influenza vaccination: OR 4.11, 95% CI: 2.19, 7.72 | |
| Hepatitis B | Mitruka 2019 | Cross sectional | 2009–2011 | Adult refugees in California, Massachusetts, Minnesota, and Washington | None | 39,896 | Of susceptible individuals (7,409), 38.3% completed the 3 dose series, 29% received 2 doses, 19.6% received 1 dose, and 13.1% received no doses |
| Mohareb 2021 | Retrospective cohort | 2013–2015 | Adult refugees in Connecticut | None | 111 | HBV initiation: 92% HBV completion of 3 doses 1 y following resettlement: 59% |
|
| Ogunwobi 2019 | Cross sectional | 2016 | African immigrants in New York | None | 70 | HBV initiation: 50.77% | |
| Raines-Milenkov 2021 | Cross sectional | 2014–2020 | Refugee and immigrants in Texas | None | 1,069 | HBV initiation: 26% Uncertain of status: 53% No HBV doses: 21% |
|
| Zhao 2015 | Cross sectional | Not reported | Chinese American immigrants in California | None | 179 | HBV initiation: 26.4% | |
| Pneumococcal | Lu 2015 | Cross sectional | 2012 | Foreign-born participants responding to National Health Interview Survey (NHIS) | US-born population | 34,218 | Pneumococcal vaccination (ever received):
|
| Morrison 2012 | Cross sectional | 2008 | Somalian refugees in Minnesota | Non-Somalian clinic patients | 91,557 | Pneumococcal vaccination: 83.8% for Somalian patients (vs. 86.3% for non-Somalian patients, p = .4546) | |
| TDaP/Td | Chai 2013 | Cross sectional | 2003–2007 | Asylees and refugees in District of Columbia | US-born population | 781 | Need for TDaP or TD: 79.9% of asylees or refugees compared to 48.4% of general US population |
| Lu 2014 | Cross sectional | 2012 | Foreign-born participants responding to National Health Interview Survey (NHIS) | US-born population | 34,525 | Tetanus vaccination containing pertussis (past 7 y): aPR 0.8, 95% CI: 0.7–0.9 | |
| Lu 2015 | Cross sectional | 2012 | Foreign-born participants responding to National Health Interview Survey (NHIS) | US-born population | 34,218 | Tetanus vaccination (past 10 y):
|
|
| Mohareb 2021 | Retrospective cohort | 2013–2015 | Adult refugees in Connecticut | None | 111 | TDaP (1 dose):96% initiated and completed within 1 y of resettlement | |
| Morrison 2012 | Cross sectional | 2008 | Somalian refugees in Minnesota | Non-Somalian clinic patients | 91,557 | Tetanus vaccination Somali patients: 84.6% vs. 83.1% for non-Somali patients (p = .2758) | |
| Sanchez-Gonzalez 2017 | Cross sectional | 2012–2013 | Foreign-born participants responding to National Health Interview Survey (NHIS) | None | 13,154 | Tdap vaccination: 9.1% Td vaccination: 49.8% |
|
| Hepatitis A | Lu 2014 | Cross sectional | 2012 | Foreign-born participants responding to National Health Interview Survey (NHIS) | US-born population | 34,525 | Hepatitis A (among those endorsing travel): aPR = 1.0, 95% CI: 0.8–1.2) |
| Mohareb 2021 | Retrospective cohort | 2013–2015 | Adult refugees in Connecticut | None | 111 | Hepatitis A within 1 y of resettlement: 89% initiated, 83% completed 2 dose series | |
| MMR | Chai 2013 | Cross sectional | 2003–2007 | Asylees and refugees in District of Columbia | US-born population | 781 | Need for MMR:
|
| Mohareb 2021 | Retrospective cohort | 2013–2015 | Adult refugees in Connecticut | None | 111 | MMR within 1 y of resettlement (among non-susceptible): 93% initiated, 71% completed | |
| Shingles | Lu 2015 | Cross sectional | 2012 | Foreign-born participants responding to National Health Interview Survey (NHIS) | US-born population | 34,218 | Shingles vaccination (ever received):
|
| COVID-19 | Abouhala 2021 | Cross sectional | 2020 | Arab Americans | None | 638 | COVID-19 vaccine intent:
aOR vaccine intent by nativity: aOR 1.70, 95% CI 1.05–2.77 (comparator foreign-born Arab Americans to US-born) |
| Kheil 2022 | Cross sectional | 2021 | Arab American immigrants across the US | None | 1,746 | COVID-19 vaccination: 92% by November 2021 | |
| Shaw 2022 | Cohort | 2020–2021 | Refugees in New York | None | 244 | COVID-19 vaccine intent before widespread availability:
COVID-19 vaccine intent before widespread availability:
COVID-19 vaccination after widespread availability: 44.7% |
|
| Sudhinaraset 2022 | Cross sectional | 2020–2021 | Undocumented immigrants in California | None | 326 | COVID-19 vaccine intent: 65% | |
| Zhang 2021 | Cross sectional | 2020–2021 | Refugees across the US | None | 435 | COVID-19 vaccine intent:
Country of origin comparison to Afghan refugees:
|
*Footnotes: Lu 2015 was excluded from the meta-analysis to avoid duplication of data from Lu 2014 (same dataset utilized).
The relative novelty of COVID-19 vaccines resulted in limited publications describing vaccination rates in RIM at the time of our review. For this reason, we included studies conducted prior to broad availability of the vaccine,19,24,70 before and after broad availability,33 or after broad availability.20 Vaccine intent was measured if the study was conducted prior to availability of the COVID-19 vaccine, while vaccination coverage was measured if conducted after. Differences in vaccine intent and acceptance varied by country of origin (Table 3).
Barriers to vaccination in the RIM population
Quantitative studies describing barriers to vaccination
Commonly identified barriers to vaccination prior to the COVID-19 pandemic included knowledge gaps (regarding the vaccine and the disease it prevents),22,31,41,45,56,67,68,75 poor access to medical care (due to lack of health insurance or infrequent visits to a physician),23–32–34–40–42–65–75 and cultural barriers (including language discordance and religiosity)29,31,47,62 (Table 4).
Table 4.
Barriers to vaccination in the RIM population from quantitative studies.
| Study | Study Design | Study Time Period | Population | Location within the US | N | Barriers & Facilitators | |
|---|---|---|---|---|---|---|---|
| HPV | Ashing 2017 | Cross sectional | 2009–2011 | Black/African descended or Hispanic/Latinx immigrants | California | 393 | Black immigrants
Latinx immigrants
|
| Barnack-Tavlaris 2016 | Cross sectional | 2007–2008 | Foreign and US-born women in California | California | 1,672 |
|
|
| Bhattacharya 2021 | Cross sectional | 2017–2018 | Foreign and US-born adults nationally in the US | National | 2,415 |
|
|
| Budhwani 2017 | Cross sectional | 2008– 2013 (except 2010 NHIS) | Asian Indian and Asian subpopulations | National | 234 |
|
|
| Cofie 2018 | Cross sectional | 2013–2015 (NHIS) | Immigrants originating from Mexico, Central America, Caribbean Islands; South America; Europe; Africa; Indian subcontinent; Asia; Southeast Asia | National | 32,917 |
|
|
| Cofie 2022 | Cross sectional | 2013–2017 (NHIS) | Black immigrants originating from Mexico/Central America/Caribbean Islands/South America, or Africa | National | 40,646 |
|
|
| Escobar 2021 | Cross sectional | 2017–2018 | Mexican, Puerto Rican, Cuban, other Hispanic immigrants in the US, US-born Hispanics, and US-born non-Hispanic whites | National | 4,523 |
|
|
| Lee 2015 | Cross sectional | 2012–2013 | Asian American Pacific Islander (AAPI) immigrant college students | Midwest | 2,270 |
|
|
| Lee 2018 | Cross sectional | N/A | Korean American women immigrants | Georgia | 243 |
|
|
| Mehta 2021 | Cross sectional | 2018 | Undocumented and documented Hispanic immigrant women | Rhode Island | 159 |
|
|
| Nguyen 2012 | Cross sectional | 2012 | Mandarin- speaking American immigrants | Northeast | 71 |
|
|
| Influenza | Budhwani 2016 | Cross sectional | 2013 (NHIS) | US-born and foreign- born Asian Indians, Blacks, Whites, and other Asians adults | National | 104,520 |
|
| Jih 2015 | Cross sectional | 2007, 2009 | Latino and Asian immigrants with low English proficiency (LEP) | California | 4,821 |
|
|
| Moran 2017 | Cross sectional | 2012–2013 | Hispanic female immigrants from Central and South America | California | 1,565 |
|
|
| Morrison 2012 | Cross sectional | 2008 | Somalian refugees | Minnesota | 91,557 |
|
|
| Ogunwobi 2019 | Cross sectional | 2016 | African immigrants | New York | 70 |
|
|
| Strong 2012 | Cross sectional | 2009–2010 | Chinese, Korean, and Vietnamese immigrants | Maryland | 877 |
|
|
| Zhao 2015 | Cross sectional | NR | Chinese immigrants | California | 179 |
|
|
| Pneumococcal | Morrison 2012 | Cross sectional | 2008 | Somalian refugees | Minnesota | 91,557 |
|
| Tetanus | Morrison 2012 | Cross sectional | 2008 | Somalian refugees | Minnesota | 91,557 |
|
| Lu 2014 | Cross sectional | 2012 | Foreign-born individuals residing in the US | National | 34,525 |
|
|
| Sanchez-Gonzalez 2017 | Cross sectional | 2012–2013 | Foreign-born individuals residing in the US | National | 13,154 |
|
|
| COVID-19 | Abouhala 2021 | Cross sectional | 2020 | Arab Immigrants | National | 638 |
|
| Kheil 2022 | Cross sectional | 2021 | Arab Immigrants | National | 1,603 |
|
|
| Page 2022 | Cross sectional | 2021 | Migrants | International (extracted data from Maryland) | 142 |
|
|
| Shaw 2022 | Cohort | 2020–2021 | Refugees | New York | 244 |
|
|
| Sudhinaraset 2022 | Cross sectional | 2020–2021 | Undocumented immigrants | California | 326 |
|
|
| Zhang 2021 | Cross sectional | 2020–2021 | Refugees | National | 435 |
|
Following the introduction of the COVID-19 vaccine, unique barriers emerged while some existing barriers intensified (Table 4). Safety concerns and distrust in the healthcare system, vaccines, and government were recurring themes for those with vaccine hesitancy amid the emergence of COVID-19 vaccines.19,20,24,39,70
Qualitative studies describing barriers to vaccination
Similar themes emerged from the qualitative literature. Seven themes regarding barriers to vaccination were identified: lack of knowledge,36,51,54,64,69,71,72 misinformation,36,54,64,77 access,33,51,65,71 safety concerns,33,36,51,64 distrust,36,64,74 cultural bias,36,54,71 and insecurity.74 Knowledge gaps existed regarding the disease process itself and a vaccine available to prevent it. This lack of awareness was a commonly identified theme among undervaccinated RIM communities. Even when awareness existed, misinformation was often identified. Many participants within the RIM community had received either incorrect or misleading information that resulted in vaccine hesitancy. This was particularly true for studies discussing COVID-19 vaccines. Access to vaccination was blocked by both physical (inaccessible location or lack of transportation) or logistical (incongruent language, lack of insurance, lack of provider, unable to take off work) barriers. Concern for safety was the result of either a personal history of vaccine side effects or safety concerns conveyed by trusted resources in the RIM community. Distrust of government or public health authorities was identified as a common barrier, which was amplified during the COVID-19 pandemic. Themes of cultural bias emerged as negative attitudes based on cultural norms, practices, or beliefs. Within certain RIM communities, the concept of “fatalism” was used to justify vaccine refusal. Finally, insecurity was a unique concern within the RIM population. Fear of deportation prevented access to healthcare services where vaccination could occur. While this barrier is unique to the RIM community, it was commonly identified across communities within RIM.
Interventions to address vaccine hesitancy
Quantitative study describing an intervention to address HPV vaccine hesitancy (n = 1)
One quantitative study described an intervention designed to improve HPV vaccination rates. Lee et al.72 performed a quasi-experimental study involving 30 Korean American immigrants. They tested a mobile health intervention designed to identify barriers, develop motivators, and provide a trigger to initiate HPV vaccination among participants. Pre- and post-intervention surveys identified significant increases in HPV and HPV vaccination knowledge, and positive changes to personal barriers, culturally based attitudes, and self-efficacy toward cervical cancer prevention. Additionally, vaccine intent significantly increased (mean difference = 0.47, 95% CI: 0.21–0.72; p < .001), with 30% of participants receiving the HPV vaccine within 3-months of the intervention (95% CI: 9.9–42.3%).
Quantitative study describing an intervention to address influenza vaccine hesitancy (n = 1)
Ponce-Gonzalez et al.37 conducted a study of 155 participants from Latinx families living in underserved communities. Participants were engaged in a community health worker vaccination promotion campaign, which consisted of two-hour workshops on the importance of getting the flu vaccine. The proportion of participants who identified vaccination as effective for influenza increased from 29% pre-workshop to 47.7% post-workshop.
Quantitative study describing interventions for hepatitis B vaccination coverage (n = 1)
One quantitative study described an intervention to increase HBV vaccination rates.
Djoufack et al.56 conducted a quasi-experimental study to determine if community outreach could improve hepatitis B knowledge among immigrants within the Greater Boston area. The study recruited 101 participants to assess knowledge before and after the intervention. The intervention consisted of six 45-min sessions hosted at trusted locations within the community. Live interpreters translated the sessions that focused on hepatitis B education and led to an insignificant increase in HBV knowledge (pre: 64% vs. Post: 75%, p = .20).
Quantitative study describing an intervention to address COVID-19 vaccine hesitancy (n = 1)
Malone et al.45 described the efforts of a community-based primary care clinic in Clarkston, Georgia, in providing COVID-19 vaccination to 3,127 immigrants and refugees. They found that three main factors led to sustainability of their vaccination efforts: establishing relationships of trust in the community, using multiple avenues of access, and providing consistent vaccination location and time.
Qualitative studies describing effective intervention strategies for vaccination (n = 7)
Three themes regarding interventions emerged from the seven applicable studies: receiving information from a trusted source,32,50,53,63,68 providing culturally tailored education,32,50,53,63,68 and facilitating access.32,68 A strong physician recommendation was found to be a trusted resource in most studies, while others sought family support or support from community leaders. Delivering culturally sensitive and language congruent content via social media or community platforms was thought to be an effective strategy. Finally, facilitating access to educational materials, or vaccination itself through community vaccination sites, was a desired intervention strategy.
Discussion
Vaccine hesitancy has steadily increased in the US and worldwide over the past decade. In 2019, the World Health Organization declared vaccine hesitancy as one of the top 10 threats to global health, emphasizing the urgency of the matter.75 To address this threat, we reviewed literature published in the past decade with the inclusion of COVID-19 vaccine hesitancy, as it has not been previously systematically captured. The broad scope and timely inclusion of COVID-19 literature distinguish this review from prior work, and in doing so, highlight the gaps in existing knowledge.
Our review identifies RIMs as an underimmunized community with lower vaccination rates compared to the US-born population, thus increasing their vulnerability to VPDs. Unfortunately, the lack of comparable data relating to COVID-19 vaccination rates precluded meta-analysis. Given its novelty, literature comparing COVID-19 vaccination rates of the RIM population to the general US population is limited. We found variability in COVID-19 vaccine intent based on nativity, however intent did not necessarily translate to vaccine uptake.23,32,69 Our results highlight the need for further research in this area, especially amid escalating vaccine hesitancy.
Common barriers to vaccination included knowledge gaps, poor access to care, cultural bias, and distrust of the medical system. Following the introduction of COVID-19 vaccines, safety concerns emerged as an increasingly cited barrier. This finding is not surprising and in congruence with what has been seen in the general US population. Rampant misinformation, coupled with distrust in the scientific community, is associated with poor COVID-19 vaccine acceptance.77,78 To address these barriers, we searched the literature for effective interventions. Although limited, a few non-randomized studies described the importance of establishing trusted relationships within the community, facilitating access, and providing culturally sensitive education to increase vaccine uptake.32,36,63
Strengths and limitations
This systematic review includes 57 studies, allowing for a robust and comprehensive response to the stated objectives. The nature of the questions raised resulted in the majority of included studies being cross-sectional or qualitative in design. Thus, the results and interpretation of our results carry risk for bias inherent to these designs. Quality assessment of the included studies revealed that the vast majority were methodologically sound with low risk of bias.
Despite a fair amount of clinical heterogeneity in the studied populations, there was a remarkable statistical homogeneity for HPV vaccination. This can be partly explained by the use of the National Health Interview Survey (NHIS) database with overlapping time periods among included studies. In contrast, there was significant statistical heterogeneity for the meta-analyses for influenza, pneumococcal, and hepatitis B vaccination. Despite the noted heterogeneity, the direction of effect was the same within all meta-analyses, demonstrating that the RIM population has decreased odds of vaccination compared to the US-born population.
To minimize bias in conducting the review, we prespecified inclusion/exclusion criteria. The process of screening, quality assessment, and data extraction was conducted in duplication. Despite a comprehensive search strategy, the use of a single electronic database (PubMed) provided a possible limitation to the studies captured. Additionally, by limiting the included studies to the past 10 y, there may have been relevant studies published prior to 2012 that were excluded. With the development and distribution of new vaccines, however, vaccine hesitancy is a fluid and evolving field that requires a timely response. As previously mentioned, the decision to limit the study period to the past decade ensured inclusion of a robust dataset during a period of growing vaccine hesitancy while maintaining relevancy to today’s RIM population.
Implications for practice
Our findings have important implications for practice. The combination of limited prior experience with vaccines, low health literacy, and lack of access to local healthcare infrastructure results in a lower priority for non-required vaccinations among RIM populations. These structural and modifiable barriers remain an important reason for undervaccination.18,38,55 Enhancing access to timely and routine care, provided in culturally sensitive settings over time builds trust and comfort with the recommendations offered.32,35,73 Bringing vaccines closer to populations to bridge trusted voices, community health workers, and culturally aligned community sites was a way to accelerate uptake for COVID-19 vaccination among vulnerable populations.32,45 Lack of insurance status for many RIM populations will continue to pose a barrier to obtaining regular care, proper documentation, and consistent recommendations for VPD.31,74 Provision of affordable quality health services will require allocation of resources to meet the highly diverse needs of RIM communities.
Limited experience with vaccines and low health literacy are common barriers to engaging RIM populations in the relative importance of vaccination. For example, very few countries have systemic HPV vaccination and cervical cancer screening programs available; therefore, RIM populations do not come with a baseline knowledge and awareness of this VPD. This low baseline knowledge is correlated with negative attitudes and perceptions of the vaccine.79 Other RIM populations have had strong sources of misinformation guiding their vaccine refusal. Rampant misinformation linking MMR vaccine to a diagnosis of autism drove down MMR vaccination rates within the Somali population in Minnesota and led to subsequent measles outbreaks.1,2,80 Culturally aligned, trusted providers and community health interventions should be sought to overcome these barriers by establishing respectful relationships to engage health educational programs within the community.
Implications for policy
Systematic health programs designed for timely health screening and vaccination have been shown to improve vaccination rates among certain RIM.81 Required health screenings and vaccination within 30–90 days of arrival guarantee access and interface with a health system designed to meet the needs of a culturally diverse population. Ensuring that these programs sustain federal funding will secure access for diverse RIM populations who arrive with limited health literacy. As RIM populations assimilate, proven strategies such as mandating school and employer vaccinations will improve immunization rates.82 Finally, those with the opportunity to apply for a visa or adjust status for permanent residency will face US Citizenship and Immigration Services’ policies that require administration of certain vaccines.83 Broadening the list of required vaccines to meet the Advisory Committee on Immunization Practices (ACIP) guidelines will improve immunization rates through this process.83
Implications for future research
Despite a fair degree of overlap, there were important differences in vaccination barriers as a result of the cultural diversity within the RIM population. Caution should be taken when attempting to generalize these results to subsets within this population, particularly when addressing COVID-19 vaccination. Additional research is necessary to clarify these differences and tailor culturally sensitive, effective interventions amid the current pandemic.19,24,70
Although there is a clear risk for VPD and many barriers have been identified, strategies to overcome vaccine hesitancy within the RIM population are lacking. Technology is increasingly used to develop tailored vaccine education material to circumvent educational and cultural barriers.49,72 The current design and scope of the studies, however, limit their widespread applicability. Randomized controlled trials involving diverse populations are necessary to truly determine their efficacy and generalizability.
Conclusions
The RIM community has lower vaccination coverage when compared to those born in the US. Barriers, such as language, poor access to medical care, and distrust for the medical system, are modifiable with increased commitment of resources. Effective interventions are only partially understood, necessitating further research to ensure improved coverage and reduced risk of VPD outbreaks. Promoting policy that will secure federal funding for health services, while adopting ACIP guidelines for recommended immunizations, will improve vaccination rates for RIM. Our review highlights the RIM population as a vulnerable group in need of unique interventions to overcome barriers to vaccination.
Supplementary Material
Acknowledgments
We would like to acknowledge Dr Telisa Stewart who graciously provided guidance as we developed our methodology and synthesis of qualitative evidence.
Funding Statement
Supported by Ministry of Health of the Czech Republic, grant nr. NU20-09-00454.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2022.2131168.
References
- 1.Link-Gelles R, Lutterloh E, Schnabel Ruppert P, Backenson PB, St George K, Rosenberg ES, Anderson BJ, Fuschino M, Popowich M, Punjabi C, et al. Public health response to a case of paralytic poliomyelitis in an unvaccinated person and detection of poliovirus in wastewater — New York, June–August 2022. MMWR Morb Mortal Wkly Rep. 2022;71(33):1–19. doi: 10.15585/mmwr.mm7133e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tenforde MW, Self WH, Adams K, Gaglani M, Ginde AA, McNeal T, Ghamande S, Douin DJ, Talbot HK, Casey JD, et al. Association between mRNA vaccination and COVID-19 hospitalization and disease severity. JAMA. 2021;326(20):2043–54. doi: 10.1001/jama.2021.19499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bahta L, Ashkir A.. Addressing MMR vaccine resistance in Minnesota’s Somali community. Minn Med. 2015;98(10):33-36. [PubMed] [Google Scholar]
- 4.Christianson B, Sharif-Mohamed F, Heath J, Roddy M, Bahta L, Omar H, Rockwood T, Kenyon C. Parental attitudes and decisions regarding MMR vaccination during an outbreak of measles among an undervaccinated Somali community in Minnesota. Vaccine. 2020;38(45):6979–84. doi: 10.1016/j.vaccine.2020.09.022. [DOI] [PubMed] [Google Scholar]
- 5.Esterline C, Batalova J. Frequently requested statistics on immigrants and immigration in the United States. 2022. Mar 17 [accessed 2022 Jun 26]. https://www.migrationpolicy.org/article/frequently-requested-statistics-immigrants-and-immigration-united-states.
- 6.Centers for Disease Control and Prevention NC for E and ZID (NCEZID), D of GM and Q (DGMQ) . Refugee health profiles. 2021. Jan 14 [accessed 2022 Jun 26]. https://www.cdc.gov/immigrantrefugeehealth/profiles/index.html.
- 7.Rojas-Venegas M, Cano-Ibáñez N, Khan KS. Vaccination coverage among migrants: a systematic review and meta-analysis. Semergen. 2022;48(2):96–105. doi: 10.1016/j.semerg.2021.10.008. [DOI] [PubMed] [Google Scholar]
- 8.Wilson L, Rubens-Augustson T, Murphy M, Jardine C, Crowcroft N, Hui C, Wilson K. Barriers to immunization among newcomers: a systematic review. Vaccine. 2018;36(8):1055–62. doi: 10.1016/j.vaccine.2018.01.025. [DOI] [PubMed] [Google Scholar]
- 9.Tankwanchi AS, Bowman B, Garrison M, Larson H, Wiysonge CS. Vaccine hesitancy in migrant communities: a rapid review of latest evidence. Curr Opin Immunol. 2021;71:62–68. doi: 10.1016/j.coi.2021.05.009. [DOI] [PubMed] [Google Scholar]
- 10.Centers for Disease Control and Prevention . COVID-19 in newly resettled refugee populations. 2020. Dec 21 [accessed 2022 Jul 2]. https://stacks.cdc.gov/view/cdc/99170.
- 11.Abba-Aji M, Stuckler D, Galea S, McKee M. Ethnic/Racial minorities’ and migrants’ access to COVID-19 vaccines: a systematic review of barriers and facilitators. J Migr Health. 2022;5:100086. doi: 10.1016/j.jmh.2022.100086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Veritas Health Information . Covidence systematic review software. Melbourne (Australia); 2022. Jun 28. [Google Scholar]
- 13.Rani U, Darabaner E, Seserman M, Bednarczyk RA, Shaw J. Public education interventions and uptake of human papillomavirus vaccine: a systematic review. J Public Health Manag Pract. 2020;28(1):E307–15. doi: 10.1097/PHH.0000000000001253. [DOI] [PubMed] [Google Scholar]
- 14.NIH National Heart L and BI . Study quality assessment tools. 2021. Jul [accessed 2022 Jul 2]. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
- 15.Critical Appraisal Skills Programme . CASP systematic review checklist. 2018. [accessed 2022 Jun 14]. https://casp-uk.net/wp-content/uploads/2018/01/CASP-Systematic-Review-Checklist_2018.pdf.
- 16.Review Manager (RevMan) . RevMan version 5.4. 2020. [accessed 2022 Jun 14]. https://documentation.cochrane.org/revman-kb/get-started.
- 17.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. The BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sudhinaraset M, Nwankwo E, Choi HY. Immigration enforcement exposures and COVID-19 vaccine intentions among undocumented immigrants in California. Prev Med Rep. 2022;27:101808. doi: 10.1016/j.pmedr.2022.101808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kheil MH, Jain D, Jomaa J, Askar B, Alcodray Y, Wahbi S, Brikho S, Kadouh A, Harajli D, Jawad ZN, et al. COVID-19 vaccine hesitancy among Arab Americans. Vaccines. 2022;10(4):610. doi: 10.3390/vaccines10040610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chuey MR, Hung MC, Srivastav A, Lu P-J, Nguyen KH, Williams WW, Lainz AR. Influenza vaccination coverage among adults by nativity, race/ethnicity, citizenship, and language of the interview - United States, 2012-2013 through 2017-2018 influenza seasons. Am J Infect Control. 2022;50(5):497–502. doi: 10.1016/j.ajic.2021.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bhattacharya M, Xiong S, McRee AL. Nativity differences in awareness and knowledge about HPV infection and vaccination among US adults: findings from a national population-based sample. J Immigr Minor Health. 2022;24(3):794–98. doi: 10.1007/s10903-021-01268-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zhao X, Edwards QT, Patel N, Hicks RW. Hepatitis B knowledge and preventive practices of Chinese American immigrants in Southern California. J Am Assoc Nurse Pract. 2015;27(4):205–12. doi: 10.1002/2327-6924.12173. [DOI] [PubMed] [Google Scholar]
- 23.Zhang M, Gurung A, Anglewicz P, Subedi P, Payton C, Ali A, Ibrahim A, Haider M, Hamidi N, Atem J, et al. Acceptance of COVID-19 vaccine among refugees in the United States. Public Health Rep. 2021;136(6):774–81. doi: 10.1177/00333549211045838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Vlahov D, Bond KT, Jones KC, Ompad DC. Factors associated with differential uptake of seasonal influenza immunizations among underserved communities during the 2009-2010 influenza season. J Community Health. 2012;37(2). doi: 10.1007/s10900-011-9443-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vashist K, Choi D, Patel SA. Identification of groups at high risk for under-coverage of seasonal influenza vaccination: a national study to inform vaccination priorities during the COVID-19 pandemic. Ann Epidemiol. 2022;68:16–23. doi: 10.1016/j.annepidem.2021.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tse SC, Wyatt LC, Trinh-Shevrin C, Kwon SC. Racial/Ethnic differences in influenza and pneumococcal vaccination rates among older adults in New York City and Los Angeles and orange counties. Prev Chronic Dis. 2018;15(12). doi: 10.5888/pcd15.180101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Tang AS, Lyu J, Wang S, He Q, Pong P, Harris AM. Disparities in hepatitis B virus infection and immunity among New York City Asian American patients, 1997 to 2017. Am J Public Health. 2018;108(S4):S327–35. doi: 10.2105/AJPH.2018.304504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Moran MB, Chatterjee JS, Frank LB, Murphy ST, Zhao N, Chen N, Ball-Rokeach S. Individual, cultural and structural predictors of vaccine safety confidence and influenza vaccination among Hispanic female subgroups. J Immigr Minor Health. 2017;19(4):790–800. doi: 10.1007/s10903-016-0428-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.McElfish PA, Narcisse MR, Felix HC, Cascante DC, Nagarsheth N, Teeter B, Faramawi MF. Race, nativity, and sex disparities in human papillomavirus vaccination among young adults in the USA. J Racial Ethn Health Disparities. 2021;8(5):1260–66. doi: 10.1007/s40615-020-00886-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lee HY, Kwon M, Vang S, DeWolfe J, Kim NK, Lee DK, Yeung M. Disparities in human papillomavirus vaccine literacy and vaccine completion among Asian American Pacific Islander undergraduates: implications for cancer health equity. J Am Coll Health. 2015;63(5):316–23. doi: 10.1080/07448481.2015.1031237. [DOI] [PubMed] [Google Scholar]
- 31.Lee HY, Choi YJ, Yoon YJ, Oh J. HPV literacy: the role of English proficiency in Korean American immigrant women. Clin J Oncol Nurs. 2018;22(3):E64–70. doi: 10.1188/18.CJON.E64-E70. [DOI] [PubMed] [Google Scholar]
- 32.Shaw J, Anderson KB, Fabi RE, Thompson CA, Harris M, Aljabbarin N, Bolourchi D, Mozo N, Lichtenstein D, Lupone CD, et al. COVID-19 vaccination intention and behavior in a large, diverse, US refugee population. Vaccine. 2022;40(9):1231–37. doi: 10.1016/j.vaccine.2022.01.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sánchez-González L, Rodriguez-Lainz A, O’Halloran A, Rowhani-Rahbar A, Liang JL, Lu P-J, Houck PM, Verguet S, Williams WW. Factors related to Pertussis and Tetanus vaccination status among foreign-born adults living in the United States. J Community Health. 2017;42(3):573–82. doi: 10.1007/s10900-016-0290-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Raines-Milenkov A, Felini M, Baker E, Acharya R, Longanga Diese E, Akpan I, Hussain A, Wagner T. Hepatitis B virus awareness, infection, and screening multiethnic community intervention for foreign-born populations. J Community Health. 2021;46(5):967–74. doi: 10.1007/s10900-021-00982-5. [DOI] [PubMed] [Google Scholar]
- 35.Pratt R, Njau SW, Ndagire C, Chaisson N, Toor S, Ahmed N, Mohamed S, Dirks J. “We are Muslims and these diseases don’t happen to us”: a qualitative study of the views of young Somali men and women concerning HPV immunization. Vaccine. 2019;37(15):2043–50. doi: 10.1016/j.vaccine.2019.03.006. [DOI] [PubMed] [Google Scholar]
- 36.Ponce-Gonzalez IM, Perez K, Cheadle AD, Jade M, Iverson B, Parchman ML. A multicomponent health education campaign led by community health workers to increase Influenza vaccination among migrants and refugees. J Prim Care Community Health. 2021;12:215013272110556. doi: 10.1177/21501327211055627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pérez AE, Agénor M, Gamarel KE, Operario D. Nativity disparities in Human Papillomavirus vaccination among US adults. Am J Prev Med. 2018;54(2):248–58. doi: 10.1016/j.amepre.2017.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Page KR, Genovese E, Franchi M, Cella S, Fiorini G, Tlili R, Salazar S, Duvoisin A, Cailhol J, Jackson Y. COVID-19 vaccine hesitancy among undocumented migrants during the early phase of the vaccination campaign: a multicentric cross-sectional study. BMJ Open. 2022;12(3):e056591. doi: 10.1136/bmjopen-2021-056591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ogunwobi OO, Dibba O, Zhu L, Ilboudo A, Tan Y, Fraser MA, Ma GX. Hepatitis B virus screening and vaccination in first-generation African immigrants: a pilot study. J Community Health. 2019;44(6):1037–43. doi: 10.1007/s10900-019-00668-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Nguyen GT, Chen B, Chan M. Pap testing, awareness, and acceptability of a human papillomavirus (HPV) vaccine among Chinese American women. J Immigr Minor Health. 2012;14(5):803–08. doi: 10.1007/s10903-012-9607-5. [DOI] [PubMed] [Google Scholar]
- 41.Morrison TB, Wieland ML, Cha SS, Rahman AS, Chaudhry R. Disparities in preventive health services among Somali immigrants and refugees. J Immigr Minor Health. 2012;14(6):968–74. doi: 10.1007/s10903-012-9632-4. [DOI] [PubMed] [Google Scholar]
- 42.Mohareb AM, Brown B, Ikuta KS, Hyle EP, Annamalai A. Vaccine completion and infectious diseases screening in a cohort of adult refugees following resettlement in the US: 2013–2015. BMC Infect Dis. 2021;21(1). doi: 10.1186/s12879-021-06273-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Mitruka K, Pezzi C, Baack B, Burke H, Cochran J, Matheson J, Urban K, Ramos M, Byrd K. Evaluation of hepatitis B virus screening, vaccination, and linkage to care among newly arrived refugees in four states, 2009–2011. J Immigr Minor Health. 2019;21(1):39–46. doi: 10.1007/s10903-018-0705-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mehta N, Raker C, Robison K. Cervical cancer prevention: screening among undocumented Hispanic women compared with documented Hispanic women. J Low Genit Tract Dis. 2021;25(2):86–91. doi: 10.1097/LGT.0000000000000587. [DOI] [PubMed] [Google Scholar]
- 45.Malone B, Kim E, Jennings R, Pacheco RA, Kieu A. COVID-19 vaccine distribution in a community with large numbers of immigrants and refugees. Am J Public Health. 2022;112(3):393–96. doi: 10.2105/AJPH.2021.306608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lu PJ, Rodriguez-Lainz A, O’Halloran A, Greby S, Williams WW. Adult vaccination disparities among foreign-born populations in the US, 2012. Am J Prev Med. 2014;47(6):722–33. doi: 10.1016/j.amepre.2014.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lu PJ, O’Halloran A, Williams WW, Lindley MC, Farrall S, Bridges CB. Racial and ethnic disparities in vaccination coverage among adult populations in the U.S. Am J Prev Med. 2015;49(6):S412–25. doi: 10.1016/j.amepre.2015.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lee HY, Koopmeiners JS, McHugh J, Raveis VH, Ahluwalia JS. mHealth pilot study: text messaging intervention to promote HPV vaccination. Am J Health Behav. 2016;40(1):67–76. doi: 10.5993/AJHB.40.1.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lee H, Kiang P, Watanabe P, Halon P, Shi L, Church DR. Hepatitis B virus infection and immunizations among Asian American college students: infection, exposure, and immunity rates. J Am Coll Health. 2013;61(2):67–74. doi: 10.1080/07448481.2012.753891. [DOI] [PubMed] [Google Scholar]
- 50.Koskan AM, Fernandez-Pineda M. Anal cancer prevention perspectives among foreign-born Latino HIV-infected gay and bisexual men. Cancer Control. 2018;25(1):107327481878036. doi: 10.1177/1073274818780368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kilmer GA, Barker LK, Ly KN, Jiles RB. Hepatitis B vaccination and screening among foreign-born women of reproductive age in the United States: 2013–2015. Clin Infect Dis. 2019;68(2):256–65. doi: 10.1093/cid/ciy479. [DOI] [PubMed] [Google Scholar]
- 52.Jih J, Vittinghoff E, Fernandez A. Patient-physician language concordance and use of preventive care services among limited English proficient Latinos and Asians. Public Health Rep. 2015;130(2):134–42. doi: 10.1177/003335491513000206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ghebrendrias S, Pfeil S, Crouthamel B, Chalmiers M, Kully G, Mody S. An examination of misconceptions and their impact on cervical cancer prevention practices among Sub-Saharan African and Middle Eastern refugees. Health Equity. 2021;5(1):382–89. doi: 10.1089/heq.2020.0125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gehlbach D, Vázquez E, Ortiz G, Li, E, Beltrán Sánchez, C, Rodriguez, S, Pozar, M, Cheney, M . COVID-19 testing and vaccine hesitancy in Latinx farm-working communities in the Eastern Coachella Valley. Res Sq. 2021. doi: 10.21203/rs.3.rs-587686/v1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Escobar B, Amboree TL, Sonawane K, Deshmukh AA, McGee LU, Rodriguez AM, Jibaja-Weiss ML, Montealegre JR. Human papillomavirus awareness among foreign- and US-born Hispanics, United States, 2017–2018. Prev Med Rep. 2021;22:101379. doi: 10.1016/j.pmedr.2021.101379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Djoufack R, Cheon SSY, Mohamed A, Faye F, Diouf K, Colvin R, Morrill J, Duffy-Keane A-M, Perumalswami P, Jourdain G, et al. Hepatitis B virus outreach to immigrant population in Greater Boston Area: key to improving hepatitis B knowledge. World J Gastroenterol. 2017;23(42):7626–34. doi: 10.3748/wjg.v23.i42.7626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.De P, Budhwani H. Human papillomavirus (HPV) vaccine initiation in minority Americans. Public Health. 2017;144:86–91. doi: 10.1016/j.puhe.2016.11.005. [DOI] [PubMed] [Google Scholar]
- 58.Dallo FJ, Kindratt TB. Disparities in vaccinations and cancer screening among US- and foreign-born Arab and European American Non-Hispanic white women. Women’s Health Issues. 2015;25(1):56–62. doi: 10.1016/j.whi.2014.10.002. [DOI] [PubMed] [Google Scholar]
- 59.Dallo FJ, Kindratt TB. Disparities in preventive health behaviors among Non-Hispanic white men: heterogeneity among foreign-born Arab and European Americans. Am J Mens Health. 2015;9(2):124–31. doi: 10.1177/1557988314532285. [DOI] [PubMed] [Google Scholar]
- 60.Cofie LE, Tailor HD, Lee MH, Xu L. HPV vaccination uptake among foreign-born blacks in the US: insights from the national health interview survey 2013–2017. Cancer Causes Control. 2022;33(4):583–91. doi: 10.1007/s10552-021-01550-x. [DOI] [PubMed] [Google Scholar]
- 61.Cofie LE, Hirth JM, Guo F, Berenson AB, Markides K, Wong R. HPV vaccination among foreign-born women: examining the national health interview survey 2013–2015. Am J Prev Med. 2018;54(1):20–27. doi: 10.1016/j.amepre.2017.08.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Chai SJ, Davies-Cole J, Cookson ST. Infectious disease burden and vaccination needs among asylees versus refugees, District of Columbia. Clin Infect Dis. 2013;56(5):652–58. doi: 10.1093/cid/cis927. [DOI] [PubMed] [Google Scholar]
- 63.Cassady D, Castaneda X, Ruelas MR, Vostrejs MM, Andrews T, Osorio L. Pandemics and vaccines: perceptions, reactions, and lessons learned from hard-to-reach Latinos and the H1N1 campaign. J Health Care Poor Underserved. 2012;23(3):1106–22. doi: 10.1353/hpu.2012.0086. [DOI] [PubMed] [Google Scholar]
- 64.Budhwani H, De P. Disparities in influenza vaccination across the United States: variability by minority group, Asian sub-populations, socio-economic status, and health insurance coverage. Public Health. 2016;138:146–53. doi: 10.1016/j.puhe.2016.04.003. [DOI] [PubMed] [Google Scholar]
- 65.Budhwani H, De P. Human papillomavirus vaccine initiation in Asian Indians and Asian subpopulations: a case for examining disaggregated data in public health research. Public Health. 2017;153:111–17. doi: 10.1016/j.puhe.2017.07.036. [DOI] [PubMed] [Google Scholar]
- 66.Barnack-Tavlaris JL, Garcini LM, Macera CA, Brodine S, Klonoff EA. Human Papillomavirus vaccination awareness and acceptability among US-Born and US foreign-born women living in California. Health Care Women Int. 2016;37(4):444–62. doi: 10.1080/07399332.2014.954702. [DOI] [PubMed] [Google Scholar]
- 67.Ashing KT, Carrington A, Ragin C, Roach V. Examining HPV- and HPV vaccine-related cognitions and acceptability among US-born and immigrant Hispanics and US-born and immigrant non-Hispanic Blacks: a preliminary catchment area study. Cancer Causes Control. 2017;28(11). doi: 10.1007/s10552-017-0973-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Allen EM, Lee HY, Pratt R, Vang H, Desai JR, Dube A, Lightfoot E. Facilitators and barriers of cervical cancer screening and Human Papilloma Virus vaccination among Somali refugee women in the United States: a qualitative analysis. J Transcult Nurs. 2019;30(1):55–63. doi: 10.1177/1043659618796909. [DOI] [PubMed] [Google Scholar]
- 69.Abouhala S, Hamidaddin A, Taye M, Glass DJ, Zanial N, Hammood F, Allouch F, Abuelezam NN. A national survey assessing COVID-19 vaccine hesitancy Among Arab Americans. J Racial Ethn Health Disparities. 2021. doi: 10.1007/s40615-021-01158-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Lee HY, Lee MH. Barriers to cervical cancer screening and prevention in young Korean immigrant women: implications for intervention development. J Transcult Nurs. 2017;28(4). doi: 10.1177/1043659616649670. [DOI] [PubMed] [Google Scholar]
- 71.Lee HY, Lee MH, Sharratt M, Lee S, Blaes A. Development of a mobile health intervention to promote Papanicolaou tests and human papillomavirus vaccination in an underserved immigrant population: a culturally targeted and individually tailored text messaging approach. JMIR Mhealth Uhealth. 2019;7(6):e13256. doi: 10.2196/13256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Beltran R, Simms T, Lee HY, Kwon M. HPV literacy and associated factors among Hmong American immigrants: implications for reducing cervical cancer disparity. J Community Health. 2016;41(3):603–11. doi: 10.1007/s10900-015-0135-9. [DOI] [PubMed] [Google Scholar]
- 73.Gehlbach D, Vázquez E, Ortiz G, Li E, Sánchez CB, Rodríguez S, Pozar M, Cheney AM. Perceptions of the coronavirus and COVID-19 testing and vaccination in Latinx and Indigenous Mexican immigrant communities in the Eastern Coachella Valley. BMC Public Health. 2022;22(1):1019. doi: 10.1186/s12889-022-13375-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Strong C, Lee S, Tanaka M, Juon HS. Ethnic differences in prevalence and barriers of HBV screening and vaccination among Asian Americans. J Community Health. 2012;37(5):1071–80. doi: 10.1007/s10900-012-9541-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.World health organization . Ten Threats to global health in 2019. 2022. [accessed 2022 Sep 10]. https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
- 76.Gehlbach D, Vázquez E, Ortiz G, et al . COVID-19 Testing and Vaccine Hesitancy in Latinx Farm-Working Communities in The Eastern Coachella Valley. Preprint. Res Sq. 2021;rs.3.rs-587686. Published 2021 Jun 25. doi: 10.21203/rs.3.rs-587686/v1. [DOI] [Google Scholar]
- 77.Kricorian K, Civen R, Equils O. COVID-19 vaccine hesitancy: misinformation and perceptions of vaccine safety. Hum Vaccin Immunother. 2022;18(1). doi: 10.1080/21645515.2021.1950504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Thompson HS, Manning M, Mitchell J, Kim S, Harper FWK, Cresswell S, Johns K, Pal S, Dowe B, Tariq M, et al. Factors associated with racial/ethnic group–based medical mistrust and perspectives on COVID-19 vaccine trial participation and vaccine uptake in the US. JAMA Netw Open. 2021;4(5):e2111629. doi: 10.1001/jamanetworkopen.2021.11629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Netfa F, Tashani M, Booy R, King C, Rashid H, Skinner SR. Knowledge, attitudes and perceptions of immigrant parents towards Human Papillomavirus (HPV) vaccination: a systematic review. Trop Med Infect Dis. 2020;5(2):58. doi: 10.3390/tropicalmed5020058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Phadke VK, Bednarczyk RA, Salmon DA, Omer SB. Association between vaccine refusal and vaccine-preventable diseases in the United States a review of measles and pertussis. JAMA. 2016;315(11):1149. doi: 10.1001/jama.2016.1353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Berman RS, Smock L, Bair-Merritt MH, Cochran J, Geltman PL. Giving it our best shot? Human Papillomavirus and Hepatitis B virus immunization among refugees, Massachusetts, 2011–2013. Prev Chronic Dis. 2017;14. doi: 10.5888/pcd14.160442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Omer SB, Richards JL, Ward M, Bednarczyk RA. Vaccination policies and rates of exemption from immunization, 2005-2011. N Engl J Med. 2012;367(12):1170–71. doi: 10.1056/NEJMc1209037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.US Citizenship and Immigration Services . Vaccination requirements. 2021. Oct 21 [accessed 2022 Sep 10]. https://www.uscis.gov/tools/designated-civil-surgeons/vaccination-requirements.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.