
FIGURE 3.
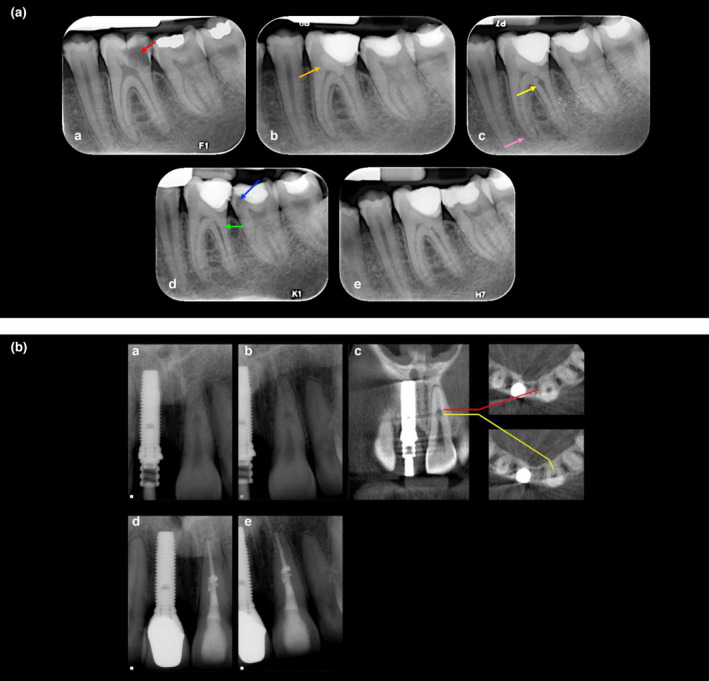
(a) Internal inflammatory resorption following pulpotomy. A 18‐year‐old male patient with an extensive carious lesion on tooth 36 with symptoms of irreversible pulpitis (a) preoperative periapical radiograph showing the deep carious lesion (red arrow), (b) a Biodentine pulpotomy (orange arrow) was carried out, (c) a 3‐month review confirmed that the tooth was asymptomatic; however, the radiographic examination revealed internal inflammatory root resorption (yellow arrow) on the distal canal, diffuse calcification on the mesial canals and apical widening of the periodontal ligament on the mesial root (pink arrow). After discussing the treatment options, as they were asymptomatic, the patient decided to have their tooth reviewed on a periodic basis. (d) A 15‐month review revealed that the tooth was asymptomatic, and there were no signs of endodontic or periodontal disease associated with the tooth, radiographic assessment confirmed that the IIR has spontaneously resolved and may have become IRR (green arrow), but did reveal secondary caries in tooth 37 (blue arrow), which was restored, (j) 24‐month review. (b) Internal replacement resorption. (a, b) Periapical radiographs of a maxillary left central incisor with radiographic signs of IRR; note the symmetrical nature of the defect, which remains centred with the parallax view, and the radio‐opaque nature of its coronal aspect. This patient sustained a dental traumatic injury 9 years previously, (c) CBCT slices through the same tooth reveals a calcified tissue in the coronal part of the lesion. (d, e) Obturated tooth and a 2‐year review radiograph demonstrating the irregular borders of the defect that have been obturated with thermoplastiicized gutta percha (Reprinted from Journal of Endodontics, Vol 36, Patel S, Ricucci D, Durak C, Tay F. Internal root resorption: a review. Journal of Endodontics pages 1107–1121, Copyright (2010) with permission from Elsevier)