
Fig. 1.
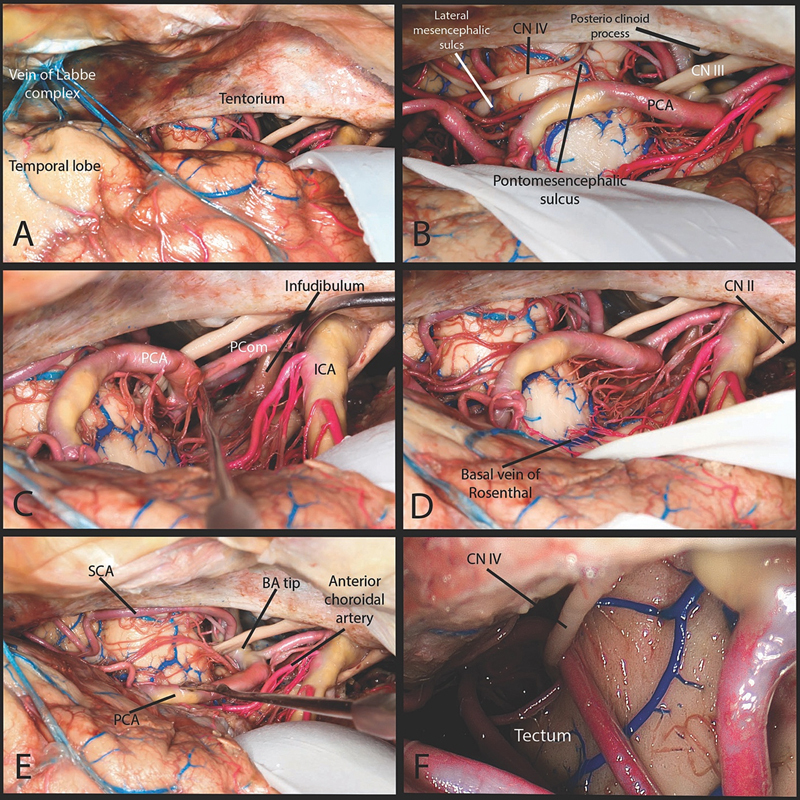
Subtemporal approach. ( A ) A temporal craniotomy was performed. Wide opening of the arachnoid spaces around tentorial incisura exposes underlying structures. The arachnoid dissection around the vein of Labbé complex is performed to maximize safe retraction. ( B ) The anterior and the anterior part of the middle incisural space is exposed. The anterior part of tentorial free edge starting at the anterior and posterior clinoid process was visualized. The free edge of the tentorium was easily followed up to the lateral mesencephalic sulcus. The pontomesencephalic sulcus was identified at the level of the tentorium. ( C ) Within the anterior incisural space the infundibulum from the hypothalamus to the pituitary was visualized. The oculomotor nerve was easily seen within the arachnoid spaces between the posterior cerebral artery (PCA) and superior cerebellar artery (SCA) and where it enters the cavernous sinus within the oculomotor triangle. ( D ) Extensive retraction of the medial temporal lobe was required to visualize the basal vein of Rosenthal. ( E ) The basilar tip, P1, posterior communicating, P2, SCA were exposed in all specimens. The origin and most of the cisternal segment of the anterior choroidal artery could also be exposed through the subtemporal approach. In all specimens the lateral mesencephalic vein was visualized. ( F ) From a subtemporal view the origin of trochlear nerve cannot be seen even with the use of endoscope. BA, basilar artery; CN, cranial nerve; ICA, internal carotid artery; PCA, posterior cerebral artery; Pcom, posterior communicating artery; SCA, superior cerebellar artery.