
Figure 1: Different Modalities of Invasive Brain Stimulation and Distribution of Patients by Seizure Onset across Neurostimulation Modalities –
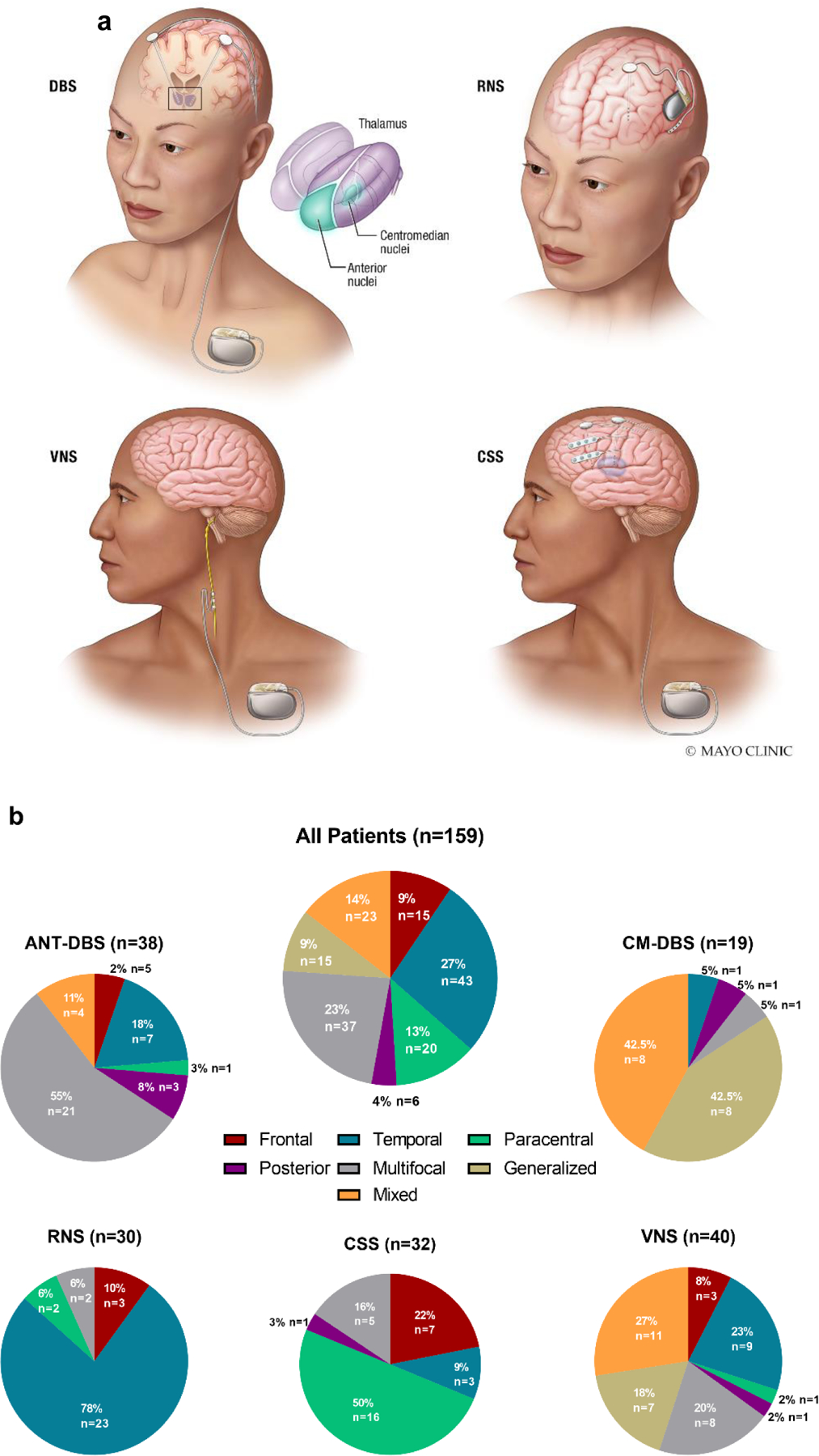
(a) Visual representation of the invasive neuromodulation strategies included in the present study. The top left panel represents deep brain stimulation (DBS) of either the anterior thalamic nuclei, centromedian nuclei or both. The top right panel represents responsive neurostimulation (RNS) with a depth lead and a subcortical lead (8 contacts total). The bottom left panel represents vagus nerve stimulation (VNS). The bottom right panel represents chronic subthreshold stimulation (CSS) with two depth electrodes and two subdural strips (16 contacts total). DBS, VNS and CSS are connected to an implantable pulse generator (IPG) placed in the chest while RNS has cranial-mounted IPG. (b) Paracentral epilepsy reflects primary sensory and/or primary motor seizure onset. Posterior epilepsy reflects patients with parietal/occipital onset. Mixed epilepsy signifies generalized epilepsy in combination with focal/multifocal epilepsy.
ANT-DBS, anterior thalamic nuclei deep brain stimulation; CM-DBS, centromedian thalamic nuclei deep brain stimulation; CSS, chronic subthreshold stimulation; RNS, responsive neurostimulation; VNS, vagus nerve stimulation.