
FIGURE 1.
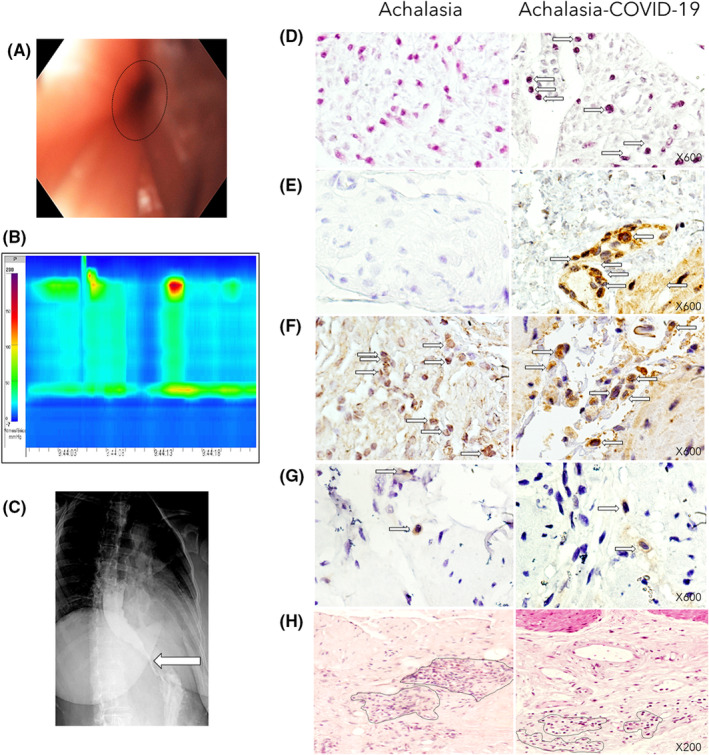
(A) Upper endoscopy shows dilated esophagus (patient that developed achalasia post‐COVID‐19). (B) High‐resolution manometry shows abnormal relaxation of the lower esophageal sphincter (LES) and aperistalsis with panesophageal pressurization in 40% of swallows, corresponding with type II achalasia. (C) Barium esophagram that shows dilation and bird beak sign (arrow). (D) The photographs depict the in situ PCR for SARS‐CoV2 (arrows indicate positive cells in dark blue) of the LES muscle of type II achalasia patient (left) and type II achalasia post‐COVID‐19 patient (right). Magnification x600. (E) The left and right panels show immunohistochemistry for SARS‐CoV2 (arrows indicate positive spike expression in brown). Magnification x600. (F) The left and right panels show immunohistochemistry for ACE2 expression (Arrows depict positive cells in brown). Magnification x600. (G) The left and right panels show immunohistochemistry for HSV‐1 expression (Arrows depict positive cells in brown). Magnification x600. (H) Tissue architecture of the LES muscle of type II achalasia patient (left) and type II achalasia post‐COVID‐19 (right). Dot circles depict inflammatory infiltrates. Magnification x200.