
Figure 2. Microbiota injury patterns in allo-HCT are conditioning regimen-specific.
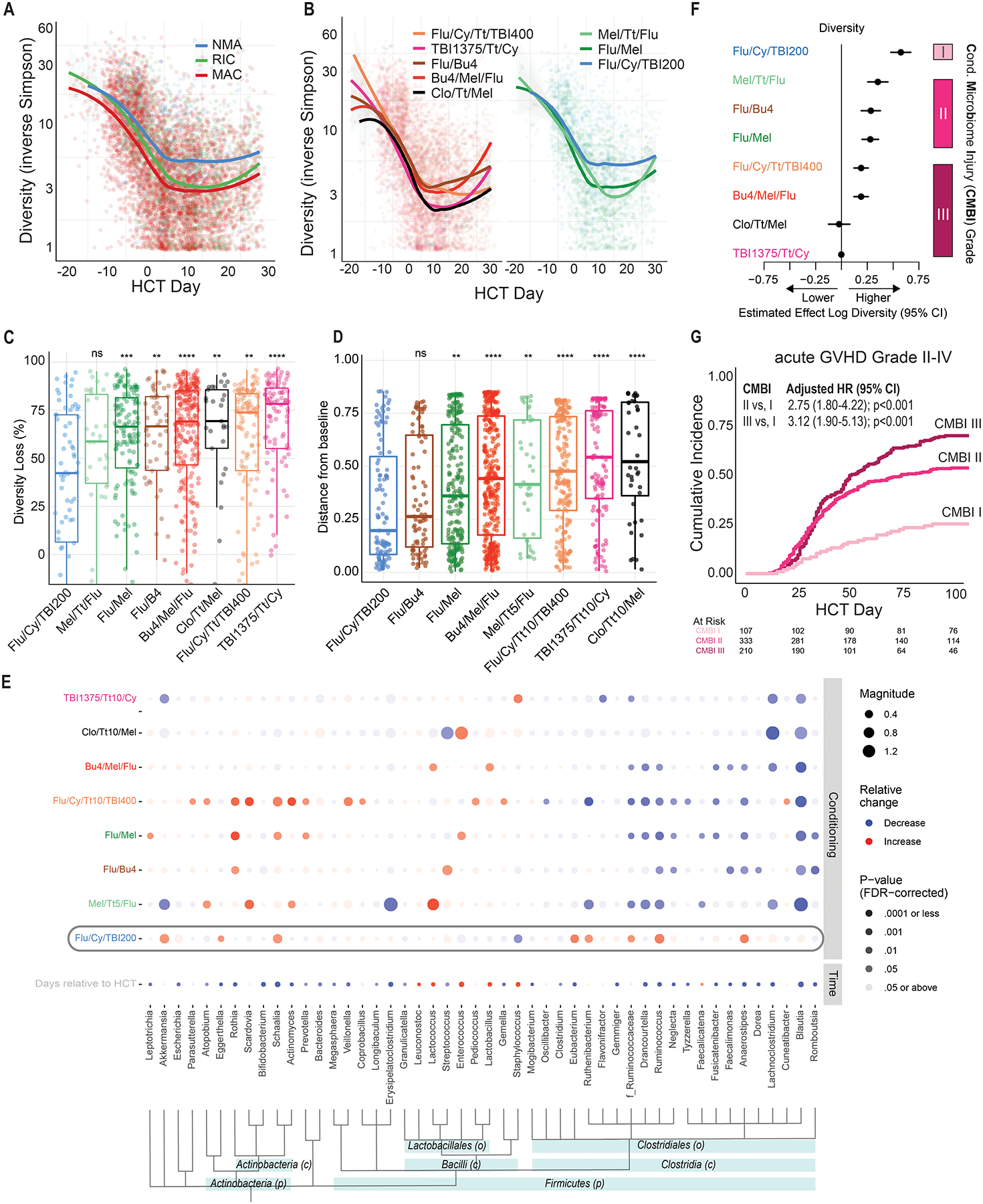
(A) Fecal microbiota α-diversity declines most in recipients of MAC and the least in recipients of NMA conditioning (Table S2). Each point is a stool sample whose α-diversity is plotted over time relative to transplantation. The smoothed curves plots are moving averages of recipients of different regimens. (B) Distinct patterns of α-diversity dynamics can be observed among recipients of specific conditioning regimens. Five MAC regimens are plotted in the left panel, two RIC and one NMA regimen are plotted in the right panel. (C) In a patient-level pair-matched analysis of the earliest sample collected before (days −20 to −1) and earliest sample after conditioning (days 0 to 10), the NMA regimen Flu/Cy/TBI200 was associated with the least reduction in diversity (42%). In contrast, the MAC regimens were associated with the greatest reduction (69%−78%). Regimens were compared to Flu/Cy/TBI200 with the Wilcoxon signed-rank test. (D) Microbiome dissimilarity, as determined by applying multidimensional scaling to the Bray-Curtis distance matrix, between samples collected at days 0 and 12 was significantly increased in all conditioning regimens except Flu/Cy/TBI200. The greatest distance was in the myeloablative regimen Clo/Tt/Mel. (E) A multivariable MaAsLin2 model(22) adjusting for time of sampling and conditioning regimens reveals a differential association between microbial taxa and conditioning regimens. Bacteria are ordered by taxonomical ranking. ASVs that could not be classified to the genus level were analyzed at the family level, as indicated by f_Ruminococcaceae. Flu/Cy/TBI200, highlighted with a gray rounded rectangle, was associated with the preservation of members of the Clostridia class. (F) A grading scheme classifying regimens into three categories of microbiota injury (low [I], intermediate [II], and high [III]) based diversity reduction between days −20 to 30 was introduced. The estimated effect on diversity of each regimen was derived from a generalized estimating equation (Table S4) regression model, adjusting for time, age, sex, exposure to GVHD prophylaxis, antibiotics, and conditioning. (G) Patients who received unmodified grafts had a higher incidence of acute GVHD Grade II-IV with regimens categorized as having greater microbiota toxicity. CMBI hazard ratios are derived from a multivariable Cox-regression adjusting for age, sex, comorbidity burden, donor and HLA matching, and GVHD prophylaxis.
* p ≤ 0.05, ** p ≤ 0.01, *** p ≤ 0.001, **** p ≤ 0.0001
HCT – allogeneic hematopoietic cell transplantation; MAC – myeloablative conditioning; RIC – reduced-intensity conditioning; NMA – nonmyeloablative conditioning; CMBI – conditioning-associated microbiota injury; graft-versus-host disease (GVHD);