

Abstract
Background:
Through adequate screening and follow-up, cervical cancer can be prevented or detected at early-stage (stage I), which is related to excellent survival. Current guidelines recommend discontinuing screening for women ≥65 with history of normal Pap and/or HPV tests, potentially leaving this age group vulnerable. This study examined late-stage disease in a population-based cohort.
Methods:
Using California Cancer Registry data, we identified 12,442 patients aged ≥21 years with a first primary cervical cancer diagnosed during 2009–2018. Proportions of late-stage disease (stages II-IV) and early and late-stage 5-year relative survival are presented by age group. Among patients aged ≥65 years, multivariable logistic regression estimated associations of sociodemographic and clinical characteristics with late-stage cervical cancer.
Results:
Nearly one-fifth of patients (n=2,171, 17.4%) were ≥65 years. More women aged ≥65 (71%) presented with late-stage disease than younger women (48% in patients aged <65). Late-stage 5-year relative survival was lower for women ≥65 (23.2%−36.8%) compared to patients <65 (41.5%−51.5%). Characteristics associated with late-stage cervical cancer in women ≥65 included older age (odds ratio (OR)=1.02, 95% confidence interval (CI) 1.01–1.04; each year), non-adenocarcinoma histologic subtypes, and comorbidities (OR=1.59, CI 1.21–2.08).
Conclusions:
There remains a significant burden of advanced cervical cancer in women ≥65.
Impact:
Efforts should be made to better understand how the current screening paradigm is failing women 65 years and older. Future work should focus on determining past screening history, lapses in follow-up care, and non-invasive testing approaches.
Keywords: relative survival, cervical cancer, stage at diagnosis
Introduction:
Although effective screening for cervical cancer exists and can detect pre-malignant lesions and early-stage (stage I) disease (1,2), many women in the United States (US) present with late-stage disease (stages II-IV) (3). Following the introduction and widespread adoption of the Papanicolaou (Pap) smear test in the 1940’s, cervical cancer incidence and mortality have fallen significantly(4,5). However, incidence rates have plateaued since 2012, and rates of invasive cervical cancer have actually increased in recent decades (5). Furthermore, from 2015–2019, nearly half of cervical cancers in the United States were diagnosed late-stage (6). Prior research suggests that women ≥65 had a greater burden of cervical cancer with higher incidence and more late-stage diagnoses (7–10).
The American Cancer Society (ACS), the US Preventive Services Task Force, and the American College of Obstetricians and Gynecologists all recommend that cervical cancer screening end for women >65 years with adequate negative prior screening (3 consecutive normal Pap tests, two consecutive negative HPV tests, or two consecutive negative cotests with Pap and HPV within the prior 10 years, with the most recent screening occurring within the previous five years, and no diagnosis of a precancerous lesion in the past 25 years) (1,11,12). However, 23.2% of women in the U.S. ≥18 are not up-to-date on recommended cervical cancer screening (13). For example, disadvantaged subgroups in the US, including uninsured women and those of lower socioeconomic status were the least likely to report being up to date with cervical cancer screening compared to women of higher educational attainment (13,14). Additionally, screening adherence may decrease as women approach 65, thereby increasing the likelihood that women have not been adequately screened prior to the upper age cutoff (15). As many as 58% of women 64 to 66 years old in a national database failed to meet the criteria to exit screening (16).
We therefore sought to examine cervical cancer stage at diagnosis and relative survival in women ≥65. Previous studies have focused on differences in incidence, mortality, and therapeutic management for younger women (<65) diagnosed with cervical cancer vs. older groups (7,9,15). However, they have not considered adjusted sociodemographic and clinical characteristics associated with late-stage cervical cancer in women ≥65 or associated relative 5-year survival by stage at diagnosis compared to younger age groups within the screening criteria. Therefore, this study utilized large population-based data from the California Cancer Registry (CCR) to examine cervical cancer relative survival by stage at diagnosis and characteristics associated with late-stage disease among women ≥65.
Materials and Methods:
Study Population
The CCR is a state-mandated population-based cancer surveillance system that has collected cancer incidence and patient demographic, diagnostic, and treatment information since 1988. Statewide data are collected through a network of regional registries that are affiliated with the National Cancer Institute’s Surveillance, Epidemiology and End Results program. The CCR has consistently met the highest national standards for data quality and completeness. We used CCR to identify all women ≥21 years who were diagnosed with a first primary cervical cancer in California from 2009–2018, the 10 most recent years for which complete data were available. Cervical cancer was identified using the SEER site recode International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) (17) code 27010 with the histologic subtypes grouped into adenocarcinoma (8098, 8140–8245, 8250–8500), squamous cell carcinoma (8050–8084), and other histologies (8000–8046, 8130, 8246, 8560, 8570, 8720–9473). Patients diagnosed posthumously (n=81) were excluded. In total, 13,485 patients were identified, including 2,420 patients ≥65 years. However, for the main analysis, 1,043 (7.7%) patients diagnosed at unknown stage were excluded; 12,442 total patients and 2,171 ≥65 years remained.
Sociodemographic and clinical characteristics
Patient demographic and clinical characteristics included stage at diagnosis, histologic subtype, comorbidity, neighborhood socioeconomic status (nSES), health insurance status, urbanicity, marital status, race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, Asian/Pacific Islander, and other/unknown), age at diagnosis, and year of diagnosis. Stage at diagnosis was determined by using American Joint Committee on Cancer staging rules (18). We defined early-stage as stage I, as the International Federation of Gynecology and Obstetrics (FIGO) classifies stage I as disease confined to the organ of origin, similar to localized stage; late-stage was classified as stages II-IV as they are similar to regional and distant stages (19).
To capture patient comorbidities, we used a modified Charlson comorbidity score, a weighted index of 16 comorbid conditions, not including cancer, diagnosed from 12 months prior to 6 months following cancer diagnosis (20). Comorbidities were categorized as having none, one, ≥ 2, or missing comorbidity information. nSES is derived using principal components analysis of aggregated 2015–2019 block group level demographic, economic, social, and housing data collected through the American Community Survey using methods described by Yang et al. (21). nSES was categorized into tertiles (lowest, medium, highest). Health insurance was categorized as private/military (health maintenance organization (HMO), preferred provider organization (PPO), Fee-For-Service (FFS), military insurance, and Medicare with supplement), public/Medicaid (Medicaid, county-funded, Indian Health Service or other public health service, Medicare with Medicaid eligibility, Medicare without supplement, Medicaid/Medicare), uninsured, and unknown. Urbanicity was determined using the California Health Manpower Policy Commission Medical Service Study Area (MSSA) urban/rural designation (22).
Statistical Analysis
Five-year relative survival by age group (20–39, 40–59, 60–64, 65–69, 70–74, 75–79, ≥80) and stage at diagnosis were calculated using SEER*Stat software (23). Relative survival was calculated using the US state-county 1992–2016 life tables by SES/ geography/ race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian and Pacific Islander, non-Hispanic American Indian and Alaskan Native, Hispanic), ages 0–99. Relative survival was calculated using the Ederer II method and is a net survival measure that estimates the probability of avoiding death due to cancer in the absence of other causes of death (24). It is defined as the ratio of the observed survival rate among those who have cancer divided by the expected survival rate for people of the same sex, race/ethnicity, and age who do not have cancer, and is expressed as a percentage.
Descriptive statistics (frequencies, percentages) and chi square tests assessed unadjusted associations between cervical cancer stage (early, late) at diagnosis and age group. Among women ≥65 years, multivariable logistic regression was used to assess sociodemographic and clinical characteristics associated with late-stage (stages II-IV vs. I). Models were adjusted for health insurance status, race/ethnicity, nSES, comorbidities, marital status, histologic subtype, year of diagnosis, and age in years. SAS version 9.4 was used to conduct analyses. Collinearity was examined using variance inflation factors and eigenvalues. Results are presented as adjusted odds ratios (OR) and 95% confidence intervals (CI). A two-sided P-value < 0.05 was considered statistically significant. Sensitivity analyses were conducted including unknown stage with stages II-IV because Kaplan-Meyer curves indicated that survival for those with unknown stage at diagnosis was similar to those with stage IV diagnosis and we wanted to assess the impact of excluding unknown stage at diagnosis on associations in our main analyses. All analyses were overseen by the Institutional Review Board of the University of California, Davis.
Data Availability:
The data analyzed in this study are available from the California Cancer Registry. Access is granted through an application process by the management or data custodians (https://www.ccrcal.org/retrieve-data/).
Results:
Among 12,442 women diagnosed from 2009–2018 with a first primary cervical cancer, 17.4% (2,171) were aged ≥65 years (Table 1). The proportion of women diagnosed late stage increased with increasing age through age 75 to 79 (Figure 1). Among women ≥65 years, the proportion diagnosed late stage ranged from 60.2% to 70.6% compared to 33.5% to 58.7% for those ages 21 to 64 years. Among women diagnosed with early-stage disease, 5-year relative survival was lowest for women 80 years and older at 51.6%. For those 20–39, 40–59, 60–64, 65–69, 70–74, and 75–79,5-year relative survival was 93.6%, 92.9%, 89.3% 81.5%, 86.2%, and 72.0%respectively. Likewise, among those with late-stage cervical cancer, 5-year relative survival was lowest for women 80 years and older at only 23.2%. For those 20–39, 40–59, 60–64, 65–69, 70–74, and 75–79, 5-year relative survival was 51.5%, 47.5%, 41.5%, 36.8%, 39.1%, and 30.8% respectively (Figure 2).
Table 1.
Characteristics of Cervical Cancer Patients Diagnosed 2009-2018 in California by Age Group and Stage (N=12,442)
| 21–64 | 65+ | |||||
|---|---|---|---|---|---|---|
| N=10,271 (82.6%) | N=2,171 (17.4%) | |||||
| Stage I | Stage II-IV | Stage I | Stage II-IV | |||
| Characteristics | N (%) | N (%) | P* | N (%) | N (%) | P* |
|
| ||||||
| Age Group | <.0001 | |||||
| 21–39 | 2162 (40.2) | 1204 (24.6) | ||||
| 40–59 | 2809 (52.2) | 2995 (61.2) | ||||
| 60–64 | 406 (7.6) | 695 (14.2) | <.0001 | |||
| 65–69 | 261 (41.6) | 490 (31.7) | ||||
| 70–74 | 151 (24.1) | 386 (25.0) | ||||
| 75–79 | 88 (14.0) | 293 (19.0) | ||||
| 80+ | 127 (20.3) | 375 (24.3) | ||||
|
| ||||||
| Year of Diagnosis | 0.0406 | 0.9414 | ||||
| 2009–2012 | 2207 (41.0) | 1926 (39.4) | 241 (38.4) | 581 (37.7) | ||
| 2013–2015 | 1529(28.4) | 1501 (30.7) | 187 (29.8) | 468 (30.3) | ||
| 2016–2018 | 1641 (30.5) | 1467 (30.0) | 199 (31.7) | 494 (32.0) | ||
|
| ||||||
| Marital Status | <.0001 | 0.0004 | ||||
| Married | 2592 (48.2) | 1952 (39.9) | 235 (37.5) | 475 (30.8) | ||
| Not Married | 2482 (46.2) | 2776 (56.7) | 349 (55.7) | 995 (64.5) | ||
| Unknown | 303 (5.6) | 166 (3.4) | 43 (6.9) | 73 (4.7) | ||
|
| ||||||
| Health Insurance | <.0001 | 0.0806 | ||||
| Private/military | 3330 (61.9) | 2107 (43.1) | 251 (40.0) | 579 (37.5) | ||
| Public/Medicaid | 1780 (33.1) | 2535 (51.8) | 353 (56.3) | 914 (59.2) | ||
| Uninsured | 143 (2.7) | 142 (2.9) | 4 (0.6) | 22 (1.4) | ||
| Unknown | 124 (2.3) | 110 (2.2) | 19 (3.0) | 28 (1.8) | ||
|
| ||||||
| Socioeconomic Status | <.0001 | 0.2017 | ||||
| Lowest | 2018 (37.5) | 2276 (46.5) | 224 (35.7) | 613 (39.7) | ||
| Medium | 1900 (35.3) | 1677 (34.3) | 225 (35.9) | 531 (34.4) | ||
| Highest | 1459 (27.1) | 941 (19.2) | 178 (28.4) | 399 (25.9) | ||
|
| ||||||
| Race/ Ethnicity | <.0001 | 0.0532 | ||||
| Non-Hispanic white | 2104 (39.1) | 1741 (35.6) | 246 (39.2) | 627 (40.6) | ||
| Non-Hispanic black | 269 (5.0) | 353 (7.2) | 39 (6.2) | 107 (6.9) | ||
| Hispanic | 2142 (39.8) | 2001 (40.9) | 211 (33.7) | 478 (31.0) | ||
| Asian/Pacific Islander | 747 (13.9) | 738 (15.1) | 119 (19.0) | 321 (20.8) | ||
| Other/ Unknown | 115 (2.1) | 61 (1.2) | 12 (1.9) | 10 (0.6) | ||
|
| ||||||
| Rural/ Urban | 0.0667 | 0.5607 | ||||
| Rural | 661 (12.3) | 661 (13.5) | 80 (12.8) | 183 (11.9) | ||
| Urban | 4716 (87.7) | 4233 (86.5) | 547 (87.2) | 1360 (88.1) | ||
|
| ||||||
| Comorbidities | <.0001 | 0.0003 | ||||
| 0 | 3365 (62.6) | 2622 (53.6) | 281 (44.8) | 595 (38.6) | ||
| 1 | 592 (11.0) | 685 (14.0) | 133 (21.2) | 283 (18.3) | ||
| >1 | 189 (3.5) | 530 (10.8) | 102 (16.3) | 369 (23.9) | ||
| Missing | 1231 (22.9) | 1057 (21.6) | 111 (17.7) | 296 (19.2) | ||
|
| ||||||
| Histology | <.0001 | <.0001 | ||||
| Adenocarcinoma | 2060 (38.3) | 968 (19.8) | 170 (27.1) | 298 (19.3) | ||
| Squamous Cell Carcinoma | 2966 (55.2) | 3401 (69.5) | 420 (67.0) | 1070 (69.3) | ||
| Other | 351 (6.5) | 525 (10.7) | 37 (5.9) | 175 (11.3) | ||
Chi-square p-value
Figure 1.
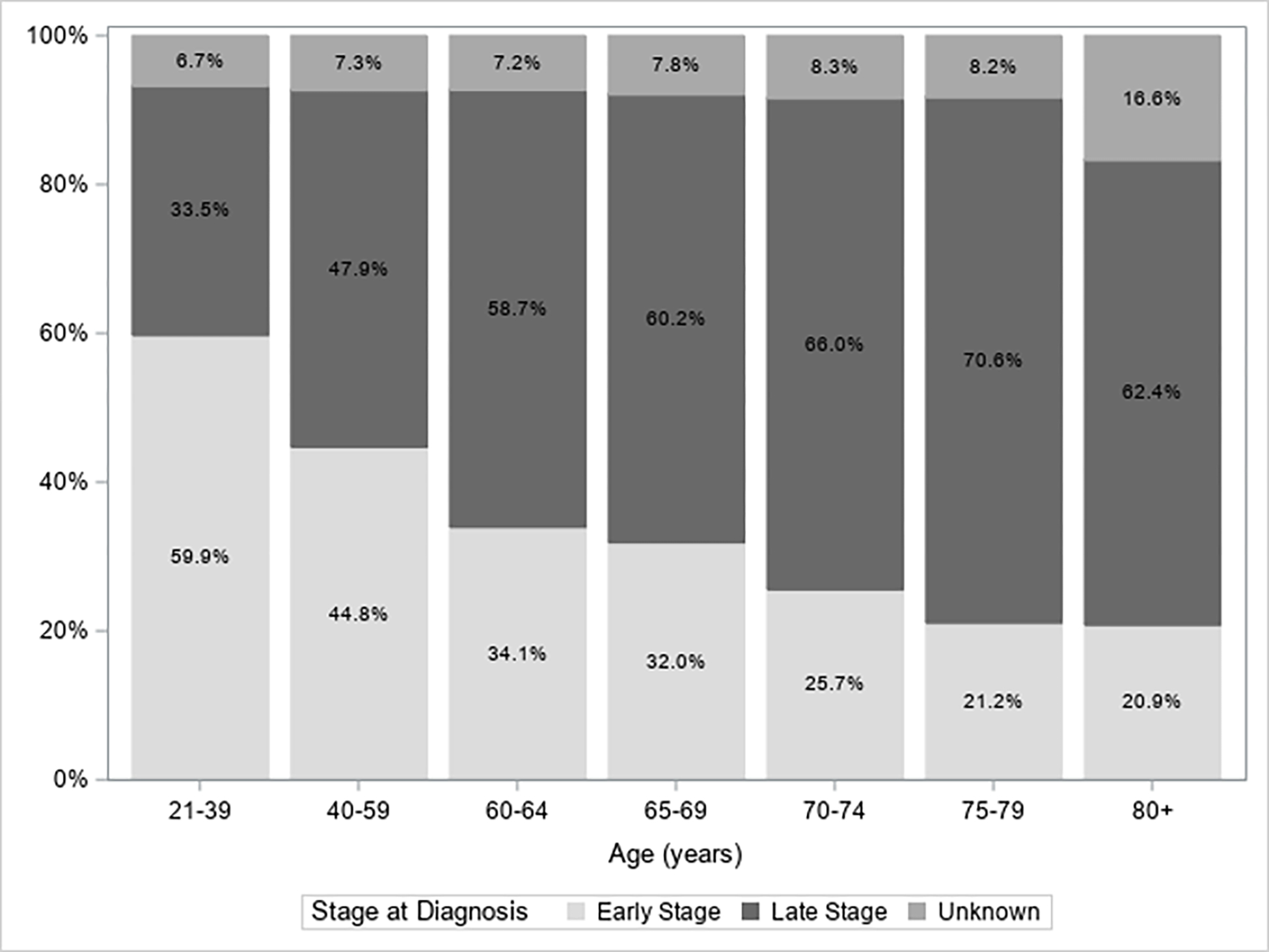
Stage at Cervical Cancer Diagnosis by Age Group, 2009–2018 (N=13,485)
Bar chart showing the percentage of women diagnosed early, late, or unknown stage by seven age groupings.
Figure 2.
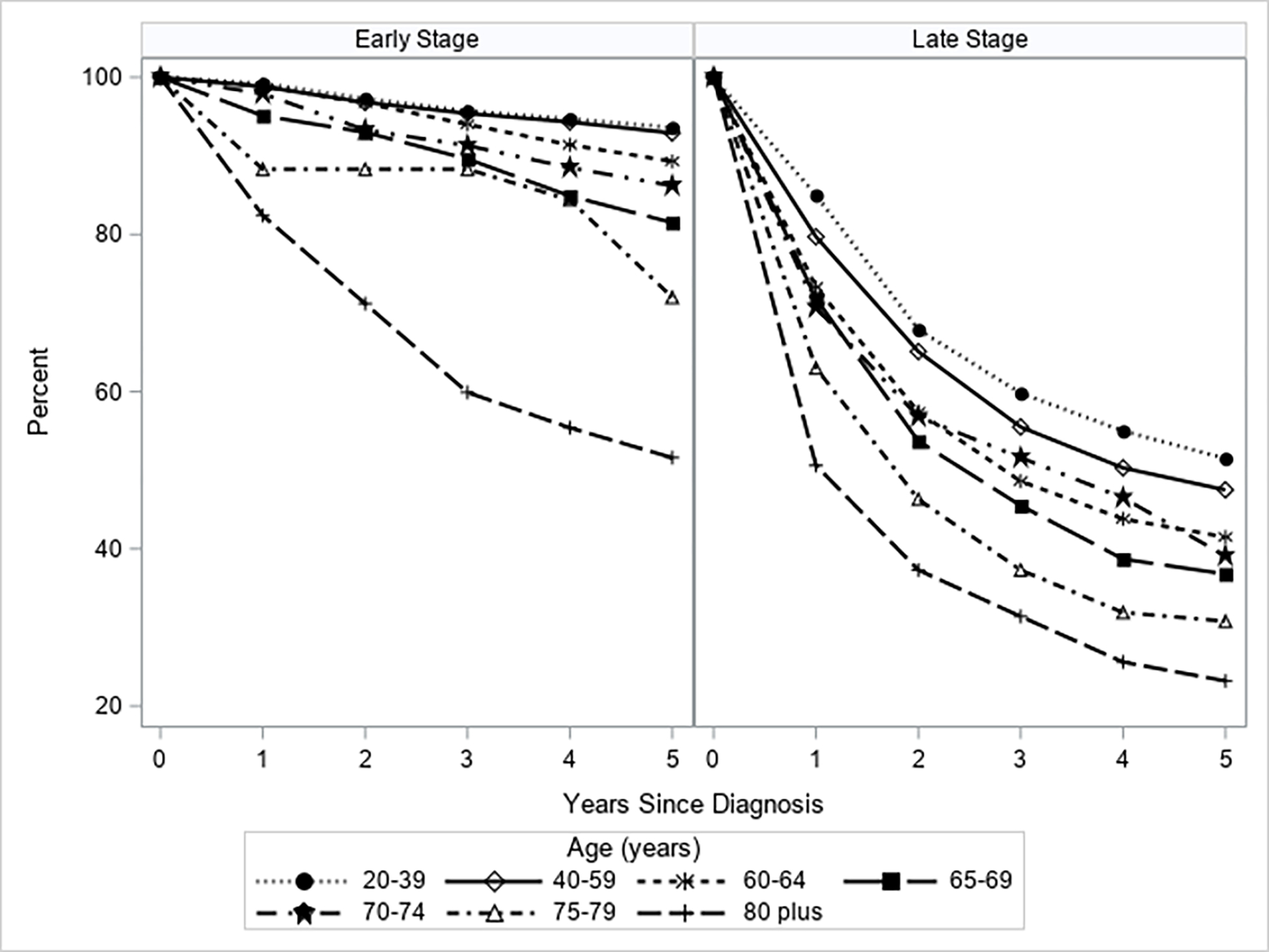
Relative Survival for Cervical Cancer Patients by Stage at Diagnosis and Age Group, 2009–2018
Series plot showing relative survival rates over five years by seven age groupings. Left panel shows relative survival rates for women diagnosed early stage and right panel shows relative survival rates for women diagnosed late stage.
Of 2,171 women ≥65, most patients were aged 65–69 (34.6%) followed by 70–74 (24.7%), 80 plus (23.1%) and 75–79 (17.5%). More women with early-stage disease at diagnosis were younger (65.7% 65–74 years and 34.3% ages 75 years and older) compared to women with lates-stage disease at diagnosis (56.7% 65–74 years and 43.3% ages75 years and older). The most common histologic subtype for both early-stage and late-stage diagnoses was squamous cell carcinoma (67.0% early-stage; 69.3% late-stage), followed by adenocarcinoma (27.1% early-stage; 19.3% late-stage), and other subtypes (5.9% early-stage; 11.3% late-stage) (Table 1). Compared to patients diagnosed at early-stage, those diagnosed at late-stage had ≥ 2 comorbidities, were unmarried, and had non-adenocarcinoma histologic subtypes.
In multivariable logistic regression models, among patients ≥65, factors associated with late-stage included older age at diagnosis (increase with each additional year of age, OR 1.02; CI, 1.01, 1.04), ≥ 2 comorbidities (vs. no comorbidities: OR, 1.59; CI, 1.21, 2.08), squamous cell carcinoma histology (OR, 1.38; CI 1.10, 1.74), or other subtypes (OR, 2.52; CI 1.68, 3.79) vs. adenocarcinoma (Table 2). Women of Hispanic ethnicity were less likely to be diagnosed with late-stage disease (OR 0.76; CI 0.60, 0.97) compared to non-Hispanic White women. Year of diagnosis, marital status, health insurance status, nSES, and urbanicity were not shown to be significantly associated with late-stage cervical cancer.
Table 2.
Association between sociodemographic and clinical characteristics with late-stage (II-IV) cervical cancer diagnosis for patients ≥65 years, 2009–2018 (N=2,171)
| Characteristics | OR Estimate (95% CI) |
|---|---|
|
| |
| Age | |
| Each year increase | 1.02 (1.01, 1.04) |
|
| |
| Year of Diagnosis | |
| 2009–2012 | Reference |
| 2013–2015 | 1.04 (0.83, 1.32) |
| 2016–2018 | 1.04 (0.83, 1.32) |
|
| |
| Marital Status | |
| Married | Reference |
| Not Married | 1.22 (0.93, 1.60) |
| Unknown | 0.80 (0.52, 1.24) |
|
| |
| Health Insurance | |
| Private/military | Reference |
| Public/Medicaid | 1.09 (0.89, 1.34) |
| Uninsured | 2.19 (0.73, 6.54) |
| Unknown | 0.76 (0.40, 1.45) |
|
| |
| Neighborhood Socioeconomic Status (Tertile) | |
| Highest | Reference |
| Lowest | 1.27 (0.98, 1.64) |
| Medium | 1.08 (0.85, 1.38) |
|
| |
| Race/Ethnicity | |
| Non-Hispanic White | Reference |
| Non-Hispanic Black | 0.86 (0.57, 1.30) |
| Hispanic | 0.76 (0.60, 0.97) |
| Asian/Pacific Islander | 1.04 (0.79, 1.36) |
| Other/Unknown | 0.35 (0.14, 0.86) |
|
| |
| Rural residence | |
| Urban | Reference |
| Rural | 0.97 (0.72, 1.30) |
|
| |
| Comorbidity Score | |
| 0 | Reference |
| 1 | 0.99 (0.77, 1.28) |
| >1 | 1.59 (1.21, 2.08) |
| Unknown | 1.22 (0.93, 1.60) |
|
| |
| Histology | |
| Adenocarcinoma | Reference |
| Squamous Cell Carcinoma | 1.38 (1.10, 1.74) |
| Other | 2.52 (1.68, 3.79) |
Abbreviations: OR, odds ratio; CI, confidence interval
In sensitivity analyses including unknown stage at diagnosis with late-stage, unmarried women were more likely to be diagnosed late-stage (OR 1.27; CI 1.04, 1.56) (Table S1). Late-stage disease was associated with older age, comorbidity, non-adenocarcinoma histology and less associated with Hispanic ethnicity, consistent with the main analysis that excluded unknown stage.
Discussion
In our large population-based study in California, nearly 1 in 5 new cervical cancer cases diagnosed from 2009–2018 were in women ≥65, and these older women had lower 5-year relative survival for both early- and late-stage diagnoses than younger women, with women 80 years and older having the lowest survival of all age groups. We also observed that the proportions of late-stage diagnoses increased up to age 79 years. Among women ≥65, those who were older, had non-adenocarcinoma histology, and had comorbidities were more likely to be diagnosed with late-stage disease.
Our study confirms findings from prior US-based studies that have noted substantial burden of cervical cancer, high rates of late-stage disease, and worse survival in women ≥65 (7–10,15). However, to our knowledge, prior studies have not examined cervical cancer 5-year relative survival by age group and stage at diagnosis. Our study found worsening 5-year relative survival with each increasing age grouping category for both early and late-stage diagnoses.
While we cannot determine the reason for these age disparities with our data, several factors may contribute. More late-stage diagnoses may be due to inadequate screening in women approaching 65 as noted previously (15). Some reasons cited for forgoing screening include discomfort, pain, embarrassment, and the intrusiveness of speculum-based exams (25,26). Another reason can be lack of follow-up after an abnormal screen. As many as 50% of women with abnormal results do not receive follow-up care (27,28). Comorbidities can also contribute to late-stage cancer diagnoses. Comorbidities increase with age and can result in a delayed diagnosis because of distraction from other health issues (29,30). Worse survival with older age can result from more late-stage diagnoses but can also result from less aggressive treatments in women ≥65. Eggemann et al. reported that patients ≥ 61 were less likely to undergo surgery and radiochemotherapy compared to patients <61 (31). Diver et al. likewise found that women ≥65 were less likely to receive surgery (7).
Another issue that could contribute to late-stage diagnosis is the use of supracervical hysterectomy. This procedure leaves the cervix intact and accounted for approximately 7.1% of laparoscopic hysterectomies in 2016 in the US (32). Unfortunately, some women do not realize the need to continue screening; Mattingly et al. found that only 67% of women who had undergone minimally invasive hysterectomy correctly identified whether their cervix had been removed and if they needed screening (33). McHale et al. found that 5.3% of women undergoing a secondary resection of a retained cervix after supracervical hysterectomy had cervical cancer (34).
Despite adequate prior screening, some women ≥65 are still diagnosed with cervical cancer (35,36). Pap testing can be difficult post-menopause when cytology tests may become less sensitive due to retraction of the squamocolumnar junction and vulvovaginal and cervical epithelium atrophy (26,37). Additionally, Pap testing is more effective at detecting squamous cell carcinoma and its precursors than adenocarcinoma which has been increasing in incidence (35,38,39). However, our study found that women with non-adenocarcinoma histologies were more likely to be diagnosed late-stage.
HPV testing provides increased sensitivity for cervical cancer precursors compared to Pap smear testing (11,40,41), but there is evidence that many women approaching age65 have not received HPV testing (42) and acceptance of it has been found to be low (43). Less intrusive options for HPV testing are becoming available including self-testing through vaginal swabs and urine collection and have been successfully used in other countries (44–47). Self-testing has been shown to be accurate and a good alternative to speculum-based exams that can be a reason to delay or altogether avoid testing as noted (25,48).
Year of diagnosis was not associated with stage at diagnosis, indicating that the proportion of late-stage cervical cancer diagnosis has not changed over time among women ≥65 in California. This differs from a previous US study that found that the proportion of regional and distant cervical cancer has in fact increased from 2001–2009 in most states, which might have been driven by the removal of pre-malignant lesions and the resulting increase in the proportion of invasive cervical cancer in unscreened women and those who did not receive adequate follow-up (49). However, our data are more recent and restricted to women ≥65, for many of whom advances in screening technologies and changes in guidelines were not applicable. This highlights the importance of ensuring women ≥65 have met the screening criteria prior to exiting as well as strategies aimed at enhancing follow-up after abnormal screening tests.
Prior studies of younger women have found increased late-stage cervical cancer diagnoses among women of Hispanic ethnicity, African American/Black race, and lower SES (49–51). Our study did not observe these associations and instead found that older Hispanic women were less likely than non-Hispanic White women to be diagnosed late-stage. Consistent with prior studies (8), our sensitivity analyses suggest that unmarried women ≥65 were diagnosed more often with late-stage cervical cancer. Increased late-stage diagnosis in unmarried patients could be related in part to differences in exposure to sexually transmitted infections between unmarried women and married women, as HPV is the causative agent in approximately 91% of cervical cancer cases (52). While the percent of HPV cases attributable to reactivation remains constant with age (18%−36%), the remaining HPV infections are caused by sexual exposure (53). The risk of acquiring HPV increases for women with new, casual, or concurrent sexual partners (53). Additionally, unmarried patients may be diagnosed late-stage more often due to economic disadvantage and less social, emotional, and practical support compared to married patients (54).
Our study had some limitations. We were unable to determine adherence to screening guidelines of our cohort or capture any HPV information, such as new or recurring infection. Additionally, we excluded 10.3% of women ≥65 (n=249) with unknown stage from our main analysis. However, when we included these women in our sensitivity analysis, our logistic regression results were similar. Despite these limitations, we utilized high-quality, large, population-based registry data to evaluate the stage at diagnosis and associated relative survival of women ≥65 diagnosed with cervical cancer.
In California, nearly one fifth of cervical cancers were diagnosed in women ≥65 and the majority were late-stage. Late-stage cervical cancer diagnoses increased with age and were associated with low 5-year relative survival of 36.8% to 23.2%. Our findings highlight the need to better understand how the current screening paradigm might be failing women ≥65. Future work should focus on determining past screening history of older women, determining lapses in follow-up care, and non-invasive testing approaches for women nearing age 65 or those who might need catch up screening.
Supplementary Material
Acknowledgements:
Research reported in this publication was supported by the UC Davis Comprehensive Cancer Center and National Cancer Institute of the National Institutes of Health under award number P30CA093373 (T.H. Keegan). The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 5NU58DP006344; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors.
Footnotes
Conflict of interest statement: We declare no conflict of interest.
References
- 1.Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, et al. Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement. JAMA : the journal of the American Medical Association 2018;320(7):674–86 doi 10.1001/jama.2018.10897. [DOI] [PubMed] [Google Scholar]
- 2.Yang DX, Soulos PR, Davis B, Gross CP, Yu JB. Impact of Widespread Cervical Cancer Screening: Number of Cancers Prevented and Changes in Race-specific Incidence. American journal of clinical oncology 2018;41(3):289–94 doi 10.1097/coc.0000000000000264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA: a cancer journal for clinicians 2020;70(1):7–30 doi 10.3322/caac.21590. [DOI] [PubMed] [Google Scholar]
- 4.Vaccarella S, Lortet-Tieulent J, Plummer M, Franceschi S, Bray F. Worldwide trends in cervical cancer incidence: impact of screening against changes in disease risk factors. Eur J Cancer 2013;49(15):3262–73 doi 10.1016/j.ejca.2013.04.024. [DOI] [PubMed] [Google Scholar]
- 5.Howlader N NA, Krapcho M, Miller D, Bishop K, et al. SEER Cancer Statistics Review, 1975–2017. Bethesda, MD: National Cancer Institute; 2020. [Google Scholar]
- 6.U.S. Cancer Statistics Working Group. 2022. U.S. Cancer Statistics Data Visualizations Tool, based on 2021 submission data (1999–2019). U.S. Department of Health and Human Services, Centers for Disease control and Prevention and national Cancer Institute; <www.cdc.gov/cancer/dataviz>. Accessed 2022 September 4. [Google Scholar]
- 7.Diver EJ, Hinchcliff EM, Gockley AA, Melamed A, Contrino L, Feldman S, et al. Assessment of treatment factors and clinical outcomes in cervical cancer in older women compared to women under 65 years old. Journal of geriatric oncology 2018;9(5):516–9 doi 10.1016/j.jgo.2018.02.004. [DOI] [PubMed] [Google Scholar]
- 8.Saghari S, Ghamsary M, Marie-Mitchell A, Oda K, Morgan JW. Sociodemographic predictors of delayed- versus early-stage cervical cancer in California. Annals of epidemiology 2015;25(4):250–5 doi 10.1016/j.annepidem.2015.01.008. [DOI] [PubMed] [Google Scholar]
- 9.Feldman S, Cook E, Davis M, Gershman ST, Hanchate A, Haas JS, et al. Cervical Cancer Incidence Among Elderly Women in Massachusetts Compared With Younger Women. Journal of lower genital tract disease 2018;22(4):314–7 doi 10.1097/lgt.0000000000000435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Quick AM, Krok-Schoen JL, Stephens JA, Fisher JL. Cervical Cancer Among Older Women: Analyses of Surveillance, Epidemiology and End Results Program Data. Cancer control : journal of the Moffitt Cancer Center 2020;27(1):1073274820979590 doi 10.1177/1073274820979590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fontham ETH, Wolf AMD, Church TR, Etzioni R, Flowers CR, Herzig A, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA: a cancer journal for clinicians 2020;70(5):321–46 doi 10.3322/caac.21628. [DOI] [PubMed] [Google Scholar]
- 12.Updated Cervical Cancer Screening Guidelines. 2021. Practice Advisory. American College of Obstetricians and Gynecologists <https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2021/04/updated-cervical-cancer-screening-guidelines>. Accessed 2022 August 30.
- 13.Sabatino SA, Thompson TD, White MC, Shapiro JA, Clarke TC, Croswell JM, et al. Cancer Screening Test Use-U.S., 2019. American journal of preventive medicine 2022;63(3):431–9 doi 10.1016/j.amepre.2022.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moss JL, Roy S, Shen C, Cooper JD, Lennon RP, Lengerich EJ, et al. Geographic Variation in Overscreening for Colorectal, Cervical, and Breast Cancer Among Older Adults. JAMA Netw Open 2020;3(7):e2011645 doi 10.1001/jamanetworkopen.2020.11645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.White MC, Shoemaker ML, Benard VB. Cervical Cancer Screening and Incidence by Age: Unmet Needs Near and After the Stopping Age for Screening. American journal of preventive medicine 2017;53(3):392–5 doi 10.1016/j.amepre.2017.02.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mills JM, Morgan JR, Dhaliwal A, Perkins RB. Eligibility for cervical cancer screening exit: Comparison of a national and safety net cohort. Gynecologic oncology 2021;162(2):308–14 doi 10.1016/j.ygyno.2021.05.035. [DOI] [PubMed] [Google Scholar]
- 17.NCI Surveillance Epidemiology and End Results Program. 2008. Site Recode ICD-O-3/WHO 2008 Definition. <https://seer.cancer.gov/siterecode/icdo3_dwhoheme/>. Accessed 2022 August 31.
- 18.Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, A T. AJCC cancer staging manual New York, NY: Springer; 2010. [Google Scholar]
- 19.Bhatla N, Berek JS, Cuello Fredes M, Denny LA, Grenman S, Karunaratne K, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet 2019;145(1):129–35 doi 10.1002/ijgo.12749. [DOI] [PubMed] [Google Scholar]
- 20.Lichtensztajn DY, Giddings BM, Morris CR, Parikh-Patel A, Kizer KW. Comorbidity index in central cancer registries: the value of hospital discharge data. Clinical epidemiology 2017;9:601–9 doi 10.2147/clep.s146395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yang J SC, Harrati A, Clarke C, Keegan THM, Gomez SL,. Developing an area-based socioeconomic measure from American Community Survey data. Fremont, California: Cancer Prevention Institute of California; 2014. [Google Scholar]
- 22.California Health and Human Services Agency. 2022 Medical Service Study Area (MSSA) Detail. California Health and Human Services Open Data Portal <https://data.chhs.ca.gov/dataset?q=MSSA>. Accessed 2022 March 12.
- 23.Surveillance Research Program. National Cancer Institute SEER*Stat software. <https://seer.cancer.gov/seerstat/>. Accessed 2022 February 3.
- 24.Lambert PC, Dickman PW, Rutherford MJ. Comparison of different approaches to estimating age standardized net survival. BMC Med Res Methodol 2015;15:64 doi 10.1186/s12874-015-0057-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.O’Laughlin DJ, Strelow B, Fellows N, Kelsey E, Peters S, Stevens J, et al. Addressing Anxiety and Fear during the Female Pelvic Examination. J Prim Care Community Health 2021;12:2150132721992195 doi 10.1177/2150132721992195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Freeman M, Waller J, Sasieni P, Lim AW, Marlow LA. Acceptability of non-speculum clinician sampling for cervical screening in older women: A qualitative study. J Med Screen 2018;25(4):205–10 doi 10.1177/0969141318756452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Harper DM. Cervical Cancer Elimination Is Dependent on Women’s Self-Tests for Primary Human Papillomavirus Testing Triaged by Methylation Status. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2022:Jco2200609 doi 10.1200/jco.22.00609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Perkins RB, Adcock R, Benard V, Cuzick J, Waxman A, Howe J, et al. Clinical follow-up practices after cervical cancer screening by co-testing: A population-based study of adherence to U.S. guideline recommendations. Preventive medicine 2021;153:106770 doi 10.1016/j.ypmed.2021.106770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Terret C, Castel-Kremer E, Albrand G, Droz JP. Effects of comorbidity on screening and early diagnosis of cancer in elderly people. The Lancet Oncology 2009;10(1):80–7 doi 10.1016/s1470-2045(08)70336-x. [DOI] [PubMed] [Google Scholar]
- 30.Sarfati D, Koczwara B, Jackson C. The impact of comorbidity on cancer and its treatment. CA: a cancer journal for clinicians 2016;66(4):337–50 doi 10.3322/caac.21342. [DOI] [PubMed] [Google Scholar]
- 31.Eggemann H, Ignatov T, Geyken CH, Seitz S, Ignatov A. Management of elderly women with cervical cancer. Journal of cancer research and clinical oncology 2018;144(5):961–7 doi 10.1007/s00432-018-2617-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Desai VB, Wright JD, Lin H, Gross CP, Sallah YH, Schwartz PE, et al. Laparoscopic Hysterectomy Route, Resource Use, and Outcomes: Change After Power Morcellation Warning. Obstetrics and gynecology 2019;134(2):227–38 doi 10.1097/aog.0000000000003375. [DOI] [PubMed] [Google Scholar]
- 33.Mattingly M, Juran R, Su I, Ebinger J, Daggy J, Tucker Edmonds B. Patient knowledge of hysterectomy and pap screening after minimally invasive hysterectomy. Patient education and counseling 2017;100(1):121–5 doi 10.1016/j.pec.2016.08.017. [DOI] [PubMed] [Google Scholar]
- 34.McHale MP, Smith AJB, Fader AN, Wethington SL. Outcomes of Women Undergoing Excision of the Retained Cervix After Supracervical Hysterectomy. Obstetrics and gynecology 2021;137(5):831–6 doi 10.1097/aog.0000000000004360. [DOI] [PubMed] [Google Scholar]
- 35.Yost S, Hoekstra A. Cervical cancer in women over 65: An analysis of screening. Gynecol Oncol Rep 2018;25:48–51 doi 10.1016/j.gore.2018.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gnade CM, Hill EK, Botkin HE, Hefel AR, Hansen HE, Sheets KA, et al. Is the age of cervical cancer diagnosis changing over time? J Gynecol Obstet Hum Reprod 2021;50(7):102040 doi 10.1016/j.jogoh.2020.102040. [DOI] [PubMed] [Google Scholar]
- 37.Gustafson LW, Petersen LK, Bor P, Andersen B, Hammer A. Cervical cancer prevention among older women - challenges in screening, diagnostic workup and treatment. Acta Obstet Gynecol Scand 2021;100(8):1364–8 doi 10.1111/aogs.14162. [DOI] [PubMed] [Google Scholar]
- 38.Pak SC, Martens M, Bekkers R, Crandon AJ, Land R, Nicklin JL, et al. Pap smear screening history of women with squamous cell carcinoma and adenocarcinoma of the cervix. The Australian & New Zealand journal of obstetrics & gynaecology 2007;47(6):504–7 doi 10.1111/j.1479-828X.2007.00788.x. [DOI] [PubMed] [Google Scholar]
- 39.Islami F, Fedewa SA, Jemal A. Trends in cervical cancer incidence rates by age, race/ethnicity, histological subtype, and stage at diagnosis in the United States. Preventive medicine 2019;123:316–23 doi 10.1016/j.ypmed.2019.04.010. [DOI] [PubMed] [Google Scholar]
- 40.Melnikow J, Henderson JT, Burda BU, Senger CA, Durbin S, Weyrich MS. Screening for Cervical Cancer With High-Risk Human Papillomavirus Testing: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA : the journal of the American Medical Association 2018;320(7):687–705 doi 10.1001/jama.2018.10400. [DOI] [PubMed] [Google Scholar]
- 41.Ogilvie GS, van Niekerk D, Krajden M, Smith LW, Cook D, Gondara L, et al. Effect of Screening With Primary Cervical HPV Testing vs Cytology Testing on High-grade Cervical Intraepithelial Neoplasia at 48 Months: The HPV FOCAL Randomized Clinical Trial. JAMA : the journal of the American Medical Association 2018;320(1):43–52 doi 10.1001/jama.2018.7464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.MacLaughlin KL, Jacobson RM, Radecki Breitkopf C, Wilson PM, Jacobson DJ, Fan C, et al. Trends Over Time in Pap and Pap-HPV Cotesting for Cervical Cancer Screening. Journal of women’s health (2002) 2019;28(2):244–9 doi 10.1089/jwh.2018.7380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Saraiya M, Kwan A, Cooper CP. Primary HPV testing: U.S. women’s awareness and acceptance of an emerging screening modality. Preventive medicine 2018;108:111–4 doi 10.1016/j.ypmed.2017.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hwang SH, Shin HY, Lee DO, Sung NY, Lee B, Lee DH, et al. A prospective pilot evaluation of vaginal and urine self-sampling for the Roche cobas 4800 HPV test for cervical cancer screening. Sci Rep 2018;8(1):9015 doi 10.1038/s41598-018-27390-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Maver PJ, Poljak M. Primary HPV-based cervical cancer screening in Europe: implementation status, challenges, and future plans. Clin Microbiol Infect 2020;26(5):579–83 doi 10.1016/j.cmi.2019.09.006. [DOI] [PubMed] [Google Scholar]
- 46.Polman NJ, Snijders PJF, Kenter GG, Berkhof J, Meijer C. HPV-based cervical screening: Rationale, expectations and future perspectives of the new Dutch screening programme. Preventive medicine 2019;119:108–17 doi 10.1016/j.ypmed.2018.12.021. [DOI] [PubMed] [Google Scholar]
- 47.Serrano B, Ibáñez R, Robles C, Peremiquel-Trillas P, de Sanjosé S, Bruni L. Worldwide use of HPV self-sampling for cervical cancer screening. Preventive medicine 2022;154:106900 doi 10.1016/j.ypmed.2021.106900. [DOI] [PubMed] [Google Scholar]
- 48.Inturrisi F, Aitken CA, Melchers WJG, van den Brule AJC, Molijn A, Hinrichs JWJ, et al. Clinical performance of high-risk HPV testing on self-samples versus clinician samples in routine primary HPV screening in the Netherlands: An observational study. Lancet Reg Health Eur 2021;11:100235 doi 10.1016/j.lanepe.2021.100235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Benard VB, Watson M, Saraiya M, Harewood R, Townsend JS, Stroup AM, et al. Cervical cancer survival in the United States by race and stage (2001–2009): Findings from the CONCORD-2 study. Cancer 2017;123 Suppl 24(Suppl 24):5119–37 doi 10.1002/cncr.30906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Eggleston KS, Coker AL, Williams M, Tortolero-Luna G, Martin JB, Tortolero SR. Cervical cancer survival by socioeconomic status, race/ethnicity, and place of residence in Texas, 1995–2001. Journal of women’s health (2002) 2006;15(8):941–51 doi 10.1089/jwh.2006.15.941. [DOI] [PubMed] [Google Scholar]
- 51.Coker AL, Desimone CP, Eggleston KS, White AL, Williams M. Ethnic disparities in cervical cancer survival among Texas women. Journal of women’s health (2002) 2009;18(10):1577–83 doi 10.1089/jwh.2008.1342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Saraiya M, Unger ER, Thompson TD, Lynch CF, Hernandez BY, Lyu CW, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. Journal of the National Cancer Institute 2015;107(6):djv086 doi 10.1093/jnci/djv086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gravitt PE, Winer RL. Natural History of HPV Infection across the Lifespan: Role of Viral Latency. Viruses 2017;9(10) doi 10.3390/v9100267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Buja A, Lago L, Lago S, Vinelli A, Zanardo C, Baldo V. Marital status and stage of cancer at diagnosis: A systematic review. European journal of cancer care 2018;27(1) doi 10.1111/ecc.12755. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data analyzed in this study are available from the California Cancer Registry. Access is granted through an application process by the management or data custodians (https://www.ccrcal.org/retrieve-data/).