
Figure 3.
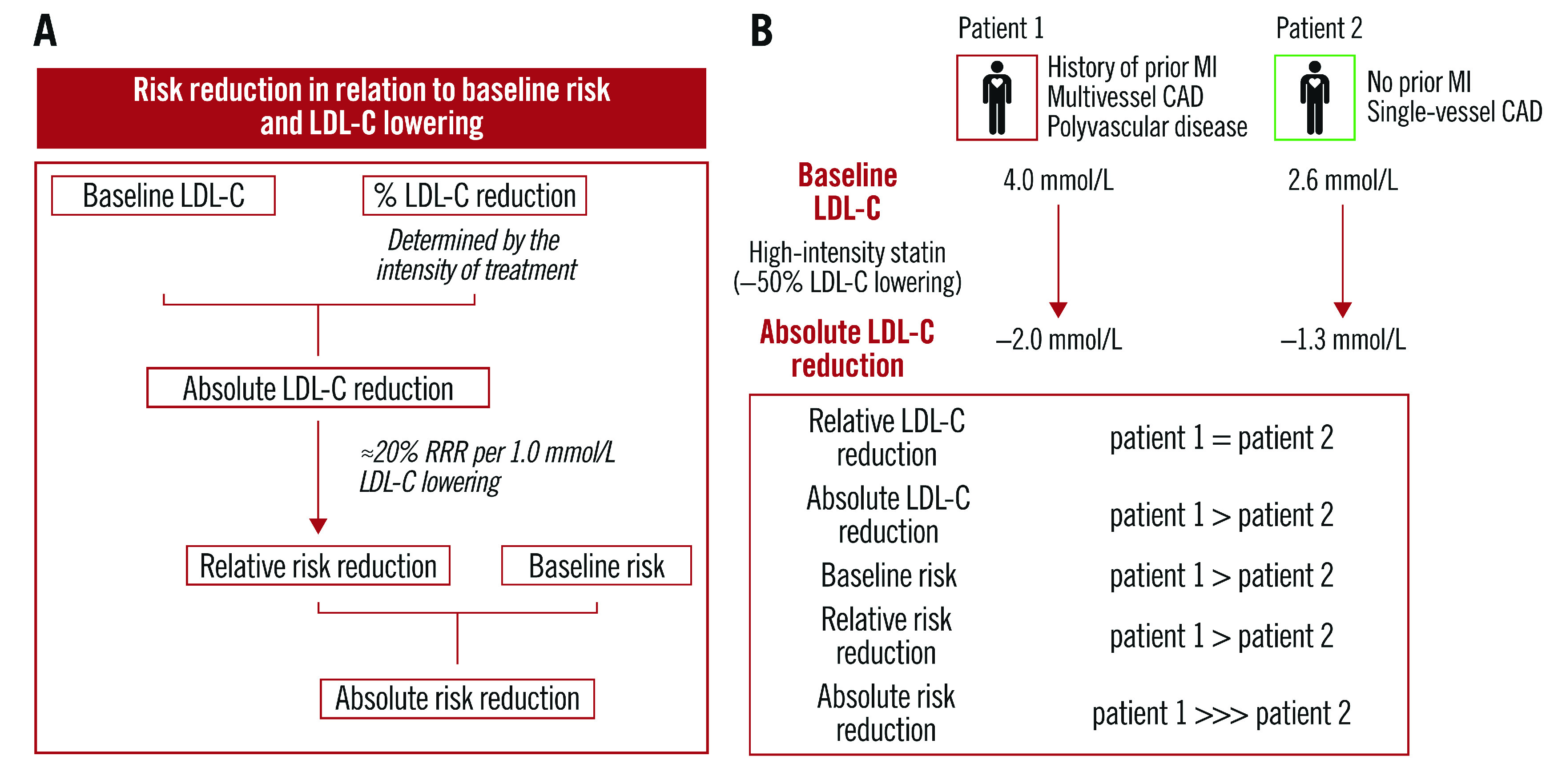
Expected clinical benefit of LDL-C lowering. A) Baseline LDL-C levels and the anticipated relative LDL-C reduction with a lipid-lowering medication both determine the expected magnitude of absolute achieved LDL-C lowering. Each 1.0 mmol/L absolute reduction in LDL-C levels is associated with an approximately 20% relative reduction in the risk of cardiovascular events, such that larger absolute LDL-C reductions result in larger proportional reductions in risk. The absolute risk reduction is driven by both the relative risk reduction and absolute baseline risk. B) Case example of two patients presenting with ACS but with different baseline (untreated) LDL-C levels and risk profiles. In both patients, guideline-recommended treatment with a high-intensity statin is expected to bring a similar (approximately 45-50%) reduction in LDL-C levels; a larger absolute LDL-C reduction, and thereby a 1.5-fold larger proportional reduction in CV risk (about 20% per 1.0 mmol/L LDL-C lowering), is estimated for patient 1 due to the higher baseline LDL-C levels. Coupled with a higher baseline risk in patient 1 (due to a history of previous MI, multivessel CAD and polyvascular disease), and although a significant risk reduction is estimated for both patients, the absolute risk reduction is expected to be substantially higher for patient 1.