
Central illustration. Risk assessment strategy of non-ischaemic lesions according to physiologic lesion severity and quantitative and qualitative plaque characteristics.
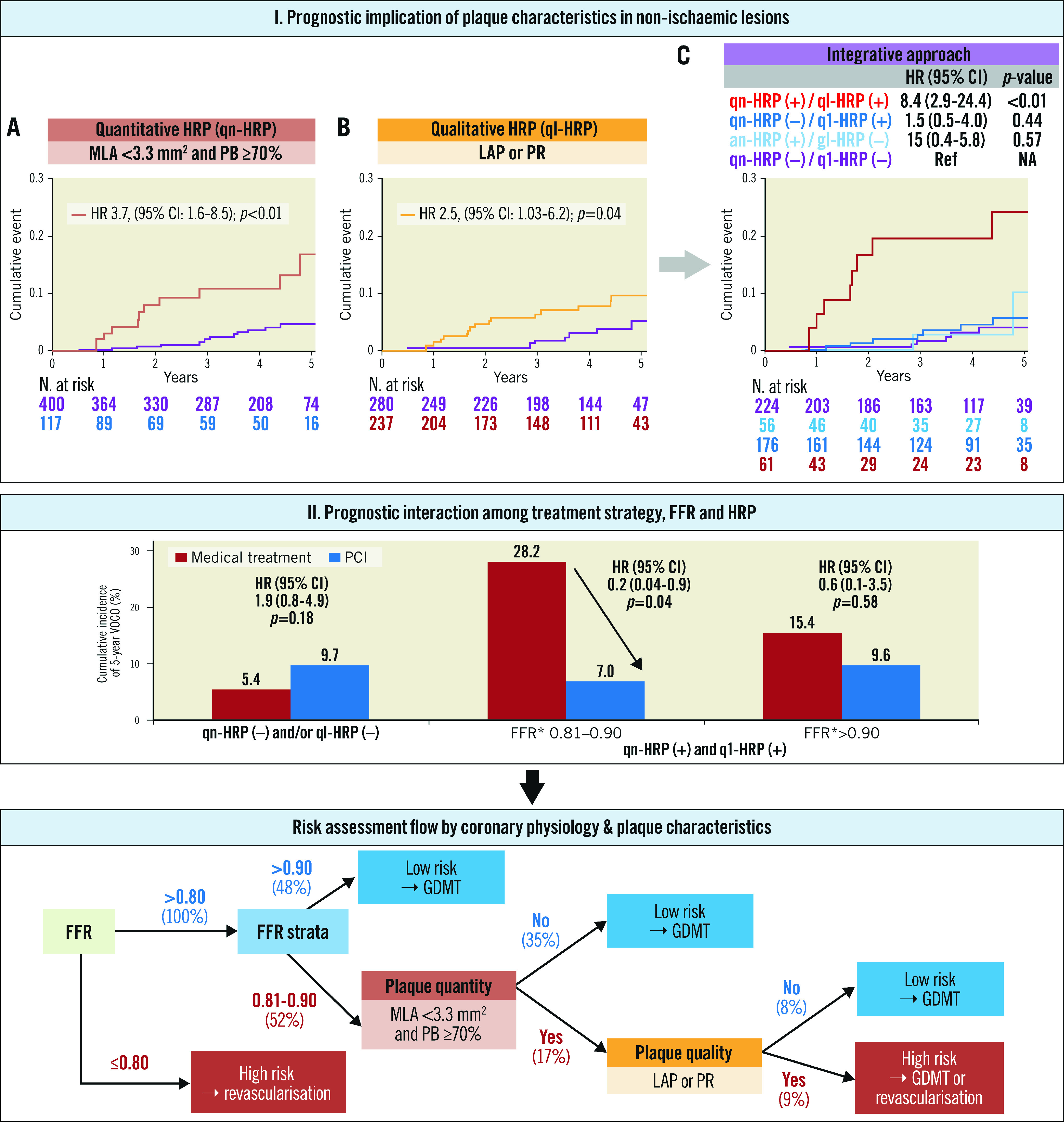
The presence of qn-HRP or ql-HRP was associated with an increased risk of VOCO, but only the lesions with both qn-HRP and ql-HRP showed a higher risk than the lesions without them. When lesions were stratified by FFR strata, qn-HRP, and ql-HRP, the PCI group showed a lower risk for VOCO than the medical treatment group in lesions with both qn-HRP and ql-HRP and FFR of 0.81–0.90. Based on these observations, a risk assessment strategy for non-ischaemic lesions was proposed. qn-HRP: MLA <3.3 mm2 and plaque burden ≥70.0%, ql-HRP: low-attenuation plaque or positive remodelling. *In the PCI group, revascularisation was performed in low pre-PCI FFR (≤0.80) lesions, and post-PCI FFR was designated as the FFR value of the corresponding vessel. CI: confidence interval; FFR: fractional flow reserve; GDMT: guideline-directed medical treatment; HR: hazard ratio; HRP: high-risk plaque; LAP: low-attenuation plaque; MLA: minimum lumen area; PB: plaque burden; PCI: percutaneous coronary intervention; PR: positive remodelling; ql-HRP: qualitative HRP; qn-HRP: quantitative HRP; VOCO: vessel-oriented composite outcomes