
Figure 1.
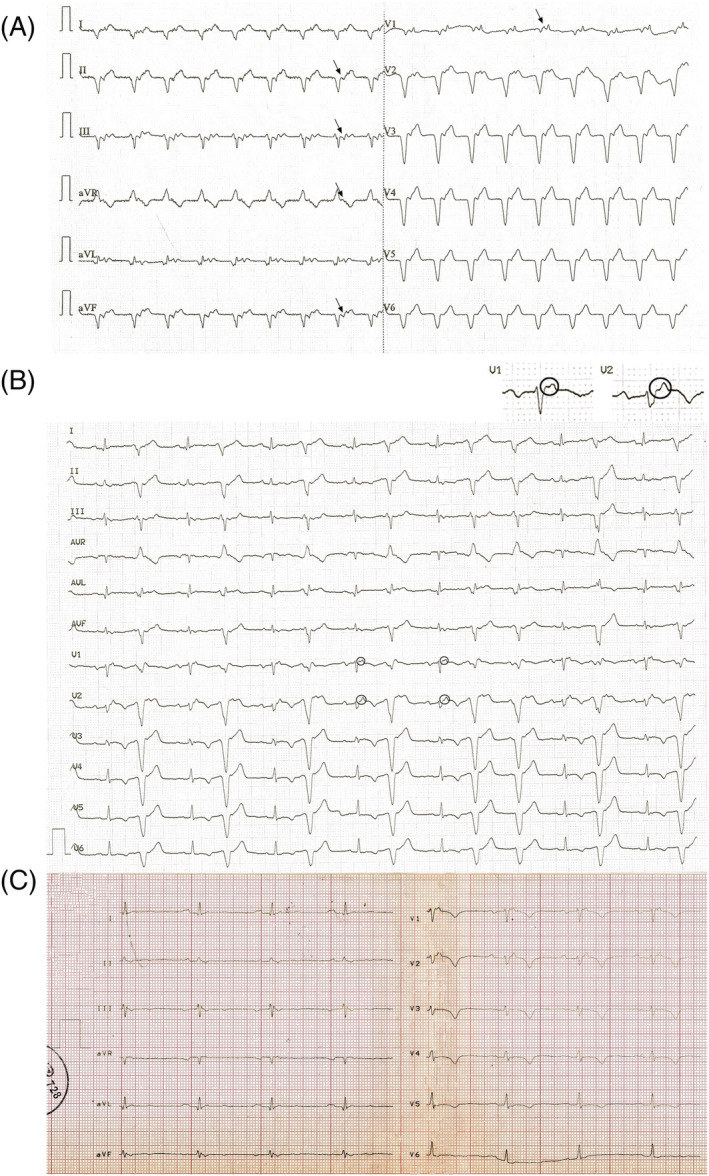
Preadmission ECGs and the ECG recorded at our department after admission. (A) Preadmission ECG tracing recorded right before admission to our department. A 105 b.p.m. ventricular rhythm with 1:1 VA conduction is shown. Arrows show the retrograde P waves. The VT diagnosis is based on the absence of RS complex in the chest leads (Brugada algorithm), the presence of initial R wave in lead aVR (Vereckei algorithm), the negative concordance pattern in the chest leads and the fact that the QRS morphology does not match that of a bundle branch block or a combination of bundle branch block and hemiblock. (B) ECG tracing recorded right before admission to our department. Sinus rhythm with ventricular premature beats (VPB) with an identical morphology to the beats of ventricular rhythm demonstrated in (A) arranged in a bigeminal pattern with the exception of two consecutive coupled VPBs is shown. Small circles denote the epsilon waves in leads V1 and V2, which are also highlighted in a magnified view. For further explanation, see text. (C) ECG tracing recorded at our department after admission, showing sinus rhythm without VPBs, otherwise essentially identical to the ECG tracing showed in (B), with the exception that the PR interval is longer: 230 ms.