
Figure 2: Approach to screening, evaluation and management of CKD in SCD.
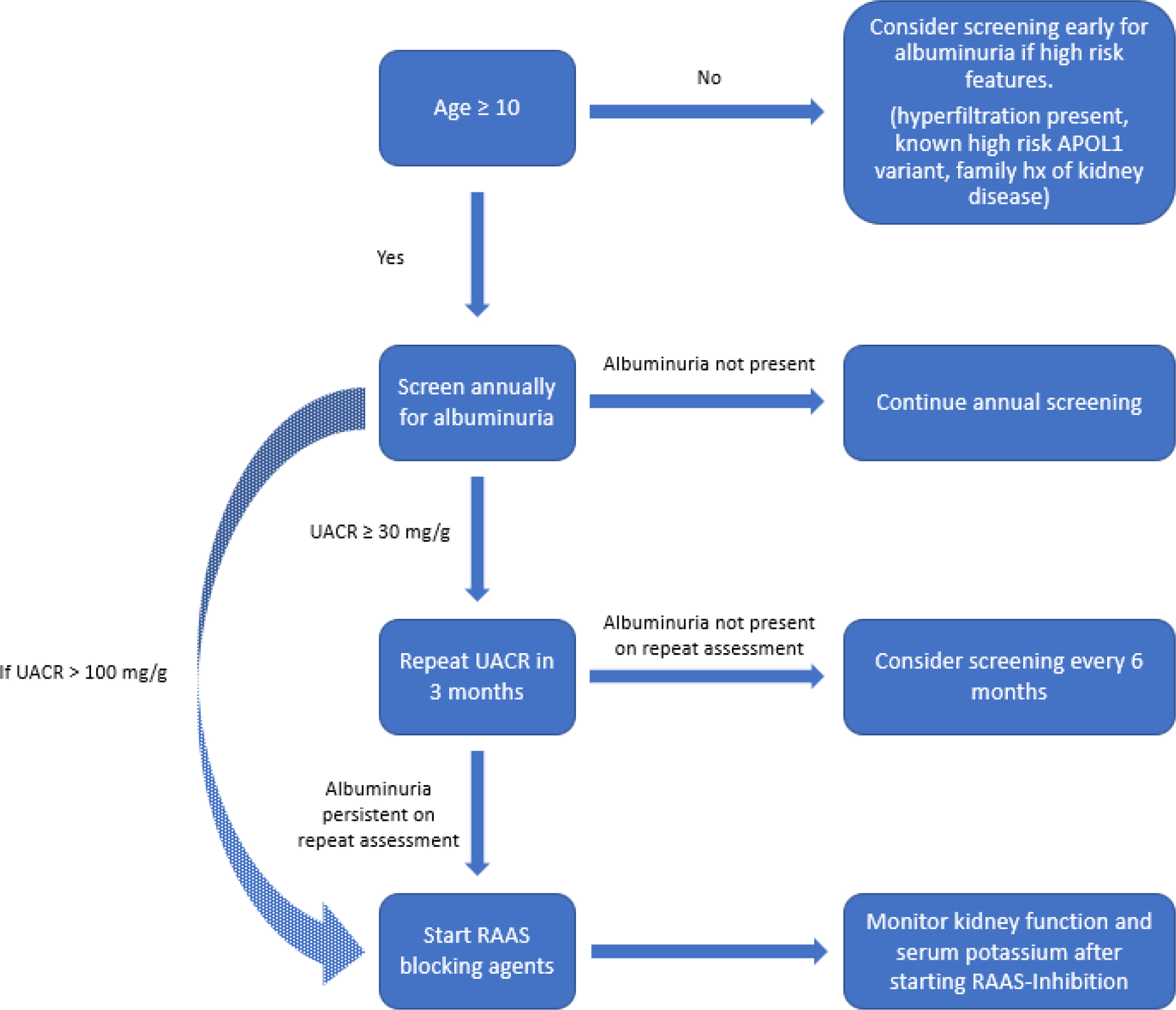
From age 10, patients should be screened for albuminuria at least annually. Repeat evaluation using first-morning void or random urine sample should be obtained to confirm albuminuria, if the initial test is positive. Earlier screening might be considered in the presence of high-risk factors, including glomerular hyperfiltration at an early age, a strong family history of kidney disease or the known presence of APOL1 risk-variants. Renin–angiotensin–aldosterone system (RAAS) blocking agents should be considered in patients with persistent albuminuria or urinary albumin-to-creatinine ratio (UACR) ≥ 100 mg/g. Kidney function (GFR) and serum potassium should be monitored after starting RAAS inhibition. *Although APOL1 testing is available clinically, current data do not support routine screening for APOL1 risk variants.