

Abstract
Evaporative cooling is an energy efficient form of air conditioning in dry climates that functions by pulling hot, dry outdoor air across a wet evaporative pad. While evaporative coolers can help save energy, they also have the potential to influence human health. Studies have shown residential evaporative coolers may pull outdoor air pollutants into the home or contribute to elevated levels of indoor bioaerosols that may be harmful to health. There is also evidence that evaporative coolers can enable a diverse microbial environment that may confer early‐life immunological protection against the development of allergies and asthma or exacerbate these same hypersensitivities. This review summarizes the current knowledge of bioaerosol and microbiological studies associated with evaporative coolers, focusing on harmful and potentially helpful outcomes from their use. We evaluate the effects of evaporative coolers on indoor bacterial endotoxins, fungal β‐(1 → 3)‐D‐glucans, dust mite antigens, residential microbial communities, and Legionella pneumophila. To our knowledge, this is the first review to summarize and evaluate studies on the influence that evaporative coolers have on the bioaerosol and microbiological profile of homes. This brings to light a gap in the literature on evaporative coolers, which is the lack of data on health effects associated with their use.
Keywords: bioaerosol, endotoxin, evaporative cooler, house dust mite, swamp cooler, β‐(1 → 3)‐D‐glucan
Practical Implications.
Bioaerosol and microbiological exposures in the residential environment play an important role in disease as well as in healthy immune system development, particularly in children.
In this review, we discuss the potential for evaporative coolers to change the bioaerosol and microbiological profile of homes, specifically related to bacterial endotoxins, β‐(1 → 3)‐D‐glucan, house dust mite allergens, and microbial species, including Legionella pneumophila.
Findings from exposure assessment and health studies are reviewed, with a focus on both deleterious and potentially favorable health outcomes associated with evaporative cooler use.
Evidence is presented for both harmful and helpful exposures, as well as significant limitations in the quality and quantity of current data on this topic.
1. INTRODUCTION
Evaporative cooling is one of the oldest and most energy efficient forms of air conditioning used in hot, dry climates. Historically, there are several examples of passive evaporative cooling methods, which relied on natural airflow. In the Southwest U.S., Native Americans splashed water on the tops of arbors in hot weather, which may have cooled the shaded area under the arbor by as much as 10 degrees. 1 Similar approaches were used by Western U.S. settlers who covered wall openings with damp burlap. 2 , 3 Other historic examples include the practice in India of hanging “tatties”, wetted screens made from the roots of khus khus (cuscus) grass, over windward doorways and window openings during hot summer months, 3 , 4 and the introduction of water into wind towers in traditional Middle Eastern architecture. 5 , 6 Early mechanical methods incorporated the use of fans to improve airflow across wetted media. As early as 1905, British soldiers' barracks in India were air conditioned by arranging tatties over fans to cool supply air coming into the building. 7 In the early 1930s in the Southwest U.S., homemade evaporative coolers were fashioned by covering a wooden box with burlap or other cloth. An electric fan was then used to blow outdoor air across the wetted cloth into the home. 2 , 3 The advent of mass‐produced mechanical evaporative air coolers (ECs) in the Southwest U.S. in the late 1930s was a major factor in opening up the otherwise hostile summer climate of Arizona and neighboring states to population growth (Figure 1A). 2 , 3
FIGURE 1.
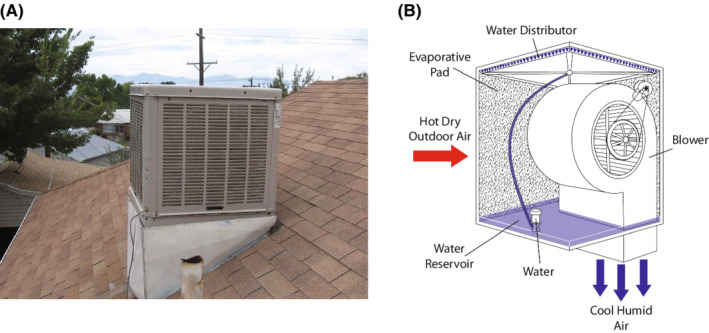
(A) Common roof mounted residential direct evaporative cooler used in Rocky Mountain States, U.S. (B) Cooling process involves pulling hot, dry outdoor air through a wetted evaporative pad. As water evaporates from the cooling pad into the air, sensible heat in the air is transferred to latent heat in the form of water vapor. The cooled air is then blown indoors.
Direct evaporative coolers are the simplest and most common type of EC used in residences in arid and semi‐arid climates. 3 , 8 Indirect evaporative coolers are available, but rarely used in residences in dry climates due to the high efficiency and low cost of direct evaporative coolers. 9 For the purposes of this review, EC will refer to residential direct evaporative air coolers, also known as “drip coolers”, “desert coolers”, and “swamp coolers”. ECs work by pulling hot, dry outdoor air across a wet evaporative pad typically made from aspen wood shavings, other natural fibers, or corrugated cellulose materials (Figure 1B). 3 , 8 , 10 , 11 The evaporative pad is kept moist during operation by an electric pump that sends water to distribution troughs at the top of the evaporative pads. As ambient air passes through the wet evaporative pads the water evaporates. During evaporation, water molecules in the evaporative pad absorb heat from outdoor air as they change phase from liquid to vapor. 3 , 12 As a result of evaporation, ECs lower the air temperature while simultaneously increasing the amount of water vapor in the air. Non‐evaporated water in the evaporation pads is drained by gravity into the water reservoir (sump) where it is recirculated through the system. The cool, humidified air is blown into the house by a fan (Figure 1B). 13 , 14
Evaporative air coolers, because they rely on heat transfer from the evaporation of water, do not work well in humid environments. For comfort cooling, ECs are less effective once the wet‐bulb temperature reaches 21°C (69.8 °F). 8 Thus, they are most effective in dry and temperate climates that experience year‐round or seasonal low humidity and high outdoor temperatures. The World Bank estimated in 1998 that 20 million residential ECs were used globally, primarily in Western Australia, the Middle East, Northern, Eastern, and Southern Africa, parts of the Indian subcontinent, Northern Mexico, the Mediterranean, and the Southwest and Rocky Mountain States in the U.S. 8 At the turn of the 21st Century, EC use in the U.S. varied considerably, from up to 90% of homes in West Texas, 16 to approximately 29% of homes in the Rocky Mountain States, 17 to 8% of homes in California. 18 In 2004, about 13% of homes in Australia had EC units. 19 Based on the 2015 Residential Energy Consumption Survey (RECS), there are approximately 2.3 million (2.0%) homes in the U.S. using EC units, primarily in the southwest region. 20 , 21
2. BACKGROUND
Vapor‐compression (refrigerated) air conditioning (AC) makes up almost 90% of the global air conditioning market. 22 Residential AC units operate by transferring heat from indoor air to a refrigerant (e.g. hydrofluorocarbons), moving the refrigerant outdoors, and then releasing the heat to the environment. 23 , 24 The principal of operation and system components for a typical residential AC system are shown in Figure 2.
FIGURE 2.
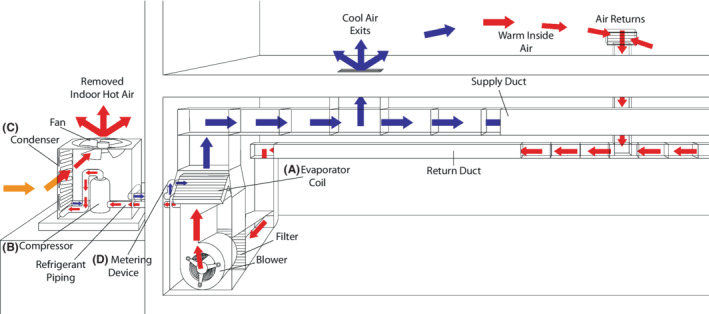
Principle of operation and structure of a vapor compression air conditioning system. (A) Room air is passed over the evaporator coil. Heat from indoor air provides latent heat of vaporization to refrigerant, causing it to boil. Refrigerant leaves the evaporator as a low‐pressure vapor. (B) Vapor enters the compressor, picking up additional heat from mechanical parts and compression. (C) High pressure, superheated vapor enters the condenser. Ambient air is pulled across the condenser by a fan. Refrigerant releases sensible heat as it changes phase from vapor to liquid. (D) High pressure liquid refrigerant enters metering device (not shown), leaves as low‐pressure, subcooled liquid/vapor mixture before entering the evaporator coil.
Differences in the mode of operation between EC and AC units may have important impacts on the indoor environment. To conserve energy, residential AC units recirculate indoor air. Yamamoto et al. (2009) reported the median air changes per hour (ACH) was 0.38 for Houston, TX (USA), homes using AC. 25 In contrast, EC units introduce large volumes of outdoor air into the home. Macher & Girman (1990) reported 8.2–13.0 ACH in a 272 m3 EC home. 15 Low ACH in AC homes may limit entrainment of outdoor bioaerosols and pollutants into the home, whereas high ACH rates in EC homes may pull outdoor pollutants into the home, 26 , 27 while simultaneously diluting indoor contaminants. 8 Another important distinction is that AC units remove moisture from indoor air, thus lowering relative humidity (RH) in the home. 28 , 29 This occurs as water vapor condenses onto the cold evaporator coil as home air passes through the system (Figure 2). Lower indoor RH may hinder microbial growth in the home, leading to decreased bioaerosols. 30 In addition, AC filters may reduce airborne bioaerosols, such as endotoxin, by capturing particulate matter as indoor air is circulated through the system. 31 Conversely, EC units add significant moisture to indoor air as water evaporates from cooling pads into the air being blown into the home (Figure 1B). Added moisture from EC units can raise indoor RH 10%–16% in single‐family dwellings. 32 , 33
Concerns about climate change and a growing demand for energy make residential ECs an appealing alternative to AC in dry climates. 34 , 35 , 36 ECs provide 50%–80% energy savings compared to AC units, 3 , 8 and in recent years, government agencies and power companies in the Southwest U.S., California, and the Rocky Mountain States, as well as Australia have offered incentives for the purchase or servicing of qualified EC units to reduce residential energy demand. 37 , 38 , 39 , 40 , 41 However, incentive programs tend to focus on the environmental and cost benefits of ECs with no mention of potential health effects. Juxtaposed with this renewed interest in energy savings is a growing body of evidence that ECs have the potential to influence human health, prompting this review.
2.1. Entrainment of outdoor air pollution
To date, a few studies show that particulate air pollution levels in EC homes are generally lower than outdoor levels, with indoor/outdoor (I/O) ratios ranging from ~0.6 to 0.9 for airborne particulate matter (PM) with an aerodynamic diameter ≤2.5 μm (PM2.5), and ~0.5 to 0.6 for airborne PM ≤10 μm (PM10). 16 , 42 , 43 Paschold et al. (2003) 44 found similarly low I/O ratios for elemental constituents in PM10 and PM2.5 in EC homes in El Paso, TX. One explanation for this is that cooler pad fibers grow in diameter when wet, increasing particle impaction while simultaneously reducing particle bounce. They thus act as an effective PM filter, albeit with decreasing efficiency as particle diameters decrease. 16 ECs also move large volumes of air through the home, resulting in several air changes per hour, 15 which rapidly dilutes indoor PM sources. 8 One study found buildings with ECs had I/O PM ratios greater than 1.0, but this study was limited to two schools and one private home. 45 Although EC cooler pads may reduce entrainment of outdoor PM into homes, they may still contribute significantly to the entrainment of other hazardous pollutants. Nazmara et al. (2020) found traffic‐related polycyclic aromatic hydrocarbons (PAHs) in dust samples collected from EC ducts in Tehran, Iran. 26 Additionally, some gas‐phase pollutants may not be captured efficiently by cooler pads. Raysoni et al. (2013) found I/O ratios ~1.0 for NO2, and I/O ratios ranging from 0.6 to 1.2 for mean concentrations of benzene, toluene, ethylbenzene, and xylenes at two schools equipped with ECs. 27 Thus, additional research is needed to fully understand the role ECs play in drawing outdoor air pollution into homes.
2.2. Introduction of bioaerosols into homes
Bioaerosols are defined as airborne particles ranging in size from 0.001 to 100.0 μm that originate from plants, animals, viruses, and living or dead microorganisms and include cellular fragments and byproducts of microbial metabolism. 46 , 47 Due to the nature of how evaporative cooling works, ECs have the potential to introduce bioaerosols into homes through three mechanisms (Figure 3). First, ECs may pull bioaerosols into homes from outdoor air. However, many outdoor bioaerosols, including pollen, spores, mold, and plant parts, have aerodynamic diameters >2.5 μm, 48 and thus may be partially filtered out as they pass through wetted cooler pads (Figure 3A). Second, ECs may distribute bacteria and fungi, or their cellular components such as endotoxin and β‐(1 → 3)‐D‐glucan, into homes through microbial growth in sump water and cooling pads (Figure 3B). 15 , 49 Endotoxin derived from bacterial cell walls, and β‐(1 → 3)‐D‐glucan, an important component of fungal cell walls, have drawn attention in the literature due their associations with respiratory health effects. 50 , 51 , 52 , 53 , 54 , 55 , 56 , 57 , 58 Finally, due to increased humidity in the home, ECs may create an ecological niche for house dust mites in arid or semi‐arid climates by providing enough moisture during cooling months for dust mites to maintain water balance and reproduce (Figure 3C). 33 , 59 House dust mite allergens such as Der p 1 and Der f 1 are associated with the development and exacerbation of asthma and other allergic diseases. 60 , 61 , 62 , 63 , 64
FIGURE 3.
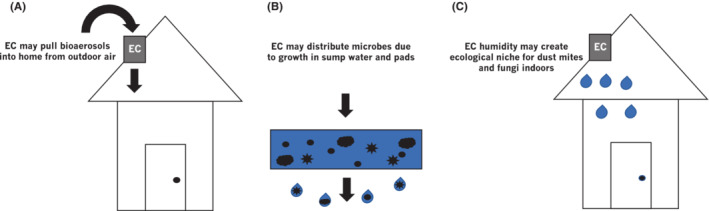
Evaporative coolers have the potential to introduce bioaerosols into homes through three mechanisms. (A) Bioaerosols present in outdoor air can be pulled into the home through the evaporative cooler, (B) Cooling pads and sump water may serve as reservoirs for microbial growth, and (C) Evaporative coolers increase indoor humidity, potentially creating an ecological niche for house dust mites and mold.
2.3. Health effects of evaporative cooler use
While summarizing and analyzing the available literature on EC‐related endotoxin, β‐(1 → 3)‐D‐glucan, and house dust mite allergens that have deleterious respiratory health effects, this review presents some limited evidence that EC‐related bioaerosols may provide important immunological benefits during early life, consistent with the “hygiene hypothesis”. 66 , 67 , 68 Furthermore, recent studies highlight the importance of the residential microbiome in shaping our immune responses during early childhood. 69 , 70 , 71 It is important to note that our understanding of the hygiene hypothesis and its health implications are continuing to be refined (e.g. old friends hypothesis and microflora hypothesis) and remain controversial to some. 72 , 73 , 74 , 75 , 76 For young children, the home provides necessary exposures to bioaerosols and a diverse microbial environment during the critical early‐life window for healthy immune development and influences adaptive immune cell lineage commitment, memory cell generation, and immune training of innate immune cells. 69 , 77 Several existing reviews discuss the design, thermal, and economic performance of ECs. 14 , 34 , 36 , 65 However, to our knowledge, this is the first review on associations between residential ECs and indoor bioaerosols and microbial exposures and their potential influences on human health.
3. METHODS
This is a nonsystematic review of medical, public health, and environmental health‐related literature, with a focus on residential ECs. We primarily searched Google Scholar and MEDLINE (EBSCO) databases with no restrictions for date of publication. In addition, papers meeting our search criteria were reviewed to find references that did not appear in our database searches. Search terms included “evaporative cooler”, “swamp cooler”, and “desert cooler” in conjunction with variations of the following terms: “house dust mite”, “house dust mite allergen”, “endotoxin”, “fungi”, “bioaerosol”, “health”, “children's health”, “allergen(s)”, “atopy”, “Legionnaire's Disease”, “Legionella”, “Pontiac Fever”, “air pollution”, “particulate matter”, “pollen”, “mold”, “mold spores”, “bacteria”, “epidemiology”, “disease”, “immunity”, and “infection”. Papers and published abstracts that reported results related to residential ECs and bioaerosols, air pollution, microorganisms, and human health were included in the review.
4. RESULTS and DISCUSSION
4.1. Epidemiology and case studies
The available data on health effects associated with EC use come from case studies and a few epidemiological studies (Table 1). Marinkovich & Hill (1975) reported a nearly fatal case of hypersensitivity alveolitis in an 11‐year old girl that was associated with a residential EC unit. 78 Laboratory results found thermophilic actinomycetes in the EC cooler pads, and the patient's serum contained antibodies for Micropolyspora faeni, a common microorganism implicated in cases of farmer's lung. 79 , 80 The authors suggested that exposure occurred as spores of M. faeni, were dislodged from the cooler pads and dispersed into the home while the EC was running. Al‐Zubaidy (1987) cultured pathogens on nutrient agar from EC air supplied to a medical laboratory in Baghdad, Iraq, including Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella pneumonia, Escherichia coli, and Serratia marcescens. These same pathogens were present in sump water from the air cooler; however, no cases of illness from these agents were identified. 81
TABLE 1.
Epidemiological and case study evidence for health effects associated with evaporative coolers
| Study | Population/location | No. Participants | Health outcome | Findings |
|---|---|---|---|---|
| Marinkovich & Hill (1975) 78 | Case study of 11‐yr old girl in rural area of the central California valley | 1 | Hypersensitivity alveolitis | Illness was likely caused by exposure to spores of Micropolyspora faeni introduced into the home by evaporative cooler |
| Aldous et al. (1996) 82 | Infants enrolled in health maintenance organization, Tucson, AZ (USA) area 1980–1984 | 936 | Risk of wheezing lower respiratory infection (LRI) | Significant risk of LRI for infants in EAC homes (OR = 1.8, 95% CI = 1.1–3.0) |
| Prasad et al. (2009) 83 | Allergy & asthma patients seen at University of Nevada School of Medicine Clinic Reno, NV (USA) 2007–2008 | 190 | Positive skin prick test for mold and house dust mite allergens | Individuals living in EAC homes were significantly more likely to have positive skin test to dust mite allergens (chi‐square, 6.2; p = 0.013) and at least one mold (chi‐square, 10.5; p = 0.001) |
| Izadi et al. (2018) 84 | Retrospective review of atopic Colorado residents <21 years old seen at National Jewish Health from 2008–2017 |
9286 (mold cohort) 8503 (dust mite cohort) |
Positive skin prick test for mold and house dust mite allergens |
EACs were not associated with sensitization to mold (relative risk 1.03, 95% CI = 0.96–1.10, p = 0.4255) or house dust mite allergen (relative risk 1.01, 95% CI = 0.91–1.12, p = 0.8452) Allergic rhinitis was significantly lower (p = 0.0215 and p = 0.0257 for the dust mite and mold cohorts, respectively), and asthma trended lower (p = 0.0505 and p = 0.0556 for the dust mite and mold cohorts, respectively), among patients living in homes with EAC units |
To date, there are few epidemiological studies regarding health effects associated with EC use. Aldous et al. (1996) studied lower respiratory tract illness (LRI) among infants (age 0–1) who were health maintenance organization patients (N = 936) in the Tucson, Arizona (USA) area from 1980 to 1984. 82 The primary study question was whether home environmental factors, including perceived neighborhood dustiness, type of home cooling and heating systems, type of cooking fuel, and number of indoor pets (dogs and cats), influenced the risk of LRI during the participants' first year of life. Among children living in homes with ECs (n = 731), 24% experienced wheezing LRI during the first year of life, compared to 15% of children living in homes (n = 141) without ECs (OR = 1.8, 95% CI = 1.1–3.0). The authors concluded that, although ECs are only used during summer months, they may introduce bioaerosols (pollen, mold, dust mite allergens) into homes that persist into winter months, and subsequent exposure to these bioaerosols may make children more susceptible to viral LRI.
ECs introduce moisture into homes, 32 , 33 and thus have the potential to create an ecological niche for indoor mold growth and/or survival and house dust mites in arid and semi‐arid regions. Prasad et al. (2009) studied patients (N = 190) with asthma and allergic rhinitis at the University of Nevada School of Medicine (USA) from August 2007 to June 2008. 83 This cross‐sectional study evaluated relationships between positive skin prick tests for common allergens and the presence of EC (n = 59) or central air conditioner (n = 124) in the home. Among participants with ECs, 42% were allergic to at least one mold compared to 25% of participants with AC (χ2, 10.5; p = 0.03). Similarly, among participants with ECs, 34% had a positive skin prick test for house dust mite allergens compared to 21% of participants with AC (χ2, 6.2; p = 0.013). The authors also reported a higher prevalence of skin prick reactivity to dust mites and mold among study participants <6 years of age, which they attributed to increased time spent indoors at home compared to adults.
A much larger, more recent pediatric cohort study by Izadi et al. (2018), however, found no association between EC use and dust mite allergen or mold sensitivity. 84 In this study, the authors conducted a retrospective review of data from patients <21 years of age seen at National Jewish Health hospital (Colorado, USA) from 2008 to 2017. Among patients for whom house dust mite test results were available (n = 8503), 922 lived in an EC home, of which 284 (28.6%) had sensitivity to house dust mite allergens. For patients with no EC (n = 7511), 2128 (28.3%) had sensitivity to house dust mite allergens (relative risk 1.01, 95% CI = 0.91–1.12, p = 0.8452). Findings for mold sensitivity were similar. Among patients for whom mold sensitivity test results were available (n = 9286), 1092 lived in an EC home, of which 487 (44.6%) were allergic to at least one mold. For patients with no EC (n = 8194), 3550 (43.3%) were sensitive to at least one mold (relative risk 1.03, 95% CI = 0.96–1.10, p = 0.4255). The authors concluded that ECs do not increase atopic children's sensitization to house dust mites or mold in Colorado's dry climate.
The literature is likewise scant regarding evidence for positive health outcomes associated with EC use. The large cohort study by Izadi et al. (2018), found the prevalence of allergic rhinitis was significantly lower among patients living in homes with ECs (p = 0.0215 and p = 0.0257 for the dust mite and mold cohorts, respectively). Furthermore, they reported a lower prevalence of asthma among children in EC homes that was trending significant (p = 0.0505 and p = 0.0556 for the dust mite and mold cohorts, respectively). 84 Differences in the prevalence of allergic rhinitis and asthma between children in EC and non‐EC homes were relatively small. Based on evidence from several studies examining the hygiene hypothesis and the residential microbiome, the critical window for exposure to the diverse microbiome necessary for healthy immune system development is likely very early, perhaps within the first few years of life. 69 , 70 , 71 , 75 , 76 , 85 It is conceivable that ECs provide some immunological benefits to children.
With the exception of Aldous et al. (1996), who used a prospective cohort study design, the available epidemiological studies were not designed to answer the most salient questions about health effects associated with EC use, if such associations exist. The contradictory findings between Izadi et al. (2018) and Prasad et al. (2009) may be explained by sample size. Izadi et al. had over 40 times the number of participants as Prasad et al. However, it should be noted that both studies used cross‐sectional designs based on current EC use. The results of both studies, therefore, may have been subject to misclassification bias, as they did not account for patients who may have moved from EC to AC homes, or vice versa, prior to study enrollment, which was very likely. According to the U.S. Census Bureau, approximately 20% of U.S. households with children ≤6 years of age move per year. 86 This may have affected the results of Izadi et al. more so than Prasad et al., given the mean ages of participants, which were ~9.0 years and 5.4 years, respectively. Furthermore, neither study provided environmental data on home allergen/mold levels or indoor RH. Thus, relationships between health outcomes and EC, dust mite allergen, and mold exposures are obscured in both studies. Prospective studies may be needed to fully understand the immunological consequences of early‐life exposures in EC homes.
Whether or not antigen and/or microbial exposure due to air conditioning type can be helpful or harmful is a complicated issue that remains unclear. There are more than 1600 genes involved in innate and adaptive immune responses, yet at birth the immune system is relatively immature and must develop over the course of one's life. 87 Early post‐natal life microbial exposure is essential to immune system development, influencing adaptive immune cell lineage commitment, memory cell generation, and immune training of innate immune cells. 69 , 77 The microbiota individuals are exposed to plays a key role in the education and development of the immune system. 87 , 88 Epidemiological evidence seems to support this claim, showing that children with older siblings, early daycare attendance and exposure to livestock have a lower incidence of allergic disease. 89 Children living in urban environments have also been shown to be protected against asthma development if their indoor home environment closely resembles the indoor microbiota found in farm homes. 90 The hygiene hypothesis mainly focuses on microbial exposures from the environment, food and drink, and domestic animals. The “biodiversity hypothesis” proposes that a decrease in microbiological biodiversity is likely related to an increase in inflammatory disease. 91 Previous studies document that ECs influence indoor levels of endotoxin, 49 , 92 , 93 β‐(1 → 3)‐D‐glucan, 93 and house dust mite allergens 33 , 59 relative to homes with AC or no air conditioning. In addition, a growing body of evidence suggests that the indoor microflora of EC homes differs from homes with AC systems. 49 , 94 , 95 These bioaerosols and their associations with EC use are discussed in the following sections.
4.2. Evaporative coolers and bacterial endotoxin
Endotoxin, also known as lipopolysaccharide or LPS, is a soluble component on the cell wall of Gram‐negative bacteria. 96 It is composed of a hydrophobic lipid section (lipid A), a hydrophilic core polysaccharide chain and a repeating hydrophilic O‐antigenic oligosaccharide side chain. 97 Endotoxin is a pathogen associated molecular pattern (PAMP) that can be bound and recognized as foreign by pathogen recognition receptors (PRRs) located on various cells of the immune system. 98 High levels of endotoxin in the body can lead to inflammation and vasodilation when recognized by the transmembrane protein toll‐like receptor 4 (TLR4). 99 , 100 TLR4 is a PRR expressed on a wide variety of cell types, including dendritic cells, macrophages, neutrophils and B cells. Endotoxin binding of TLR4 activates transcription factor NF‐κB, and the subsequent production of pro‐inflammatory cytokines. 100 Development of asthma and allergic disease are attributed to a combination of genetic and environmental factors. Research has shown that two missense mutations located in the extracellular domain of the TLR4 receptor are associated with differences in reaction to inhaled endotoxin. Heterozygous individuals demonstrated a hypo‐responsive phenotype to endotoxin. 96 , 101
Early life exposure to endotoxins may be protective against the development of asthma and other allergic diseases later in life. 66 , 67 This can be observed in the Amish and Hutterite communities. Both populations share common ancestry, but asthma is 4–6 times lower in Amish children, while Amish dust endotoxin levels are 6.8 times higher than levels found in Hutterite homes. 85 Mice exposed to this Amish dust were protected from development of asthma, while mice exposed to Hutterite dust were not. Similarly, a study of children in the Alps showed an inverse relationship between endotoxin exposure and the prevalence of asthma. 102 However, exposure to endotoxin in the home is also known to obstruct airflow in adults and children who are already asthmatic. 55 , 56 , 57
Several housing factors are associated with increased indoor residential endotoxin levels, including the presence of rugs and carpet, 103 , 104 lack of cleanliness, 105 , 106 living on a farm or contact with farm animals, 103 , 107 , 108 having indoor pets, 30 , 103 , 104 , 105 , 108 , 109 , 110 , 111 higher home occupancy, 104 , 105 , 108 , 109 , 110 the presence of cockroaches in the home, 105 and geographic location. 104 , 105 , 107 , 108 , 110 , 111 Endotoxin levels also appear to be influenced by heating, ventilation, and air conditioning (HVAC) systems (Table 2). Gereda et al. (2001) 30 found that house dust endotoxin levels in metropolitan Denver, CO were significantly lower in homes with AC systems compared to homes with no air conditioning or room air conditioners only. They attributed their findings to AC homes being mostly closed to the outdoor environment. They also suggested lower indoor RH in AC homes may have caused decreased bacterial growth on home surfaces, and thus lower indoor endotoxin levels. AC refrigeration coils condense water out of the air, thus lowering indoor RH. However, Thorne et al. (2009) found no association between AC use and indoor endotoxin levels 105 ; thus, additional research is needed to fully understand this relationship.
TABLE 2.
Reservoir dust levels of endotoxin and β‐(1 → 3)‐D‐glucan in EC and AC homes
| Study | Location/population | Bioaerosol | Surface sampled a | AC Type b | No. Homes | Endotoxin c (EU/mg) | β‐(1 → 3)‐D‐glucan (μg/mg) |
|---|---|---|---|---|---|---|---|
| Gereda et al. (2001) 30 | Low‐income homes of infants enrolled in asthma study, Metropolitan Denver, CO (USA) | Endotoxin | BF, MA, LF, UF, KF |
AC RAC EC No AC |
16 4 11 55 |
90.6 202.4 181.2 210.8 |
– – – – |
| Johnston et al. (2017) 92 | Middle‐income homes of university faculty and staff in Utah County, Utah (USA) | Endotoxin | BF, MA, LF, UF |
EC AC |
18 22 |
4.4 1.3 |
– – |
| Lemons et al. (2017) 49 | Homes of children in a pediatric allergy/asthma cohort study in Reno, NV (USA) area | Endotoxin | BF, MA |
EC AC |
5 6 |
162.3 58.1 |
– – |
| Johnston et al. (2019) 93 | Low‐income homes in Utah County, Utah (USA) |
Endotoxin, β‐(1 → 3)‐D‐glucan |
BF, MA, LF, UF |
EC AC |
20 28 |
3.6 1.3 |
0.45 0.17 |
All samples were collected from indoor house dust. BF, Bedroom floor; MA, Mattress; LF, Living room floor; UF, Upholstered furniture; KF, Kitchen floor.
EC, Evaporative Air Conditioner; AC, Vapor Compression Air Conditioner; RAC, Room Air Conditioner; No AC, No air conditioning.
Results for Gereda et al. (2001) in EU/mg were derived from their reported results by dividing EU/mL by 5 mg, the amount of house dust extracted per mL. Where multiple locations were sampled, results represent averages across sample locations.
In contrast to dehumidification caused by AC units, ECs create a warm, wet environment inside the cooler that is conducive to growth of Gram‐negative bacteria, potentially leading to higher levels of endotoxin in the home. Macher & Girman (1990) found bacteria levels in EC sump water as high as 1.0 × 105 CFU/mL after 9 weeks of operation during summer months. The predominant bacterial species were Gram‐negative. 15 Since this water is used to cool the hot air pulled from outside, evaporative cooling could be a source of endotoxin distribution in homes. 15 A significant limitation in this study, however, is that the results are based on a single EC from one home in California (USA). Macher & Girman's results may not be representative of bacteria levels in other ECs and may not be generalizable to ECs in other regions.
A growing number of studies using vacuum‐collected dust samples conducted in the Rocky Mountain region (USA) confirm that ECs are associated with higher indoor endotoxin levels (Table 2). In the 11 EC homes included in the study by Gereda et al. (2001) in the metropolitan Denver area, the geometric mean endotoxin concentration in house dust extracts was 906 EU/mL, compared to 453 EU/mL in AC homes. Johnston et al. (2017), in a study of middle‐income homes in Utah County, Utah, found house dust endotoxin levels (EU/mg) and endotoxin surface loads (EU/m 2 ) three to six times higher in EC (n = 18) compared to AC (n = 22) homes. 92 In a recent follow‐up study, Johnston et al. (2019) 93 reported similar findings among low‐income homes in the same county. In this study, house dust endotoxin levels (EU/mg) and endotoxin surface loads (EU/m2) were approximately three times higher in EC (n = 20) compared to AC (n = 28) homes. Similarly, Lemons et al. (2017), in a pediatric allergy/asthma cohort study in the Reno, NV (USA) area, found house dust endotoxin levels (EU/mg) from bedroom mattress and flooring dust were approximately three times higher in EC (n = 5) compared with AC (n = 6) homes (p = 0.039). 49
Time and cost constraints often restrict sample sizes in studies where residential environmental samples are collected, 112 and the studies referenced herein are no exception. While these studies may provide detailed results, they are nevertheless based on small sample sizes restricted to relatively small geographical areas. Endotoxin levels reported in these studies may not be representative of demographically different housing in the same community, or in housing in other U.S. or global regions. Furthermore, while there is consistency in the relative differences between EC and AC homes, endotoxin levels, inexplicably, vary by two orders of magnitude across studies (Table 2). What remains unclear is whether these findings reflect actual differences in endotoxin levels between sampling sites, or if differences can be explained by factors associated with sample collection or laboratory procedures. Furthermore, it is not clear if higher endotoxin levels in EC homes originated from bacterial growth in the cooler itself, bacterial growth on home surfaces resulting from higher RH in EC homes, or from environmental endotoxin being blown into the home. Evaporative cooler pads, as mentioned previously, may filter out as much as 40%–50% of outdoor airborne PM ≤10 μm (PM10). 16 , 42 , 43 Additional studies are needed to quantify the relative contributions of EC‐generated endotoxin and outdoor endotoxin being entrained into EC homes.
4.3. Evaporative coolers and β‐(1 → 3)‐D‐glucan
β‐(1 → 3)‐D‐glucan (β‐glucan) is a polysaccharide located in the cell wall of fungi, bacteria, yeast, algae, lichens, and plants such as oats and barley. 22 β‐glucans can trigger various immune responses including activation of neutrophils, macrophages, complement and possibly eosinophils. 113 , 114 , 115 , 116 , 117 β‐glucans are of particular interest for their immunomodulating properties. They have been shown to enhance cytotoxic activities of macrophages, 118 and functional maturation of dendritic cells 119 as well as to prevent cancer promotion and progression. 120 While exact mechanisms of how β‐(1 → 3)‐D‐glucan exposure might trigger asthma remain elusive, a few associations with asthma and β‐(1 → 3)‐D‐glucan have been discovered. A study looking at children from infancy to 7 years of age showed that children exposed to higher environmental relative moldiness index at the age of 1 year were more likely to develop asthma at 7 years of age. 121 Another study used a mouse model to further understand what exactly happens in β‐glucan exposure. Mice exposed to inhaled β‐glucan showed a slightly enhanced TH2 response while mice exposed to inhaled β‐glucan in conjunction with house dust mite allergens showed a significantly enhanced TH2 response. 122
Various studies suggest there is a link between fungal exposure and asthma, 123 , 124 however other evidence shows that perhaps β‐(1 → 3)‐D‐glucan is not actually the causative agent, with health effects actually being caused by inhaled endotoxin. 58 , 125 Burg et al. (2016) found mice that ingested WGP®, a preparation of β‐1,3/1,6‐glucans, had significantly reduced pulmonary eosinophils and TH2 cytokine production, indicating that β‐glucan could potentially mitigate asthma symptoms. 126 Kirmaz et al. (2005) showed β‐glucan administration to subjects with seasonal allergic rhinitis also demonstrated a reduction in IL‐4 and IL‐5 levels. 127 Sarinho et al. (2009) showed β‐glucan administration caused a reduction in asthmatic symptoms. 128 Despite no concrete evidence of β‐(1 → 3)‐D‐glucan being the causitive agent of asthma attacks, some studies show that exposure to inhaled β‐(1 → 3)‐D‐glucan increases asthma severity. 129 , 130 Research has shown that immune responses induced at mucosal surfaces create much more tolerogenic dendritic cells and certain types of regulatory T cells because of a need to discriminate between commensal flora and invading pathogens. 131 , 132 The seemingly contradictory reactions to ingested and inhaled β‐glucans are consistent with what is seen in mucosal and respiratory immune responses.
To date, the published literature, albeit scant, suggests there is some evidence that ECs may potentially lead to an increase in fungi and subsequent β‐(1 → 3)‐D‐glucan levels in the home (Table 2). Sneller & Pinnas (1987) cultured higher amounts, and isolated more species of fungi from air samples collected in EC (n = 15) vs. AC (n = 8) homes in the southwest U.S. 94 Likewise, Lemons et al. (2017), using genomic extraction and metagenomic analyses, found significant differences in the predominant fungal species in air samples from EC (n = 9) compared with AC (n = 11) homes in the Reno, NV (USA) area. 49 The authors also reported that fungal spores were three times higher in EC compared with AC homes when measured by quantitative PCR. It is important to note that the Sneller & Pinnas and Lemons et al studies did not specifically measure β‐(1 → 3)‐D‐glucan levels so that remains unknown. A recent study of low‐income homes in Utah (USA) by Johnston et al. (2019) found house dust β‐(1 → 3)‐D‐glucan concentration (μg/mg) and surface load (μg/m2) were 2.65‐fold and 3.64‐fold higher, respectively, in EC (n = 20) compared to AC (n = 28) homes. 93
The origins of increased fungi and β‐(1 → 3)‐D‐glucan levels in EC homes is not entirely clear. ECs introduce large volumes of ambient air into the home, and it is possible that the higher fungal and β‐(1 → 3)‐D‐glucan levels in EC homes can be explained by entrainment of outdoor air. Hirsch et al. (1978), in a study comparing AC (n = 6) with non‐air‐conditioned (n = 6) homes in Milwaukee, WI (USA), reported significantly lower spore counts in AC homes, which the authors concluded was primarily due to closed windows in air‐conditioned homes, which limited entrainment of outdoor spores. 133 They also suggested that decreased indoor RH from air conditioners may have played a minor role in limiting fungal growth in AC homes. Similarly, Lemons et al. (2017) found that fungal species richness was significantly higher in outdoor air compared to AC and EC environments and also reported quantitative PCR findings that fungal spores were three times higher in EC compared to AC homes. 49 The relative differences in fungal abundance between outdoor, AC, and EC homes may be partially explained by AC homes being more closed off to the outdoor environment, and EC homes filtering out a significant portion of ambient fungal spores or fungal cellular components as outdoor air is pulled through wet cooler pads.
However, there is also evidence that fungi and subsequent β‐(1 → 3)‐D‐glucans in EC homes originate in the EC unit itself. Sneller & Pinnas (1987) found that Aspergillus tamarii and Fusarium were recovered from EC but not AC homes, and Aspergillus niger was significantly more common in EC compared with AC homes. 94 Furthermore, they found a more than 100‐fold increase in A. tamarii in EC homes compared to ambient air, and multiple fungal species that were isolated from the evaporative cooler sump water and cooling pads were also found in the home. Lemons et al. (2017) did not find an association between fungal species in indoor air and those swabbed from the EC sump water pans. The authors suggested the evaporative cooling pad may be a likely candidate explaining differences in species found in their air samples; however, cooling pad samples were not included in their study. 49
As with bacterial endotoxin, understanding the influence of ECs on indoor β‐(1 → 3)‐D‐glucan levels is severely limited by the low number of homes for which data are reported in the literature. While there is some evidence that ECs are associated with higher levels and more diverse species of fungi, the study by Johnston et al. (2019) is the only study that we are aware of where β‐(1 → 3)‐D‐glucan levels are reported. Furthermore, studies on associations between ECs and fungi and β‐(1 → 3)‐D‐glucan levels are limited to states in the Western U.S., and therefore may not be gerneralizable to homes in other regions. Maintenance recommendations for EC units focus primarily on measures to prevent buildup of sediment and mineral deposits (scale) in the cooler, which decrease cooler efficiency over time. 3 , 134 , 135 Some scale prevention efforts, such as replacing cooling pads more frequently, may also help reduce the introduction of fungi and fungal components such as β‐(1 → 3)‐D‐glucan into the home. Furthermore, extracts from some fiberous plants such as Luffa gourd (Luffa aegyptiaca and L. cylindrica), show antibacterial and antifungal activity. 136 , 137 In one study, Luffa gourd cooling pads had less mold growth than cooling pads made from date palm stem fibers, Jute tossa, and aspen wood shavings, while maintaining cooling efficiency and low salt deposition. 138 Continued research on pad materials is needed which, in addition to system performance parameters, should consider the potential for fungi and β‐(1 → 3)‐D‐glucan to be introduced into the home. Understanding these factors may help guide the development of updated recommendations that consider health‐related aspects of EC use.
4.4. Evaporative coolers, house dust mites, and their allergens
House dust mite allergen exposure is associated with multiple poor health outcomes, including immune system sensitization, development and exacerbation of asthma, allergic rhinitis, and atopic dermatitis. 60 , 61 , 62 , 63 , 64 , 139 , 140 Der p 1 and Der f 1, which originate from Dermatophagoides pteronyssinus and D. farinae, respectively, are two common dust mite allergens. 141 These allergens, which are derived from enzymes in the mite gut, are expelled in dust mite feces. Inhalation exposure primarily occurs when dust mite feces is suspended in the air. For allergic sensitization and triggering of allergic symptoms to occur, dust mite allergens must be present at clinically significant levels. For allergic sensitization, including the development of asthma, this threshold is 2.0 μg of dust mite allergen per gram of dust. 142 , 143 For development of asthma symptoms in previously sensitized individuals, the threshold is 10.0 μg of dust mite allergen per gram of dust. 144 , 145 , 146
House dust mites primarily feed on skin cells shed from humans and their pets, and they live in approximately the same temperature range as humans. 61 , 147 Thus, water is generally the limiting factor for dust mite growth and reproduction in homes. 148 , 149 , 150 House dust mites primarily acquire water from humid air. 148 , 151 RH levels necessary for the survival of house dust mites range from 55.0% to 75.0% at temperatures between 15.0°C and 35.0°C. 151 , 152 Residential AC systems decrease indoor RH, and thus AC homes tend to have lower levels of house dust mites and their allergens in humid climates. 153 , 154 In dry climates, the lack of humidity appears to prevent dust mite populations from thriving. Several studies report low and clinically insignificant levels of indigenous mites and their allergens in approximately 20%–25% of homes in the Rocky Mountain States in the U.S. 32 , 155 , 156 , 157 However, there is some evidence that increased RH associated with ECs may create an ecological niche for house dust mites in climates where they otherwise would not thrive. Studies conducted in Utah and Colorado (USA) show ECs can increase indoor RH by 10% or more compared to homes with AC or no air conditioning. 32 , 33 In some cases, increased RH from ECs may provide enough water to support house dust mite survival and reproduction.
To date, a few studies show a positive relationship between ECs and the presence of dust mites and their allergens in homes (Table 3). Ellingson et al. (1995), in a study of homes in the Denver, CO (USA) area, found Der p 1 and Der f 1 prevalence and levels in house dust were significantly higher in EC (n = 19) homes compared to homes with no air conditioning (n = 19). 33 In their study, 63% of EC homes were positive for Der p 1 and/or Der f 1, and the mean mite allergen level in EC homes was 11.02 μg per gram of dust. In contrast, 26% of homes with no air conditioning were positive for mite allergens, and the mean allergen level was only 0.19 μg per gram of dust. Nelson & Fernandez‐Caldas (1995) counted dust mites from mattress or bedroom carpet dust collected by 58 patients being treated for bronchial asthma at National Jewish Center for Immunology in Denver, CO. 157 All dust samples were collected from patient homes in the Rocky Mountain region. Of the 58 dust samples submitted, only 10 contained house dust mites. However, the sample with the highest number of mites (3000 mites/g of house dust) was from a home with an evaporative cooler in New Mexico. It should be noted, however, that the other three EC homes in the study did not have any quantifiable dust mites. Vanlaar et al. (2001), in a study of 50 rural homes located in dry, inland Australia, reported that ECs (n = 22) increased Der p 1 levels 3.34 (p = 0.007) and 3.94 (p = 0.003) times in bed and bedroom floor dust samples, respectively. 59 Geometric mean Der p 1 levels in EC homes were 11.29 and 7.54 μg per gram of dust in bed and floor samples, respectively.
TABLE 3.
House dust mite allergen concentrations by type of air conditioning
| Study | Location | Antigen | AC type a | No. homes | Antigen level (μg/g dust) b | Indoor RH(%) c |
|---|---|---|---|---|---|---|
| Ellingson et al. (1995) 33 | Colorado Front Range area (USA) | Der p 1, Der f 1 |
EC No AC |
19 19 |
11.02 0.19 |
59.1 43.1 |
| Vanlaar et al. (2001) 59 | Rural homes in Moree & Wagga Wagga, Australia | Der p 1 |
EC No AC |
22 28 |
11.29 7.54 |
|
| Johnston et al. (2016) 32 | Middle‐income homes in Utah County, Utah (USA) | Der p 1, Der f 1 |
EC AC |
18 22 |
0.108, 0.369 |
49.7 40.1 |
| Tovey et al. (1997) 158 | Homes in Broken Hill (AUS) | Der p 1 |
EC No AC |
50 26 |
0.38 0.47 |
|
| Johnston et al. (2018) 159 | Low‐income homes in Utah County, Utah (USA) | Der p 1, Der f 1 | EC | 22 | 0.125, 0.126 | |
| Johnston et al. (2019) 93 | Low‐income homes in Utah County, Utah (USA) | Der p 1, Der f 1 |
EC AC |
20 28 |
0.21 0.09 |
44.5 43.9 |
EC, Evaporative Air Conditioner; AC, Vapor Compression Air Conditioner; No AC, No air conditioning. In Vanlaar et al. (2001), homes in Moree and Wagga Wagga were predominantly non‐air conditioned, with only a few homes using AC. The authors reported no difference in Der p 1 between AC and no AC homes, so they were combined as No AC homes in the analysis.
In some cases authors only reported combined antigen levels for Der p 1 and Der f 1, so only one value is given per type of AC even though both Der p 1 and Der f 1 were analyzed in the study. Where two values are given, they are for Der p 1 and Der f 1, respectively. For Johnston et al. (2016), there was no difference in mite allergen levels by type of air conditioning, and only combined Der p 1 and Der f 1 levels were reported.
RH levels reported in the table are for summer measurements when air conditioning units are most commonly used.
In contrast, several studies show no relationship between EC use and dust mite allergen levels, or show allergen levels in EC homes below the 2.0 μg per gram of dust threshold for clinical significance (Table 3). Tovey et al. (1997) found no difference in Der p 1 levels in house dust between EC (n = 50) and non‐EC (n = 26) homes in Broken Hill (AUS), which has a hot, arid climate. 158 Furthermore, mite allergen levels in their study were below the 2.0 μg per gram threshold for sensitization. In a study of middle‐income homes of university faculty and staff in Utah (USA), Johnston et al. (2016) found low levels of Der p 1 and Der f 1 in house dust in 25% of study homes, but only one sample was above the 2.0 μg per gram threshold for sensitization. 32 Mean Der p 1 and Der f 1 levels were 0.11 and 0.37 μg per gram of dust, respectively. The authors found no difference in mean Der p 1 and Der f 1 allergen levels between EC (n = 18) and AC (n = 22) homes. In a study of low‐income homes with evaporative coolers (n = 22) in the same county, Johnston et al. (2018) 159 found 68.2% of study homes tested positive for Der p 1 or Der f 1 in house dust. However, allergen levels, with the exception of one sample, were again below the sensitization threshold. In a subsequent study of low‐income homes in Utah County, Utah, Johnston et al. (2019) found Der p 1 or Der f 1 in house dust was significantly higher in EC (n = 20) compared to AC (n = 28) homes (OR = 2.29; 95% CI: 1.05, 4.98; p = 0.04). 93 The authors also found a higher prevalence of dust mite allergens in EC (55%) compared to AC homes (36%). However, allergen levels were again below the 2.0 μg per gram threshold for sensitization for all but two samples. Mean allergen levels in EC and AC homes, across all sample locations, were 0.21 and 0.09 μg per gram of dust, respectively.
Associations between ECs and house dust mites and their allergens are based on relatively small studies from Western U.S. States and dry regions in Australia, and thus may not be generalizable to other locations globally. The available studies also differ in the methods used to collect and process dust samples for analysis. For example, several studies report collecting samples from mattresses, 32 , 33 , 93 , 159 while one study reported collecting samples from bedding on top of the mattress. 59 There were also inconsistencies in the sizes of dust used in Der p 1 and Der f 1 extractions, with some studies prescreening house dust with 300 μm sieves, 32 , 93 one study using 400 μm sieves, 59 and other studies not specifying. 33 , 159 It is unclear how these factors may have influenced study results. Larger studies involving sample collection across multiple geographic regions, using consistent methods, may help resolve the conflicting results from prior studies.
4.5. Evaporative coolers and residential microbial exposures
The human microbiome is defined as the collection of all the microorganisms (bacteria, archaea, eukaryotes, and viruses) living in association with the human body. 160 , 161 These communities that constitute our microbiome can be found throughout the body, including the gastrointestinal tract, skin, oral cavities, mammary glands, placenta, lungs, nasal, and the urogenital tract. 161 Between individuals, the microbiome genetic variation is much greater than the genomic variation (humans share 99.9% of their host genomes, but only 80–90% of their microbiome genomes). 161 , 162 , 163 Urbanization has resulted in people spending the majority of their time indoors, resulting in a larger role for the residential microbiome, mainly dust‐borne microbes, in human microbial exposure. 164 , 165 House dust has been estimated to have 500–1000 different microbial species. 164 , 166 Early life exposure to a diverse microbial environment is essential for the proper development and education of the immune system. 167 This early microbiota exposure first occurs during pregnancy, and at birth, with a strong influence on multiple health outcomes including inflammatory bowel disease, asthma, allergy, cancer, diabetes, metabolic syndrome, and obesity. 69 , 161 The prenatal and early postnatal periods are a critical window of time for exposure to diverse microbes, immune cell development, and disease prevention. 69 Children <4 years of age spend 18 or more hours, and children <1 year spend almost 20 h per day within the home. 112 Thus, the residential environment likely plays a key role in the diversity of microbes a child is exposed to during this critical developmental period for the immune system and the occupants and occupant density are also influencing the residential microbiome. 75 , 76
Westernization has altered urbanization and home architecture, dramatically changing our interaction with the outdoor environment and exposure to microbes. 75 Recent work examining homes across an urbanization gradient in the Amazon rainforest, has identified unique microbial and chemical profiles based on characteristics such as house architecture, construction material, and occupant density. 76 Urbanization is associated with reduced outdoor microbial exposure and increased exposure to antimicrobials, cleaning products, and chemical diversity, resulting in increased exposure to human associated microbes and decreased exposure to environmental microbes. 75 , 76 Thus, urbanization influences home characteristics, the diversity and type of microbial and chemical exposure, and has a significant impact on the inhabitants' human microbiome. 75 , 76 Recent studies characterizing home microbiomes in Finland and Germany identified unique microbiome compositions for farming and non‐farming homes and they found that asthma risk decreased as the similarity of the home bacterial microbiota composition to that of farm homes increased. They concluded that indoor dust microbiota composition appears to be a definable predictor of asthma risk and a target that could be useful for asthma prevention. 90
How ECs may influence home microbiome composition remains unknown, but it is becoming increasingly clear that changes in human microbial diversity, particularly in early developmental periods, has significant influence on many health outcomes. 69 Only a couple of studies have been performed over the years that provide insight into the influence of ECs on home microbiomes (Table 4). Lebowitz et al (1982) identified increased algae and thermophyllic bacillus in homes with evaporative coolers and possible connections between bioaerosols and asthma. 95 Sneller & Pinnas (1987) found more fungi and more diverse species of fungi in EC compared to AC homes in the U.S. southwest. 94 Macher & Girman (1990) identified multiplication of microorganisms in ECs as a potential health concern. 15 In their study of a single home with an EC, bacteria in sump water grew to 1.0 × 10 5 CFU/mL during 9 weeks of operation during summer months. Bacterial and fungal species in indoor air more closely matched species in EC sump water than in outdoor air. Macher et al. (1995) also examined the distribution Micrococcuus luteus in an EC home after artificially contaminating the cooler with the bacteria. 168 They concluded that the transfer rate was low (55 cfu/min), even though the EC was heavily contaminated with the tracer bacteria (>106 CFU/mL).
TABLE 4.
Microbiome of homes with evaporative coolers and central air conditioners
| Study | Methodology | No. homes | Bacterial phyla/species | Fungal species | ||
|---|---|---|---|---|---|---|
| EC | AC | EC | AC | |||
| Lemons et al. (2017) 49 | Next generation sequencing of air samples and swab samples from sump water |
EC 10 AC 11 |
Proteobacteria (55.93%) Actinobacteria (21.63%) Firmicutes (14.43%) |
Proteobacteria (58.38%) Firmicutes (18.73%) Actinobacteria (17.06%) |
Alternaria alternata (32%) and Phoma spp. (22%) | Aspergilius (20%) and Cryptoccocus (20%) |
|
Sneller et al. (1987) 94 |
Petri dish samples placed in the home |
EC 15 AC 8 |
‐ | ‐ | Alternaria, Aspergillus tamarii a , Aspergillus spp, Biospora and Fusarium more abundant | Penicilium spp, Mycelia sterilia, Cephalosporium more abundant |
EC, Evaporative Air Conditioner; AC, Vapor Compression Air Conditioner.
Aspergillus tamarii was more prevalent in EC compared to AC homes, and Penicillium spp were more abundant in AC compared to EC homes (p < 0.05). Fusarium was isolated exclusively from EC homes.
Large‐scale quantitative residential microbiome studies examining the role of ECs have not been performed to date. The largest study thus far, and only next generation sequencing study on this topic to date, was conducted by Lemons et al. (2017), who examined the microbiome of homes (n = 21) in the Great Basin Desert region (USA) and found that EC and AC homes had similar bacterial populations but significant differences in fungal species present (summarized in Table 4). 49 EC homes had significantly higher levels of hydrophilic fungi in air samples compared to AC homes. 49 This study also reported significant diversity in fungal species between EC and non‐EC homes, with EC homes being more likely to harbor species associated with allergic sensitization. The dynamic and regional differences in equipment and water sources make studying their microbiomes at a large scale more difficult.
4.6. Evaporative coolers and Legionella pneumophila
Legionella pneumophila made its debut as a deadly human pathogen in the 1976 outbreak of pneumonia among members of the American Legion attending a conference in Philadelphia (USA). 169 In the four decades following, L. pneumophila has been implicated as the causative agent in a number of outbreaks, often associated with engineered water systems such as cooling towers, building hot water systems, and whirlpool spas. 170 , 171 , 172 , 173 , 174 , 175 ECs have some similarities to industrial cooling towers and thus have the potential to harbor L. pneumophila; however, we found little in the published literature on this topic. Two studies from the Sudan report finding L. pneumophila in residential EC units, however, no cases of Legionnaire's Disease or Pontiac Fever were reported. 176 , 177 As part of a Legionella disease investigation in South Australia, Cameron et al. (1991) collected environmental samples from ECs. They isolated the organism from one out of 21 EC units, again with no reported illnesses. 178 Puckorius et al. (1995) identify two reasons why ECs are low risk for transmitting Legionella. 179 First, Legionella bacteria grow in water at temperatures ranging from 20–45°C, but the optimal temperature range is 37–41°C. ECs operate around the wet bulb temperature, which is generally below 24°C, and often under 20°C. Thus, water temperature in EC units is likely a limiting factor as it ranges closely around the point where the bacteria become dormant. Second, L. pneumophila must be transmitted as a respirable aerosol (<5.0 μm) to reach the alveoli. However, ECs typically release water in the form of vapor (gaseous state) rather than aerosols, and therefore do not transmit the bacteria into the home. In this review, we did not find any reports implicating residential ECs in cases of Legionnaire's Disease or Pontiac Fever, the two primary diseases caused by L. pneumophila.
5. CONCLUSIONS
Residential ECs are a simple, energy‐efficient alternative to vapor compression AC units in arid and semi‐arid climates. The importance of ECs in providing low‐cost comfort to people in hot, dry climates cannot be overstated. Speaking of the advent of mass‐produced ECs in the early 1930's, Cunningham (1985) stated, “In Arizona, man's best friend is not the dog; it is the evaporative cooler”. 2 Almost a century later, ECs remain a boon to people who live in hot dry climates, particularly in resource‐poor settings. However, accompanying the impressive thermal and economic performance of ECs, a growing body of literature suggests that ECs may play important, perhaps even paradoxical, roles in immunological health.
This review brings to light a gap in the literature on ECs, which is the lack of data on health effects associated with their use. Most of the studies identified in this review focus on exposure assessment. These studies are helpful to show differences in bioaerosol levels found in air and dust samples collected from homes, and these data certainly help provide context for future health studies. To date they provide valuable insight on endotoxin and β‐(1 → 3)‐D‐glucan levels, which appear to be higher in homes with ECs. The existing exposure assessement studies also shed light on inconsitencies in relationships between ECs and house dust mites and their allergens, Der p 1 and Der f 1, warranting additional research in this area. Currently, there is little in the published literature on health effects associated with ECs. The fact that no case studies linked EC use to Legionnaire's Disease or Pontic Fever, and only one case study linked EC use to Farmer's lung suggest they are not a significant source of infectious disease transmission. However, epidemiological studies on health effects from ECs are limited. We found only three in this review, two of which used retrospective study designs, 83 , 84 and thus cannot be used to determine the incidence of health outcomes or causality of diseases associated with ECs. 180
Longitudinal, prospective studies, such as the one conducted by Aldous et al. (1996), 82 may be necessary to fully understand the health implications of using ECs. The hygiene hypothesis and current research on the residential microbiome offer an important perspective that may apply to ECs. Namely, ECs may provide important microbial exposures during the critical early‐life window for immune develoment. Although few studies have been done on this topic, data suggest the microbiome of EC homes differs significantly from AC homes, particularly for fungal species. 49 , 94 Furthermore, the largest epidemiological study in this review, conducted by Izadi et al. (2018), showed evidence that ECs may indeed provide some immunological protection, consistent with these theories. 84 This review shows the need for additional research on both deleterious and protective health effects associated with ECs, and many of the most salient questions may best be answered through prospective studies.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare. This research did not include human subjects, and the authors received no external funding for this project.
ACKNOWLEDGMENT
Our special thanks to Jennifer Saldana for her expert work preparing the figures.
Johnston JD, Cowger AE, Weber KS. Bioaerosol and microbial exposures from residential evaporative coolers and their potential health outcomes: A review. Indoor Air. 2022;32:e13082. doi: 10.1111/ina.13082
DATA AVAILABILITY STATEMENT
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
REFERENCES
- 1. Nabokov P, Easton R. Native American Architecture. Oxford University Press; 1989. [Google Scholar]
- 2. Cunningham B. The box that broke the barrier: the swamp cooler comes to southern Arizona. J Arizona History. 1985;26:163‐174. [Google Scholar]
- 3. Watt JR, Brown WK. Evaporative Air Conditioning Handbook. 3rd ed. Fairmont Press; Distributed by Prentice Hall PTR: Lilburn, GA; Upper Saddle River, NJ; 1997. [Google Scholar]
- 4. Speid MJB. Our Last Years in India. Smith, Elder and co; 1862. [Google Scholar]
- 5. Bahadori MN. Passive cooling Systems in Iranian Architecture. Sci Am. 1978;238:144. [Google Scholar]
- 6. Jomehzadeh F, Nejat P, Calautit JK, et al. A review on windcatcher for passive cooling and natural ventilation in buildings, part 1: indoor air quality and thermal comfort assessment. Renew Sust Energ Rev. 2017;70:736‐756. [Google Scholar]
- 7. Abbott SHL. Some remarks on malaria prophylaxis. Ind Med Gaz. 1905;40:173‐174. [PMC free article] [PubMed] [Google Scholar]
- 8. Bom G. Evaporative Air‐Conditioning: Applications for Environmentally Friendly Cooling. Vol 23. World Bank Publications; 1999. [Google Scholar]
- 9. Mast B, McCormick J, Ignelzi P, et al. Evaporative cooling in California: Assessing the market and establishing baselines for evaporative cooling technologies in the residential and commercial/industrial sectors. IEPEC Proc. 1999:353‐364. [Google Scholar]
- 10. Malli A, Seyf HR, Layeghi M, Sharifian S, Behravesh H. Investigating the performance of cellulosic evaporative cooling pads. Energ Convers Manage. 2011;52:2598‐2603. [Google Scholar]
- 11. Nada SA, Fouda A, Mahmoud MA, Elattar HF. Experimental investigation of energy and exergy performance of a direct evaporative cooler using a new pad type. Energ Buildings. 2019;203:109449. [Google Scholar]
- 12. Chiesa G, Pearlmutter D. Ventilative Cooling in Combination with Other Natural Cooling Solutions: Direct Evaporative Cooling—DEC. In: Chiesa G, Kolokotroni M, Heiselberg P, eds. Innovations in Ventilative Cooling. PoliTO Springer Series. Spinger Cham. 2021:167‐190. [Google Scholar]
- 13. Mathews E, Kleingeld M, Grobler L. Integrated simulation of buildings and evaporative cooling systems. Build Environ. 1994;29:197‐206. [Google Scholar]
- 14. Xuan YM, Xiao F, Niu XF, Huang X, Wang SW. Research and applications of evaporative cooling in China: a review (II)‐systems and equipment. Renew Sust Energ Rev. 2012;16:3523‐3534. [Google Scholar]
- 15. Macher J, Girman J. Multiplication of microorganisms in evaporative air cooler and possible indoor air contamination. Environ Int. 1990;16:203‐211. [Google Scholar]
- 16. Paschold H, Li WW, Morales H, Walton J. Laboratory study of the impact of evaporative coolers on indoor PM concentrations. Atmos Environ. 2003;37:1075‐1086. [Google Scholar]
- 17. Kinney L. Evaporative cooling policy and program options: promising peak shaving in a growing southwest. U.S. Department of Energy. 2004.
- 18. Davis Energy Group, Energy Solutions . Codes and Standards Enhancement Initiative for PY2004: Title 20 Standards Development. Analysis of Standards Options for Evaporative Coolers ; 2004. Available from: https://citeseerx.ist.psu.edu/viewdoc/download?coi=10.1.1.543.9365&rep=rep1&type=pdf. Last accessed July 23, 2022.
- 19. Wilkenfeld G. A National Demand Management Strategy for Small Air Conditioners: The Role of the National Applicance and Equipment Energy Efficiency Efficiency Program (NAEEEP) ; 2004. Available from: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.456.82&rep=rep1&type=pdf. Last accessed July 23, 2022.
- 20. U.S. Energy Information Administration . Air Conditioning and Other Appliances Increase Residential Electricity Use in the Summer . Available from: https://energycentral.com/c/ec/air‐conditioning‐and‐other‐appliances‐increase‐residential‐electricity‐use‐summer. Last accessed July 23, 2022.
- 21. U.S. Energy Information Administration . Residential Energy Consumption Survey (RECS). Table HC7.1 Air Conditioning in U.S. Homes by Housing Unit Type, 2015. Available from: https://www.eia.gov/consumption/residential/data/2015/hc/php/hc7.1.php. Last accessed July 23, 2022.
- 22. Rahar S, Swami G, Nagpal N, Nagpal MA, Singh GS. Preparation, characterization, and biological properties of β‐glucans. J Adv Pharm Technol Res. 2011;2:94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Arora CP. Refrigeration and air conditioning. Tata McGraw‐Hill Education; 2000. [Google Scholar]
- 24. Whitman B, Johnson B, Tomczyk J, Silberstein E. Refrigeration and air conditioning technology. Cengage Learning; 2012. [Google Scholar]
- 25. Yamamoto N, Shendell D, Winer A, Zhang J. Residential air exchange rates in three major US metropolitan areas: results from the relationship among indoor, outdoor, and personal air study 1999–2001. Indoor Air. 2010;20:85‐90. [DOI] [PubMed] [Google Scholar]
- 26. Nazmara S, Sorooshian A, Delikhoon M, et al. Characteristics and health risk assessment of polycyclic aromatic hydrocarbons associated with dust in household evaporative coolers. Environ Pollut. 2020;256:113379. [DOI] [PubMed] [Google Scholar]
- 27. Raysoni AU, Stock TH, Sarnat JA, et al. Characterization of traffic‐related air pollutant metrics at four schools in El Paso, Texas, USA: implications for exposure assessment and siting schools in urban areas. Atmos Environ. 2013;80:140‐151. [Google Scholar]
- 28. Al‐Farayedhi AA, Ibrahim NI, Gandhidasan P. Condensate as a water source from vapor compression systems in hot and humid regions. Desalination. 2014;349:60‐67. [Google Scholar]
- 29. Mahvi AH, Alipour V, Rezaei L. Atmospheric moisture condensation to water recovery by home air conditioners. Am J Appl Sci. 2013;10:917. [Google Scholar]
- 30. Gereda J, Kinnert M, Price M, Leung D, Liu A. Metropolitan home living conditions associated with indoor endotoxin levels. J Allergy Clin Immunol. 2001;107:790‐796. [DOI] [PubMed] [Google Scholar]
- 31. Mazique D, Diette GB, Breysse PN, et al. Predictors of airborne endotoxin concentrations in inner city homes. Environ Res. 2011;111:614‐617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Johnston JD, Tuttle SC, Nelson MC, et al. Evaporative cooler use influences temporal indoor relative humidity but not dust mite allergen levels in homes in a semi‐arid climate. PLoS One. 2016;11:e0147105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Ellingson A, LeDoux R, Vedanthan P, Weber R. The prevalence of Dermatophagoides mite allergen in Colorado homes utilizing central evaporative coolers. J Allergy Clin Immunol. 1995;96:473‐479. [DOI] [PubMed] [Google Scholar]
- 34. Cuce PM, Riffat S. A state of the art review of evaporative cooling systems for building applications. Renew Sust Energ Rev. 2016;54:1240‐1249. [Google Scholar]
- 35. Isaac M, van Vuuren DP. Modeling global residential sector energy demand for heating and air conditioning in the context of climate change. Energ Policy. 2009;37:507‐521. [Google Scholar]
- 36. Amer O, Boukhanouf R, Ibrahim H. A review of evaporative cooling technologies. Int J Environ Sci Dev. 2015;6:111. [Google Scholar]
- 37. Schroeder C, Zaragoza B, Little J, Gilroy J. Cooling Off While Utilities Heat Up in the Rockies. 2004 Summer study on energy efficiency in buildings: Breaking out of the box. Vol 2004. American Council for an Energy‐Efficient Economy; 2004:1‐9. [Google Scholar]
- 38. Gerritsen R, Zeng B & O'Leary R. A Review of the Alice Solar City Program. Central Australia Research Group, Charles Darwin University, Alice Springs. 2012.
- 39. Utilities, R.P . Energy rebates, residential air conditioning rebate program. 2022. [cited 2022 1‐1‐2022] Available from: https://www.riversideca.gov/utilities/residents/rebates‐energy.asp
- 40. Energy, I.I.D . Residential rebates. 2022. [cited 2022 1‐1‐2022] Available from: https://www.iid.com/customer‐service/save‐energy‐and‐money/your‐home/residential‐rebates
- 41. Electric, E.P . Texas low income residential program for evaporative cooler. 2019. [cited 2022 1‐1‐2022] Available from: https://www.epelectric.com/company/news/texas‐low‐income‐residential‐program‐for‐evaporative‐cooler
- 42. Li WW, Paschold H, Morales H, Chianelli J. Correlations between short‐term indoor and outdoor PM concentrations at residences with evaporative coolers. Atmos Environ. 2003;37:2691‐2703. [Google Scholar]
- 43. Quackenboss JJ, Lebowitz MD, Crutchfield CD. Indoor‐outdoor relationships for particulate matter: exposure classifications and health effects. Environ Int. 1989;15:353‐360. [Google Scholar]
- 44. Paschold H, Li W‐W, Morales H, Pingitore NE, Maciejewska B. Elemental analysis of airborne particulate matter and cooling water in West Texas residences. Atmos Environ. 2003;37:2681‐2690. [Google Scholar]
- 45. Thompson CR, Hensel EG, Kats G. Outdoor‐indoor levels of six air pollutants. J Air Pollut Control Assoc. 1973;23:881‐886. [DOI] [PubMed] [Google Scholar]
- 46. Kim KH, Kabir E, Jahan SA. Airborne bioaerosols and their impact on human health. J Environ Sci. 2018;67:23‐35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Georgakopoulos DG, Despres V, Frohlich‐Nowoisky J, et al. Microbiology and atmospheric processes: biological, physical and chemical characterization of aerosol particles. Biogeosciences. 2009;6:721‐737. [Google Scholar]
- 48. Pope CA, Dockery DW. Health effects of fine particulate air pollution: lines that connect. J Air Waste Manage Assoc. 2006;56:709‐742. [DOI] [PubMed] [Google Scholar]
- 49. Lemons AR, Hogan MB, Gault RA, et al. Microbial rRNA sequencing analysis of evaporative cooler indoor environments located in the Great Basin desert region of the United States. Environ Sci: Processes Impacts. 2017;19:101‐110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Rylander R. Investigations of the relationship between disease and airborne (1 ‐> 3)‐beta‐D‐glucan in buildings. Mediat Inflamm. 1997;6:275‐277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Rylander R, Norrhall M, Engdahl U, Tunsater A, Holt PG. Airways inflammation, atopy, and (1 ‐> 3)‐beta‐D‐glucan exposures in two schools. Am J Resp Crit Care. 1998;158:1685‐1687. [DOI] [PubMed] [Google Scholar]
- 52. Thorn J, Rylander R. Airways inflammation and glucan in a rowhouse area. Am J Respir Crit Care Med. 1998;157:1798‐1803. [DOI] [PubMed] [Google Scholar]
- 53. Thorn J, Beijer L, Rylander R. Airways inflammation and glucan exposure among household waste collectors. Am J Ind Med. 1998;33:463‐470. [DOI] [PubMed] [Google Scholar]
- 54. Douwes J, Zuidhof A, Doekes G, et al. (1‐‐>3)‐beta‐D‐glucan and endotoxin in house dust and peak flow variability in children. Am J Respir Crit Care Med. 2000;162:1348‐1354. [DOI] [PubMed] [Google Scholar]
- 55. Thorne PS, Kulhankova K Yin M, et al. Endotoxin exposure is a risk factor for asthma: the national survey of endotoxin in United States housing. Am J Respir Crit Care Med. 2005;172:1371‐1377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Michel O, Kips J, Duchateau J, et al. Severity of asthma is related to endotoxin in house dust. Am J Respir Crit Care Med. 1996;156:1641‐1646. [DOI] [PubMed] [Google Scholar]
- 57. Michel O, Ginanni R, Duchateau J, Vertongen F, Le Bon B, Sergysels R. Domestic endotoxin exposure and clinical severity of asthma. Clin Exp Allergy. 1991;21:441‐448. [DOI] [PubMed] [Google Scholar]
- 58. Oluwole O, Rennie DC, Senthilselvan A, et al. The association between endotoxin and beta‐(1→3)‐D‐glucan in house dust with asthma severity among schoolchildren. Respir Med. 2017; 138:38‐46. [DOI] [PubMed] [Google Scholar]
- 59. Vanlaar CH, Downs SH, Mitakakis TZ, et al. Predictors of house‐dust‐mite allergen concentrations in dry regions in Australia. Allergy. 2001;56:1211‐1215. [DOI] [PubMed] [Google Scholar]
- 60. Sporik R, Holgate ST, Plattsmills TAE, Cogswell JJ. Exposure to house‐dust mite allergen (Der‐P‐I) and the development of asthma in childhood ‐ a prospective‐study. New Engl J Med. 1990;323:502‐507. [DOI] [PubMed] [Google Scholar]
- 61. Portnoy J, Miller JD, Williams PB, et al. Environmental assessment and exposure control of dust mites: a practice parameter. Ann Allerg Asthma Immunol. 2013;111:465‐507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Lodge CJ, Lowe AJ, Gurrin LC, et al. House dust mite sensitization in toddlers predicts current wheeze at age 12 years. J Allergy Clin Immunol. 2011;128:782‐788. [DOI] [PubMed] [Google Scholar]
- 63. Tunnicliffe WS, Fletcher TJ, Hammond K, et al. Sensitivity and exposure to indoor allergens in adults with differing asthma severity. Eur Respir J. 1999;13:654‐659. [DOI] [PubMed] [Google Scholar]
- 64. Teplitsky V, Mumcuoglu KY, Babai I, Dalal I, Cohen R, Tanay A. House dust mites on skin, clothes, and bedding of atopic dermatitis patients. Int J Dermatol. 2008;47:790‐795. [DOI] [PubMed] [Google Scholar]
- 65. Yang YF, Cui G, Lan CQ. Developments in evaporative cooling and enhanced evaporative cooling ‐ a review. Renew Sust Energ Rev. 2019;113:109230. [Google Scholar]
- 66. Liu A. Something old, something new: indoor air endotoxin, allergens and asthma. Pediatr Respir Rev. 2004;5:S65‐S71. [DOI] [PubMed] [Google Scholar]
- 67. Liu A. Revisiting the hygien hypotheiss for allergy and asthma. J Allergy Clin Immunol. 2015;136:860‐865. [DOI] [PubMed] [Google Scholar]
- 68. Ege MJ. The hygiene hypothesis in the age of the microbiome. Ann Am Thorac Soc. 2017;14:S348‐S353. [DOI] [PubMed] [Google Scholar]
- 69. Renz H, Skevaki C. Early life microbial exposures and allergy risks: opportunities for prevention. Nat Rev Immunol. 2021;21:177‐191. [DOI] [PubMed] [Google Scholar]
- 70. Ege MJ et al. Exposure to environmental microorganisms and childhood asthma. N Engl J Med. 2011;364:701‐709. [DOI] [PubMed] [Google Scholar]
- 71. Ruokolainen L, Paalanen L, Karkman A, et al. Significant disparities in allergy prevalence and microbiota between the young people in Finnish and Russian Karelia. Clin Exp Allergy. 2017;47:665‐674. [DOI] [PubMed] [Google Scholar]
- 72. Pfefferle PI, Keber CU, Cohen RM, Garn H. The hygiene hypothesis–learning from but not living in the past. Front Immunol. 2021;12:632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Stiemsma LT, Reynolds LA, Turvey SE, Finlay BB. The hygiene hypothesis: current perspectives and future therapies. ImmunoTargets Ther. 2015;4:143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Bloomfield SF, Rook GAW, Scott EA, Shanahan F, Stanwell‐Smith R, Turner P. Time to abandon the hygiene hypothesis: new perspectives on allergic disease, the human microbiome, infectious disease prevention and the role of targeted hygiene. Perspect Public Health. 2016;136:213‐224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Ruiz‐Calderon JF, Cavallin H, Song SJ, et al. Walls talk: microbial biogeography of homes spanning urbanization. Sci Adv. 2016;2:e1501061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. McCall LI, Callewaert C, Zhu Q, et al. Home chemical and microbial transitions across urbanization. Nat Microbiol. 2020;5:108‐115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Adams K, Weber KS, Johnson SM. Exposome and immunity training: how pathogen exposure order influences innate immune cell lineage commitment and function. Int J Mol Sci. 2020;21:8462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Marinkovich VA, Hill A. Hypersensitivity Alveolitis. JAMA. 1975;231:944‐947. [PubMed] [Google Scholar]
- 79. Kotimaa MH, Husman KH, Terho EO, Mustonen MH. Airborne molds and actinomycetes in the work environment of farmer's lung patients in Finland. Scand J Work Environ Health. 1984;10:115‐119. [DOI] [PubMed] [Google Scholar]
- 80. Reyes CN, Wenzel FJ, Lawton BR, Emanuel DA. The pulmonary pathology of farmer's lung disease. Chest. 1982;81:142‐146. [DOI] [PubMed] [Google Scholar]
- 81. Al‐Zubaidy TS. Effects of aircoolers on city dwellers. Indoor Air '87: Proceedings of the 4th International Conference on Indoor Air Quality and Climate; Berlin (West); 1987. p. 17–21.
- 82. Aldous MB, Holberg CJ, Wright AL, Martinez FD, Taussig LM. Evaporative cooling and other home factors and lower respiratory tract illness during the first year of life. Group health medical associates. Am J Epidemiol. 1996;143:423‐430. [DOI] [PubMed] [Google Scholar]
- 83. Prasad C, Hogan MB, Peele K, Wilson NW. Effect of evaporative coolers on skin test reactivity to dust mites and molds in a desert environment. Allergy Asthma Proc. 2009;30:624‐627. [DOI] [PubMed] [Google Scholar]
- 84. Izadi N, Brar K, Lanser B. Evaporative coolers are not associated with dust mite or mold sensitization in a large pediatric cohort. Ann Allergy Asthma Immunol. 2018;120:542‐543. [DOI] [PubMed] [Google Scholar]
- 85. Stein MM, Hrusch CL, Gozdz J, et al. Innate immunity and asthma risk in Amish and Hutterite farm children. N Engl J Med. 2016;375:411‐421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Ihrke D. Households on the move. United States Census Bureau; 2013. [Google Scholar]
- 87. Simon AK, Hollander GA, McMichael A. Evolution of the immune system in humans from infancy to old age. Proc R Soc B Biol Sci. 2015;282:20143085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Gensollen T, Blumberg RS. Correlation between early life regulation of immune system by microbiota and allergy development. J Allergy Clin Immunol. 2017;139:1084‐1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Bach J‐F. The effect of infections on susceptibility to autoimmune and allergic diseases. New Engl J Med. 2002;347:911‐920. [DOI] [PubMed] [Google Scholar]
- 90. Kirjavainen PV, Karvonen AM, Adams RI, et al. Farm‐like indoor microbiota in non‐farm homes protects children from asthma development. Nat Med. 2019;25:1089‐1095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Von Hertzen L, Hanski I, Haahtela T. Natural immunity: biodiversity loss and inflammatory diseases are two global megatrends that might be related. EMBO Rep. 2011;12:1089‐1093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Johnston JD, Kruman BA, Nelson MC, et al. Differential effects of air conditioning type on residential endotoxin levels in a semi‐arid climate. Indoor Air. 2017;27:946‐954. [DOI] [PubMed] [Google Scholar]
- 93. Johnston JD, Cowger AE, Graul RJ, et al. Associations between evaporative cooling and dust‐mite allergens, endotoxins, and β‐(1→ 3)‐d‐glucans in house dust: a study of low‐income homes. Indoor Air. 2019;29:1005‐1017. [DOI] [PubMed] [Google Scholar]
- 94. Sneller M, Pinnas J. Comparison of airborne fungi in evaporative cooled and air conditioned homes. Ann Allergy. 1987;59:317‐320. [PubMed] [Google Scholar]
- 95. Lebowitz MD, O'Rourke MK, Dodge R, et al. The adverse health effects of biological aerosols, other aerosols, and indoor microclimate on asthmatics and nonasthmatics. Environ Int. 1982;8:375‐380. [Google Scholar]
- 96. Werner M, Topp R, Wimmer K, et al. TLR4 gene variants modify endotoxin effects on asthma. J Allergy Clin Immunol. 2003;112:323‐330. [DOI] [PubMed] [Google Scholar]
- 97. Muroi M, Tanamoto K‐I. The polysaccharide portion plays an indispensable role in salmonella lipopolysaccharide‐induced activation of NF‐kappaB through human toll‐like receptor 4. Infect Immun. 2002;70:6043‐6047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Elson G, Dunn‐Siergrist R, Daubeuf B, Pugin J. Contribution of toll‐like receptors to the innate immune response to gram‐negative and gram‐positive bacteria. Blood. 2007;109:1574‐1583. [DOI] [PubMed] [Google Scholar]
- 99. Beutler B. TLR4 as the mammalian endotoxin sensor. In: Curr Top Microbiol Immunol. 2002;270:109‐120. [DOI] [PubMed] [Google Scholar]
- 100. Park BS, Lee J‐O. Recognition of lipopolysaccharide pattern by TLR4 complexes. Exp Mol Med. 2013;45:e66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Arbour NC, Lorenz E, Schutte BC, et al. TLR4 mutations are associated with endotoxin hyporesponsiveness in humans. Nat Genet. 2000;25:187‐191. [DOI] [PubMed] [Google Scholar]
- 102. Braun‐Fahrlander C, Riedler J, Herz U, et al. Environmental exposure to endotoxin and its relation to asthma in school‐age children. New Engl J Med. 2002;347:869‐877. [DOI] [PubMed] [Google Scholar]
- 103. Holst G, Host A, Doekes G, Meyer HW, Madsen AM, Sigsgaard T. Determinants of house dust, endotoxin, and β‐(1→ 3)‐d‐glucan in homes of Danish children. Indoor Air. 2015;25:245‐259. [DOI] [PubMed] [Google Scholar]
- 104. Giovannangelo M, Gehring U, Nordling E, et al. Determinants of house dust endotoxin in three European countries‐the AIRALLERG study. Indoor Air. 2007;17:70‐79. [DOI] [PubMed] [Google Scholar]
- 105. Thorne P, Cohn R, Mav D, Arbes S Jr, Zeldin D. Predictors of endotoxin levels in U.S. housing. Environ Health Perpect. 2009;117:763‐771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Bischof W, Koch A, Gehring U, Fahlbusch B, Wichmann HE, Heinrich J. Predictors of high endotoxin concentrations in the settled dust of German homes. Indoor Air. 2002;12:2‐9. [DOI] [PubMed] [Google Scholar]
- 107. Schram D, Doekes G, Boeve M, et al. Bacterial and fungal components in house dust of farm children, Rudolf Steiner school children and reference children–the PARSIFAL study. Allergy. 2005;60:611‐618. [DOI] [PubMed] [Google Scholar]
- 108. Gehring U, Bischof W, Borte M, Herbarth O, Wichmann HE, Heinrich J. Levels and predictors of endotoxin in mattress dust samples from east and west German homes. Indoor Air. 2004;14:284‐292. [DOI] [PubMed] [Google Scholar]
- 109. Wickens K, Douwes J, Siebers R, et al. Derterminants of endotoxin levels in carpets in New Zealand homes. Indoor Air. 2003;12:128‐135. [DOI] [PubMed] [Google Scholar]
- 110. Chen CM, Thiering E, Doekes G, et al. Geographical variation and the determinants of domestic endotoxin levels in mattress dust in Europe. Indoor Air. 2012;22:24‐32. [DOI] [PubMed] [Google Scholar]
- 111. Casas L, Tischer C, Wouters IM, et al. Endotoxin, extracellular polysaccharides, and β (1‐3)‐glucan concentrations in dust and their determinants in four European birth cohorts: results from the HITEA project. Indoor Air. 2013;23:208‐218. [DOI] [PubMed] [Google Scholar]
- 112. Cohen Hubal EA, Sheldon LS, Burke JM, et al. Children's exposure assessment: a review of factors influencing Children's exposure, and the data available to characterize and assess that exposure. Environ Health Perspect. 2000;108:475‐486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Zhang K, Petty HR. Influence of polysaccharides on neutrophil function: specific antagonists suggest a model for cooperative saccharide‐associated inhibition of immune complex‐triggered superoxide production. J Cell Biochem. 1994;56:225‐235. [DOI] [PubMed] [Google Scholar]
- 114. Adachi Y, Okazaki M, Ohno N, Yadomae T. Enhancement of cytokine production by macrophages stimulated with (1→3)‐β‐D‐glucan, grifolan (GRN), isolated from Grifola frondosa. Biological and Pharmaceutical Bulletin. 1994;17:1554‐1560. [DOI] [PubMed] [Google Scholar]
- 115. Lebron F, Vasallo R, Puri V, Limpers A. Pneumocystis Carinii cell wall ß‐glucans initiate macrophage inflammatory responses through NF‐kB activation. J Biol Chem. 2003;278:25001‐25008. [DOI] [PubMed] [Google Scholar]
- 116. Saito K, Nishijima M, Ohno N, Nagi N, Yadomae T, Miyazaki T. Activation of compliment and limulus coagulation system by an alkali‐soluble glucan isolated from Omphalia lapidescens and its less branched derivates. Chem Pharm Bull. 1992;40:1227‐1230. [DOI] [PubMed] [Google Scholar]
- 117. Mahauthaman R, Howell CJ, Spur BW, et al. The generation and cellular distribution of leukotriene C4 in human eosinophils stimulated by unopsonized zymosan and glucan particles. Clin Immunol. 1988;81:696‐705. [DOI] [PubMed] [Google Scholar]
- 118. Kerékgyártó C, Virág L, Tankó L, Chihara G, Fachet J. Strain differences in the cytotoxic activity of TNF production of murine macrophages stimulated by lentinan. Int J Immunopharmacol. 1996;18:347‐353. [DOI] [PubMed] [Google Scholar]
- 119. Chan W, Law H, Lin Z, Lau Y, Chan G. Response of human dendritic cells to different immunomodulatory polysaccharides derived from mushroom and barley. Int Immunol. 2007;19:891‐899. [DOI] [PubMed] [Google Scholar]
- 120. Harada K, Itashiki Y, Takenawa T, Ueyama Y. Effects of lentinan alone and in combination with fluoropyrimidine anticancer agent on growth of human oral squamous cell carcinoma in vitro and in vivo. Int J Oncol. 2010;37:623‐631. [DOI] [PubMed] [Google Scholar]
- 121. Reponen T, Vesper S, Levin L, et al. High environmental relative moldiness index during infancy as a predictor of asthma at 7 years of age. Ann Allergy Asthma Immunol. 2011;107:120‐126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Hadebe S, Kirstein F, Fierens K, et al. Beta‐Glucan exacerbates allergic airway responses to house dust mite allergen. Respir Res. 2016;17:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Black PN, Udy AA, Brodie SM. Sensitivity to fungal allergens is a risk factor for life‐threatening asthma. Allergy. 2000;55:501‐504. [DOI] [PubMed] [Google Scholar]
- 124. Zureik M, Neukirch C, Leynaert B, Liard R, Liard J, Neukirch F. Sensitisation to airborne moulds and severity of asthma: cross sectional study from European Community respiratory health survey. BMJ. 2002;235:411‐414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Rylander R, Fogelmark B, Ewaldsson B. Moldy environments and toxic pneumonitis. Toxicol Ind Health. 2008;24:177‐180. [DOI] [PubMed] [Google Scholar]
- 126. Burg AR, Quigley L, Jones AV, et al. Orally administered β‐glucan attenuates the Th2 response in a model of airway hypersensitivity. Springer Plus. 2016;5:815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Kirmaz C, Bayrak P, Yilmaz O, Yuksel H. Effects of glucan treatment on the Th1/Th2 balance in patients with allergic rhinitis: a double‐blind placebo‐controlled study. Eur Cytokine Netw. 2005;16:128‐134. [PubMed] [Google Scholar]
- 128. Sarinho E, Medeiros D, Schor D, et al. Production of interleukin‐10 in asthmatic children after beta‐1‐3‐glucan. Allergol Immunopathol. 2009;37:188‐192. [DOI] [PubMed] [Google Scholar]
- 129. Zhang Z, Myers JMB, Brandt EB, et al. β‐Glucan exacerbates allergic asthma independent of fungal sensitization and promotes steroid‐resistant TH2/TH17 responses. J Allergy Clin Immunol. 2017;139:54‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Hadebe S, Kirstein F, Fierens K, et al. β‐Glucan exacerbates allergic airway responses to house dust mite allergen. Respir Res. 2016;17:1‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131. Winer HL. The mucosal milieu creates tolerogenic dendritic cells and TR1 and TH3 regulatory cells. Nat Immunol. 2001;2:671‐672. [DOI] [PubMed] [Google Scholar]
- 132. Aliberti J. Immunity and tolerance induced by intestinal mucosal dendritic cells. Mediat Inflamm. 2016;2016:3104727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Hirsch D, Hirsch S, Kalbfleisch J. Effect of central air conditioning and meteorologic factors on indoor spore counts. J Allergy Clin Immunol. 1978;62:22‐26. [DOI] [PubMed] [Google Scholar]
- 134. Bahobail MA. Evaporative cooler: self salt clean. J King Saud Univ. 2013;25:1‐12. [Google Scholar]
- 135. Qureshi BA, Zubair SM. The impact of fouling on performance evaluation of evaporative coolers and condensers. Int J Energy Res. 2005;29:1313‐1330. [Google Scholar]
- 136. Al‐Snafi AE. Constituents and pharmacology of Luffa cylindrica‐a review. IOSR J Pharm. 2019;9:68‐79. [Google Scholar]
- 137. Mankilik M, Mikailu A, Mhya D. Phytochemical content and antimicrobial activities of Luffa aegyptiaca (sponge gourd) leaves extracts. Int J Res Pharm Biosci. 2014;1:1‐4. [Google Scholar]
- 138. Al‐Sulaiman F. Evaluation of the performance of local fibers in evaporative cooling. Energ Convers Manage. 2002;43:2267‐2273. [Google Scholar]
- 139. Sears M, Herbison GP, Holdaway MD, Hewitt CJ, Flannery EM, Silva PA. The relative risks of sensitivity to grass pollen, house dust mite and cat dander in the development of childhood asthma. Clin Exp Allergy. 1989;19:419‐424. [DOI] [PubMed] [Google Scholar]
- 140. Miller JD. The role of dust mites in allergy. Clin Rev Allergy Immunol. 2018;57:312‐329. [DOI] [PubMed] [Google Scholar]
- 141. Baxi SN, Phipatanakul W. The role of allergen exposure and avoidance in asthma. Adolesc Med State Art Rev. 2010;21:57. [PMC free article] [PubMed] [Google Scholar]
- 142. Kuehr J, Frischer T, Meinert R, et al. Mite allergen exposure is a risk for the incidence of specific sensitization. J Allergy Clin Immunol. 1994;94:44‐52. [DOI] [PubMed] [Google Scholar]
- 143. Wickman M, Korsgaard J. Transient sensitization to house‐dust mites: a study on the influence of mite exposure and six. European Journal of Allergy and Clinical Immunology. 1996;51:511‐513. [DOI] [PubMed] [Google Scholar]
- 144. Sporik R, Platts‐Mills T, Cogswell J. Exposure to house dust mite allergen of children admitted to hospital with asthma. Clin Exp Allergy. 1993;23:740‐746. [DOI] [PubMed] [Google Scholar]
- 145. Nitschke M, Pilotto LS, Attewell RG, et al. A cohort study of indoor nitrogen dioxide and house dust mite exposure in asthmatic children. J Occup Environ Med. 2006;48:462‐469. [DOI] [PubMed] [Google Scholar]
- 146. Vervloet D, Pradal M, Porri F, Charpin D. The epidemiology of allergy to house dust mites. Rev Mal Respir. 1991;8:59‐65. [PubMed] [Google Scholar]
- 147. Platts‐Mills TAE, de Weck AL, Aalberse RC, et al. Dust mite allergens and asthma—a worldwide problem. J Allergy Clin Immunol. 1989;83:416‐427. [DOI] [PubMed] [Google Scholar]
- 148. Arlian L. Water balance and humidity requirements of house dust mites. Exp Appl Acarol. 1992;16:15‐35. [DOI] [PubMed] [Google Scholar]
- 149. Arlian LG, Confer PD, Rapp CM, Vyszenski‐Moher DL, Chang JC. Population dynamics of the house dust mites Dermatophagoides farinae, D. pteronyssinus, and Euroglyphus maynei (Acari: Pyroglyphidae) at specific relative humidities. J Med Entomol. 1998;35:46‐53. [DOI] [PubMed] [Google Scholar]
- 150. Arlian LG, Morgan MS, Neal JS. Dust mite allergens: Ecology and distribution. Curr Allergy Asthma Rep. 2002;2:401‐411. [DOI] [PubMed] [Google Scholar]
- 151. Arlian LG, Platts‐Mills TAE. The biology of dust mites and the remediation of mite allergens in allergic disease. J Allergy Clin Immunol. 2001;107:406‐413. [DOI] [PubMed] [Google Scholar]
- 152. Arlian LG, Veselic MM. Reevaluation of the humidity requirements of the house dust mite Dermatophagoides farinae . J Med Entomol. 1981;18:351‐352. [Google Scholar]
- 153. Lintner TJ, Brame KA. The effects of season, climate, and air‐conditioning on the prevalence of Dermatophagoides mite allergens in household dust. J Allergy Clin Immunol. 1993;91:862‐867. [DOI] [PubMed] [Google Scholar]
- 154. Carpenter GB, Win GH, Furumizo RT, Massey DG, Ortiz AA. Air conditioning and house dust mite. J Allergy Clin Immunol. 1985;75:121. [Google Scholar]
- 155. Weiler E, Semmens E, Noonan C, Cady C, Ward T. Dust allergens within rural northern rocky mountain residences. Jacobs J Allergy Immunol. 2015;1:1‐6. [PMC free article] [PubMed] [Google Scholar]
- 156. Moyer D, Nelson H, Arlian L. House dust mites in Colorado. Ann Allergy. 1985;55:680‐682. [PubMed] [Google Scholar]
- 157. Nelson HS, Fernandez‐Caldas E. Prevalence of house dust mites in the Rocky Mountain states. Ann Allergy Asthma Immunol. 1995;75:337‐339. [PubMed] [Google Scholar]
- 158. Tovey E, Mamic A, Jalaludin B, Beloossova E, Peat J. The use of air conditioning does not have a detectable effect on mite allergen levels in Australian houses. J Allergy Clin Immunol. 1997;99:163. [Google Scholar]
- 159. Johnston JD, Barney TP, Crandall JH, et al. Prevalence of house dust mite allergens in low‐income homes with evaporative coolers in a semiarid climate. Arch Environ Occup Health. 2018;73:38‐41. [DOI] [PubMed] [Google Scholar]
- 160. Marchesi JR, Ravel J. The vocabulary of microbiome research: A proposal. Microbiome. 2015;3:1‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161. Jain T, Sharma P, Are AC, Vickers SM, Dudeja V. New insights into the cancer‐microbiome‐immune Axis: Decrypting a decade of discoveries. Front Immunol. 2021;12:622064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162. Fierer N, Hamady M, Lauber CL, Knight R. The influence of sex, handedness, and washing on the diversity of hand surface bacteria. Proc Natl Acad Sci USA. 2008;105:17994‐17999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163. Turnbaugh PJ, Hamady M, Yatsunenko T, et al. A core gut microbiome in obese and lean twins. Nature. 2009;457:480‐484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164. Shan Y, Guo J, Fan W, et al. Modern urbanization has reshaped the bacterial microbiome profiles of house dust in domestic environments. World Allergy Organ J. 2020;13:100452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165. Klepeis NE, Nelson WC, Ott WR, et al. The National Human Activity Pattern Survey (NHAPS): A resource for assessing exposure to environmental pollutants. J Expo Sci Environ Epidemiol. 2001;11:231‐252. [DOI] [PubMed] [Google Scholar]
- 166. Rintala H, Pitkäranta M, Täubel M. Microbial communities associated with house dust. Adv Appl Microbiol. 2012;78:75‐120. [DOI] [PubMed] [Google Scholar]
- 167. Jain N. The early life education of the immune system: Moms, microbes and (missed) opportunities. Gut Microbes. 2020;12:1824564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168. Macher J, Girman J, Alevantis L. Limited water‐to‐air bacterial transfer from a residential evaporative air cooler. Environ Int. 1995;21:761‐764. [Google Scholar]
- 169. Fraser DW, Tsai TR, Orenstein W, et al. Legionnaires' disease: description of an epidemic of pneumonia. New Engl J Med. 1977;297:1189‐1197. [DOI] [PubMed] [Google Scholar]
- 170. Shelton BG, Kerbel W, Witherell L, Millar JD. Review of Legionnaires' disease. AIHAJ‐Am Indus Hyg Assoc. 2000;61:738‐742. [DOI] [PubMed] [Google Scholar]
- 171. Joseph C. Legionnaires' disease in Europe 2000–2002. Epidemiol Infect. 2004;132:417‐424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172. Joseph C, Ricketts K. Legionnaires' disease in Europe 2007–2008. Eurosurveillance. 2010;15:19493. [PubMed] [Google Scholar]
- 173. Shelton BG, Flanders WD, Morris GK. Legionnaires' disease outbreaks and cooling towers with amplified Legionella concentrations. Curr Microbiol. 1994;28:359‐363. [Google Scholar]
- 174. Fields BS, Benson RF, Besser RE. Legionella and Legionnaires' disease: 25 years of investigation. Clin Microbiol Rev. 2002;15:506‐526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175. Hamilton K, Prussin A, Ahmed W, Haas C. Outbreaks of legionnaires' disease and Pontiac fever 2006–2017. Curr Environ Health Rep. 2018;5:263‐271. [DOI] [PubMed] [Google Scholar]
- 176. Elsanousi RMEA. Evaporative coolers air conditioners devices as a source of Legionella Pneumophila in Khartoum state, Sudan and Recommended Measures of Control. Int J Micobiol Biotech. 2020;5:93‐96. [Google Scholar]
- 177. Elsanousi RMA, Elsanousi SM. Detection of Legionella pneumophila from evaporative coolers air conditioners in Khartoum state. Am J Microbiol Res. 2017;5:138‐141. [Google Scholar]
- 178. Cameron S, Roder D, Walker C, Feldheim J. Epidemiological characteristics of legionella infection in South Australia: implications for disease control. Aust NZ J Med. 1991;21:65‐70. [DOI] [PubMed] [Google Scholar]
- 179. Puckorius P. Why evaporative coolers have not caused legionnaires' disease. Energy Fuel. 1995;1995:300. [Google Scholar]
- 180. Wang X, Cheng Z. Cross‐sectional studies: strengths, weaknesses, and recommendations. Chest. 2020;158:S65‐S71. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.