

Abstract
Allergic rhinitis is a common and chronic immunoglobulin E-mediated inflammation of nasal mucosa induced after allergen exposure. Allergic rhinitis is a global health problem that causes major illness and affects patient’s social life, sleep, school and work performance. Various studies have implicated the association between low serum vitamin D levels and allergic diseases. Active form of Vitamin D3 has been shown to have immunoregulatory effect on both innate and adaptive immunity, which can significantly affect the outcome of allergic responses in allergic rhinitis. The study aims to evaluate effectiveness of Oral Vitamin D3 supplementation as an adjunct to standard therapy, in the management of allergic rhinitis. The present study is a prospective study in which 80 subjects were recruited and were randomly divided into two groups. The study group received oral vitamin D3 (60,000 IU) along with intranasal steroid spray while control group received only intranasal steroid spray for 4 weeks. The response in both the groups was compared by evaluating total nasal symptom score (TNSS). Subjects of allergic rhinitis showed deficiency in vitamin D indicated by mean serum vitamin D levels of 15 ± 2.42 ng/ml in the study group and 14.72 ± 2.64 ng/ml in the control group. The pre treatment mean TNSS score was 10.45 ± 3.1 in the study group and 11.43 ± 2.35 in the control group. The post treatment mean TNSS score was 2.1 ± 0.21 in the study group and 3.85 ± 0.76 in the control group. A significant reduction in symptoms score was observed after 4 weeks of oral vitamin D3 supplementation. The difference between two groups was found to be statistically significant (p value < 0.05).
Keywords: Vitamin D3, Supplementation, TNSS, Allergic rhinitis
Introduction
Allergic rhinitis is one of the inflammatory diseases of the nasal mucosa, caused by immunoglobulin E(IgE) after allergen exposure which affects 10–20% of total population [1]. The main clinical symptoms are sneezing, runny, stuffy and itchy nose, which are accompanied by ocular symptoms such as watery, red and itching eyes. Severe allergic rhinitis have been associated with negative impact on sleep, mood, work/school performance and health related quality of life. Prevalence of allergic rhinitis has been increased over the years and various studies have pointed out the association between Vitamin D3 deficiency and allergic rhinitis [2–4]. Vitamin D3 deficiency has been widely discussed as one of the world health problems which can lead to acute and chronic illness. Studies have proven that food allergies and anaphylaxis occurs at much higher rates in areas with less sun exposure. In addition asthma, eczema and atopy have been associated with low vitamin D3 levels, particularly for people who have mutations in their vitamin D receptor genes [5, 6].
Futhermore, studies have shown that Vitamin D3 acts as a potent immunomodulator by regulating the body’s immune system cells which work on the pathophysiology of allergic rhinitis. Vitamin D3 affects T cells, B cells, monocytes and macrophages and regulates the activity of dendritic cells which are the key immune system cells [7, 8]. Although studies have investigated the role of Vitamin D in the treatment of allergic rhinitis, the results are still controversial.
The present study is conducted to determine the role of oral vitamin D3 supplementation in improving the clinical symptoms in allergic rhinitis patients.
Methods
The present study is conducted in out patient department of ENT from December 2018 to November 2020. The study was approved by Institutional ethics committee. A total of 100 patients of Allergic rhinitis were selected and diagnosed clinically. Diagnosis of AR was made according to AR and its impact on Asthma classification [9]. The cardinal symptoms according to ARIA guidelines are paraoxysmal sneezing, itching in the nose, itching of eyes, palate or pharynx, watery nasal discharge, nasal obstruction and history of urticaria while the clinical signs include pale boggy nasal mucosa, hypertrophied turbinates, thin watery or mucoid discharge and transverse nasal crease.
Inclusion Criteria
Patients aged between 15 and 60 years, either sex, clinically diagnosed as AR seasonal or perennial.
Exclusion Criteria
Non-allergic rhinitis.
Associated nasal co-morbidities like Nasal polyposis, sinusitis, DNS and autoimmune diseases.
Associated co-morbidities like kidney disease, rickets and osteomalacia.
Taking other medications like immunomodulatory, H/o Immunotherapy, H/o Vitamin D consumption in past.
All the patients were thoroughly interviewed and Complete ENT examination was done.
Patients were randomly assigned to the study and control group. The study group received standard pharmacotherapy (intranasal steroid spray) along with Oral vitamin D(60,000 IU) for 4 weeks. Control group received only standard therapy for allergic rhinitis. Serum Vitamin D3 levels were recorded pre and post treatment. Total Nasal symptoms score (TNSS) were evaluated pre and post treatment. Total nasal symptoms score was assessed based on the severity of the symptoms as depicted in Table 1.
Table 1.
Total nasal symptoms and scoring system
| Symptoms | Score |
|---|---|
| Rhinorrhoea | 0–3 |
| Obstruction | 0–3 |
| Sneezing | 0–3 |
| Itching | 0–3 |
| Anosmia | 0–3 |
| TNSS | Out of 15 |
0, Absent; 1, Mild; 2, Moderate; 3, Severe; TNSS, total nasal symptoms score
The severity of each symptom was based on following scores:
0 = No symptoms
1 = Mild symptoms
2 = Moderate disturbing symptoms
3 = Severe symptoms that interferes with daily activities, sleep, work performance.
Statistical Analysis
Data was entered into SPSS Version 17.0. Data was expressed as mean with standard deviation. The mean values in study and control groups were compared by using student’s unpaired t-test. A p value of < 0.05 was considered as statistically significant.
Results
Out of 100 subjects with allergic rhinitis,80 subjects were included in the study who had Vitamin D deficiency (Serum vitamin D deficiency < 20 ng/ml) where as 20 subjects with normal vitamin D levels were excluded from the study. Among 80 AR subjects, there were 34 male subjects (42.5%) and 46 female subjects (57.5%). Male to female ratio was 1:1.35.
The majority of subjects were in the age group of 15–30 years. The mean age of presentation of subjects was 26.45 years. The mean value of serum vitamin D level at the start of the study were 15 ± 2.42 ng/ml and 14.72 ± 2.64 ng/ml in study group and control group respectively, with no significant differences between the two groups.
All baseline characteristic is depicted in Table 2.
Table 2.
Baseline characteristics of subjects
| Characteristics | Study group n = 40 |
Control group n = 40 |
p value |
|---|---|---|---|
| Age(years) | 27.76 (± 7.02) | 26.42 (± 8.85) | 0.26 |
| Male | 18 (45%) | 16 (40%) | 0.33 |
| Female | 22 (55%) | 24 (60%) | |
| Mean vitamin D3 levels (ng/ml) | 15 ± 2.42 | 14.72 ± 2.64 | 0.23 |
Maximum subjects presented with symptoms of Rhinorrhoea followed by obstruction, sneezing, itching and anosmia as depicted in Table 3.
Table 3.
Symptoms of allergic rhinitis among subjects
| Symptoms | No. of subjects (%) |
|---|---|
| Rhinorrhoea | 58 (72.5%) |
| Obstruction | 48 (60%) |
| Sneezing | 40 (50%) |
| Itching | 20 (25%) |
| Anosmia | 13 (16.25%) |
The subjects were evaluated for TNSS score according to symptoms at the time of presentation (pre-treatment score) and after 4th week (post-treatment score). Out of 80 subjects, 16 (20%) had severe signs and symptoms of AR (TNSS > 10), 34 (42.5%) were having moderate signs and symptoms (TNSS 7–10) and 30 (37.5%) had mild signs and symptoms of AR with TNSS < 7. Table 4 shows TNSS grading in both study and control group.
Table 4.
Distribution of subjects according to grading of TNSS score
| Grading | TNSS score | |
|---|---|---|
| Study group | Control group | |
| Mild < 7 | 16 (40%) | 14 (35%) |
| Moderate 7–10 | 15 (37.5%) | 19 (47.5%) |
| Severe > 10 | 9 (22.5%) | 7 (17.5%) |
| Total | 40 | 40 |
The mean pre-treatment TNSS score in study group (pharmacotherapy with Oral Vitamin D3) was 10.45 ± 3.10 while post- treatment TNSS score was 2.1 ± 0.21. The mean pre-treatment TNSS score in control group (pharmacotherapy without Oral Vitamin D3) was 11.43 ± 2.35 while post treatment TNSS score was 3.85 ± 0.76, depicted in Table 5 and Fig. 1.
Table 5.
Total nasal symptoms score (TNSS) pre and post treatment
| Mean TNSS (at 4th week) | Significance | ||
|---|---|---|---|
| Study group | Control group | ||
| Pre-treatment | 10.45 ± 3.1 | 11.43 ± 2.35 | p value < 0.05 |
| Post-treatment | 2.1 ± 0.21 | 3.85 ± 0.76 | |
Fig. 1.
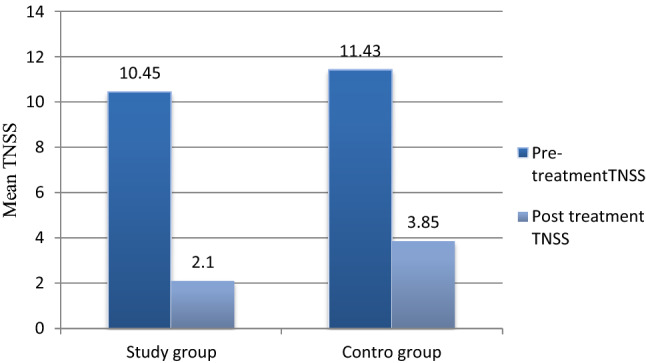
Total nasal symptoms score (TNSS) pre-treatment and post treatment at 4 weeks
The student’s unpaired ‘t’ test was applied to compare the TNSS score between two groups which showed no significant difference in pre-treatment total nasal symptom scores but significant difference in post treatment total nasal symptoms score after 4 weeks (p value < 0.05).
Discussion
The present study was conducted with a primary objective to see for any symptoms improvement in patients of AR with Vitamin D3 supplementation using Total nasal score system. Among 80 AR subjects included in the study, there were 34 males subjects (42.5%) and 46 female subjects (57.5%). Male to female ratio was 1:1.35. The mean age of presentation of AR subjects was 26.45 years.
Out of 100 subjects with AR, 80 subjects (80%) were included in the study as they had deficient levels of Serum Vitamin D3 levels suggesting higher incidence of Vitamin D3 deficiency in these subjects. The mean Vitamin D3 levels were 15 and 14.72 in study and control group respectively with no significant differences between two groups (p value = 0.23). Similarly Arshi et al. [10] in their study assessed Vitamin D levels of 50 patients with AR and reported a significantly higher prevalence of severe Vitamin D deficiency in patients with AR. After 4 weeks of supplementation of oral vitamin D3, the mean serum vitamin D3 levels in the study group showed a significant difference compared with vitamin D3 levels at pre treatment which signifies the role of evaluating Vitamin D3 levels in allergic rhinitis before starting treatment.
Total nasal symptom score (TNSS) was assessed pre and post-treatment. A significant decrease in TNSS was found in the study group that received oral vitamin D3 supplementation in addition to the steroid spray as compared to the control group which received only steroid spray. This is in accordance with the study done by Gupta et al. [11] in 2016, where 27 patients of allergic rhinitis with mean age of 26.47 ± 9.25 years were enrolled. Their treatment regimen included oral antihistaminic which was supplemented by oral vitamin D3 in 14 patients and in rest 13 patients no vitamin D supplementation was added. The study revealed overall symptomatic improvement in nasal symptoms score (NSS) in patients receiving vitamin D along with antiallergic medication. Another study by Modh et al. [12] conducted on 21 allergic rhinitis with vitamin D deficiency also showed significant symptomatic improvement after supplementation of Oral Vitamin D3 Similarly in 2019, Agarwal et al. [13] evaluated 80 AR subjects using TNSS and concluded that Vitamin D3 supplementation lowers TNSS score with symptomatic relief.
Symptomatic improvement after supplementation of Vitamin D3 in patients of Allergic rhinitis could be related to its immunomodulatory effects, as it acts on both innate and adaptive immune system. Vitamin D regulates activities of T cells, B cells, dendritic cells, monocytes and macrophages. It inhibits the proliferation of T cells, induces a shift from TH1 to TH2, and provokes the synthesis of T-regulatory cells that are important immune reactions in the course of AR. Vitamin D activates apoptosis of activated B cells and inhibits plasma differentiation and immunoglobin secretion, including IgE [14–16]. Hence it suggests that Vitamin D can act as a disease modulator by improving the quality of life in AR patients.
Conclusion
The study concludes that oral Vitamin D3 supplementation along with standard therapy can provide clinically significant improvement in symptoms in patients of allergic rhinitis with Vitamin D3 deficiency.
Funding
No funding sources.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Taken from Institutional Ethics Committee.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Small P, Kim H. Allergic rhinitis. Allergy Asthma Clin Immunol. 2011;7 Suppl(Suppl 1):S3. doi: 10.1186/1710-1492-7-S1-S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bunyavanich S, et al. Prenatal, perinatal, and childhood vitamin D exposure and their association with childhood allergic rhinitis and allergic sensitization. J Allergy Clin Immunol. 2016;137(4):1063–1070.e2. doi: 10.1016/j.jaci.2015.11.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dogru M, Suleyman A. Serum 25-hydroxyvitamin D3 levels in children with allergic or nonallergic rhinitis. Int J Pediatr Otorhinolaryngol. 2016;80:39–42. doi: 10.1016/j.ijporl.2015.11.013. [DOI] [PubMed] [Google Scholar]
- 4.Bener A, Ehlayel MS, Bener HZ, Hamid Q. The impact of Vitamin D deficiency on asthma, allergic rhinitis and wheezing in children: An emerging public health problem. J Family Community Med. 2014;21(3):154–161. doi: 10.4103/2230-8229.142967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bauchau V, Durham SR. Prevalence and rate of diagnosis of allergic rhinitis in Europe. Eur Respir J. 2004;24(5):758–764. doi: 10.1183/09031936.04.00013904. [DOI] [PubMed] [Google Scholar]
- 6.Mullins RJ, Camargo CA. Latitude, sunlight, vitamin D, and childhood food allergy/anaphylaxis. Curr Allergy Asthma Rep. 2012;12(1):64–71. doi: 10.1007/s11882-011-0230-7. [DOI] [PubMed] [Google Scholar]
- 7.Searing DA, Leung DY. Vitamin D in atopic dermatitis, asthma and allergic diseases. Immunol Allergy Clin North Am. 2010;30(3):397–409. doi: 10.1016/j.iac.2010.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tian HQ, Cheng L. The role of vitamin D in allergic rhinitis. Asia Pac Allergy. 2017;7(2):65–73. doi: 10.5415/apallergy.2017.7.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brożek JL, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950–958. doi: 10.1016/j.jaci.2017.03.050. [DOI] [PubMed] [Google Scholar]
- 10.Arshi S, Ghalehbaghi B, Kamrava SK, Aminlou M. Vitamin D serum levels in allergic rhinitis: any difference from normal population? Asia Pac Allergy. 2012;2(1):45–48. doi: 10.5415/apallergy.2012.2.1.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gupta PK, Raut P, Singh SP. Vitamin D and modulation of allergic rhinitis. Int J Sci Res. 2017;6(2):330–333. [Google Scholar]
- 12.Modh D, Katarkar A, Thakkar B, Jain A, Shah P, Joshi K. Role of vitamin D supplementation in allergic rhinitis. Indian J Allergy Asthma Immunol. 2014;28:35–39. doi: 10.4103/0972-6691.134223. [DOI] [Google Scholar]
- 13.Agarwal S, Singh SN, Kumar R, Sehra R. Vitamin D: a modulator of allergic rhinitis. Indian J Otolaryngol Head Neck Surg. 2019;71(Suppl 3):2225–2230. doi: 10.1007/s12070-019-01697-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bartels LE, Bendix M, Hvas CL, Jørgensen SP, Agnholt J, Agger R, Dahlerup JF. Oral vitamin D3 supplementation reduces monocyte-derived dendritic cell maturation and cytokine production in Crohn's disease patients. Inflammopharmacology. 2014;22(2):95–103. doi: 10.1007/s10787-013-0197-1. [DOI] [PubMed] [Google Scholar]
- 15.Boonstra A, Barrat FJ, Crain C, Heath VL, Savelkoul HF, O'Garra A. 1alpha,25-Dihydroxyvitamin d3 has a direct effect on naive CD4(+) T cells to enhance the development of Th2 cells. J Immunol. 2001;167(9):4974–4980. doi: 10.4049/jimmunol.167.9.4974. [DOI] [PubMed] [Google Scholar]
- 16.Robinson DS. Regulatory T cells and asthma. Clin Exp Allergy. 2009;39(9):1314–1323. doi: 10.1111/j.1365-2222.2009.03301.x. [DOI] [PubMed] [Google Scholar]