
Figure 1: Proposed mechanisms and biomarkers of sickle cell nephropathy.
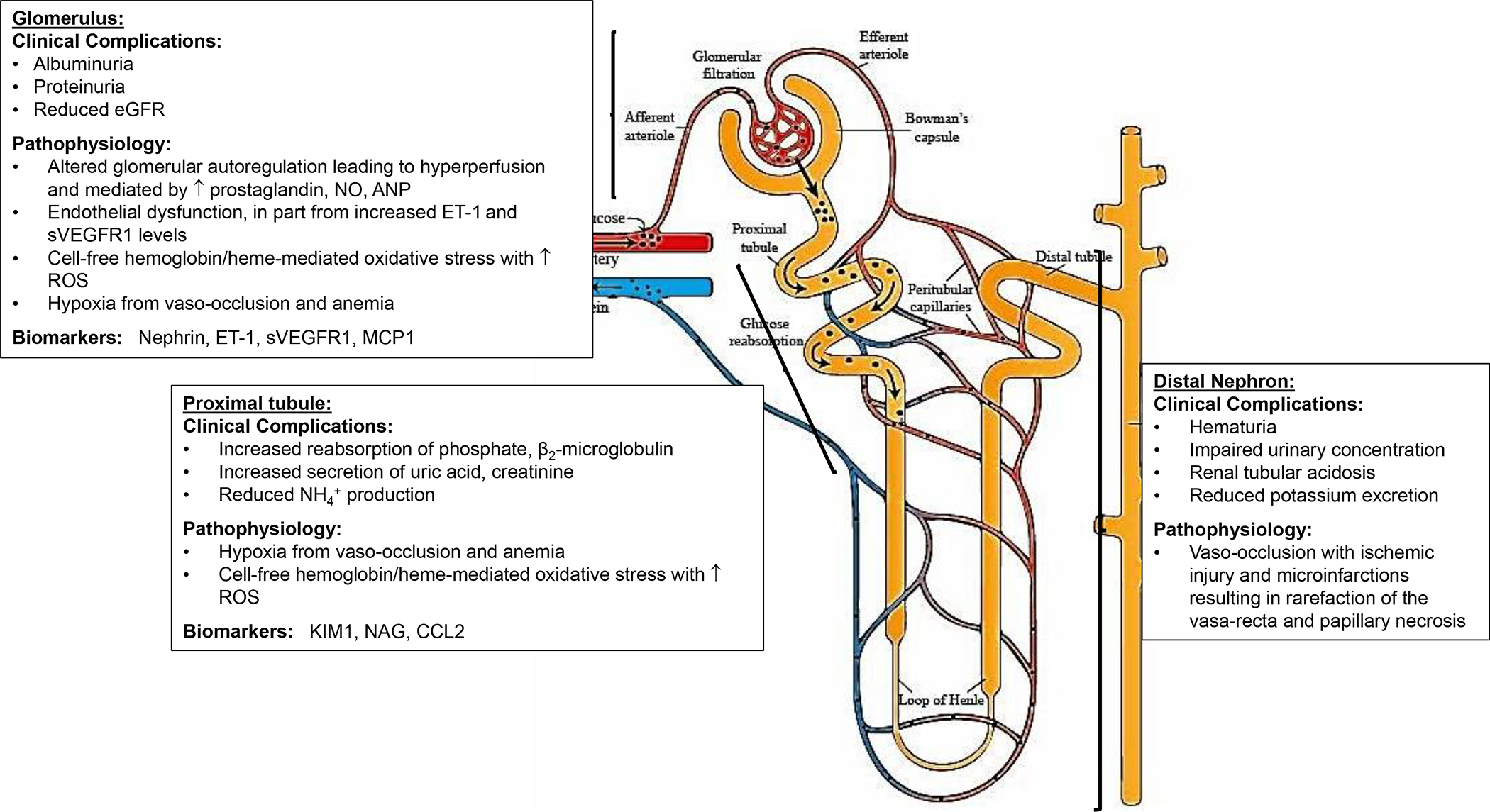
Sickle cell disease is complicated by multiple functional and structural abnormalities that occur along the nephron — clinical complications include hyposthenuria, haematuria, albuminuria and progressive estimated glomerular filtration rate (eGFR) decline. Medullary ischaemia drives localized prostaglandin release and results in marked vasodilation, increasing effective renal blood flow and GFR. In the glomerulus, the pathogenesis of albuminuria seems to be multifactorial — ischaemia-reperfusion injury, haemolysis, oxidative stress, hyperfiltration and glomerular hypertension have all been implicated. ANP, atrial natriuretic peptide; CCL2, CC-chemokine ligand 2; ET1: endothelin 1; KIM1: kidney injury molecule 1; NAG, N-acetyl-β-d-glucosaminidase; NH4+: ammonium ion; NO, nitric oxide; sVEGFR1, soluble vascular endothelial receptor 1; RBC, red blood cell; ROS, reactive oxygen species.