
Fig 1.
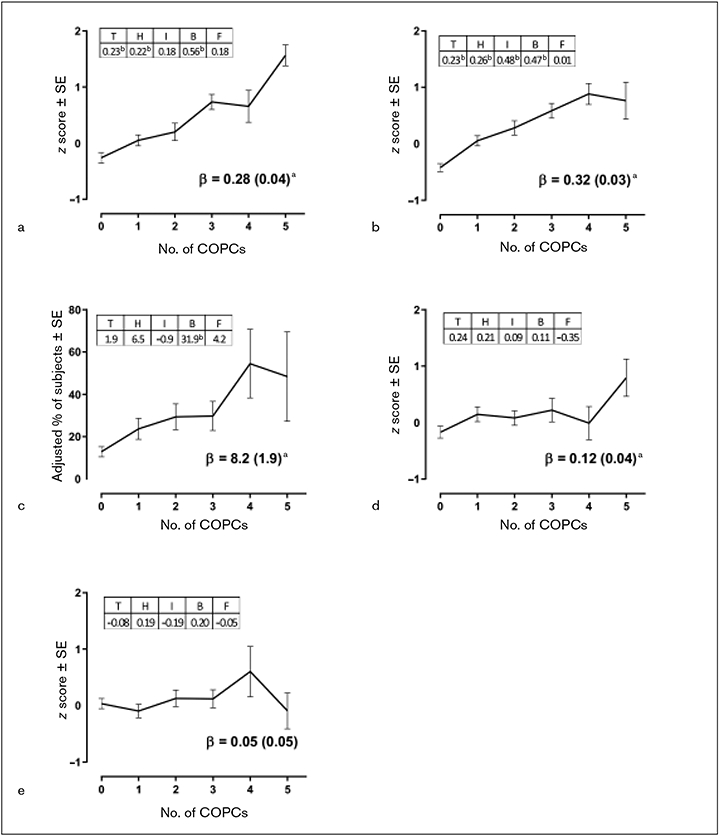
Relationships between number of COPCs and health measures in OPPERA-2 (n = 655 participants). (a) PROMIS Fatigue Score. (b) PSQI Sleep Disturbance. (c) Obstructive Sleep Apnea. (d) Number of atopic disorders. (e) Body mass index. Each health measure was the dependent variable in separate linear regression models that used weighted estimates from generalized estimating equations with robust error variance calculation and with adjustment for study site, age, gender, and race. Each plot summarizes the results from the three linear regression models: (1) Plotted values are adjusted means of the z-transformed health measure ± standard error (SE) from models in which the number of COPCs was the categorical predictor variable. (2) Beta (β) estimate (SE) represents amount of change in the dependent variable associated with a unit increase in number of COPCs, modeled as a continuous variable. aP < .05 for the null hypothesis that β = 0. (3) All five COPCs were modeled as binary predictor variables in a multivariable linear regression model that adjusted for covariates to show independent contributions of the COPCs to each clinical measure. The tabulated numbers, denoted as T = temporomandibular disorder, H = headache, I = irritable bowel syndrome, B = low back pain, and F = fibromyalgia, are parameter estimates for COPCs. bP < .05 for the null hypothesis that the parameter estimate for the dummy variable = 0.