
Fig. 7. Effects of harmine–GLP-1 on β cells from individuals with T2D.
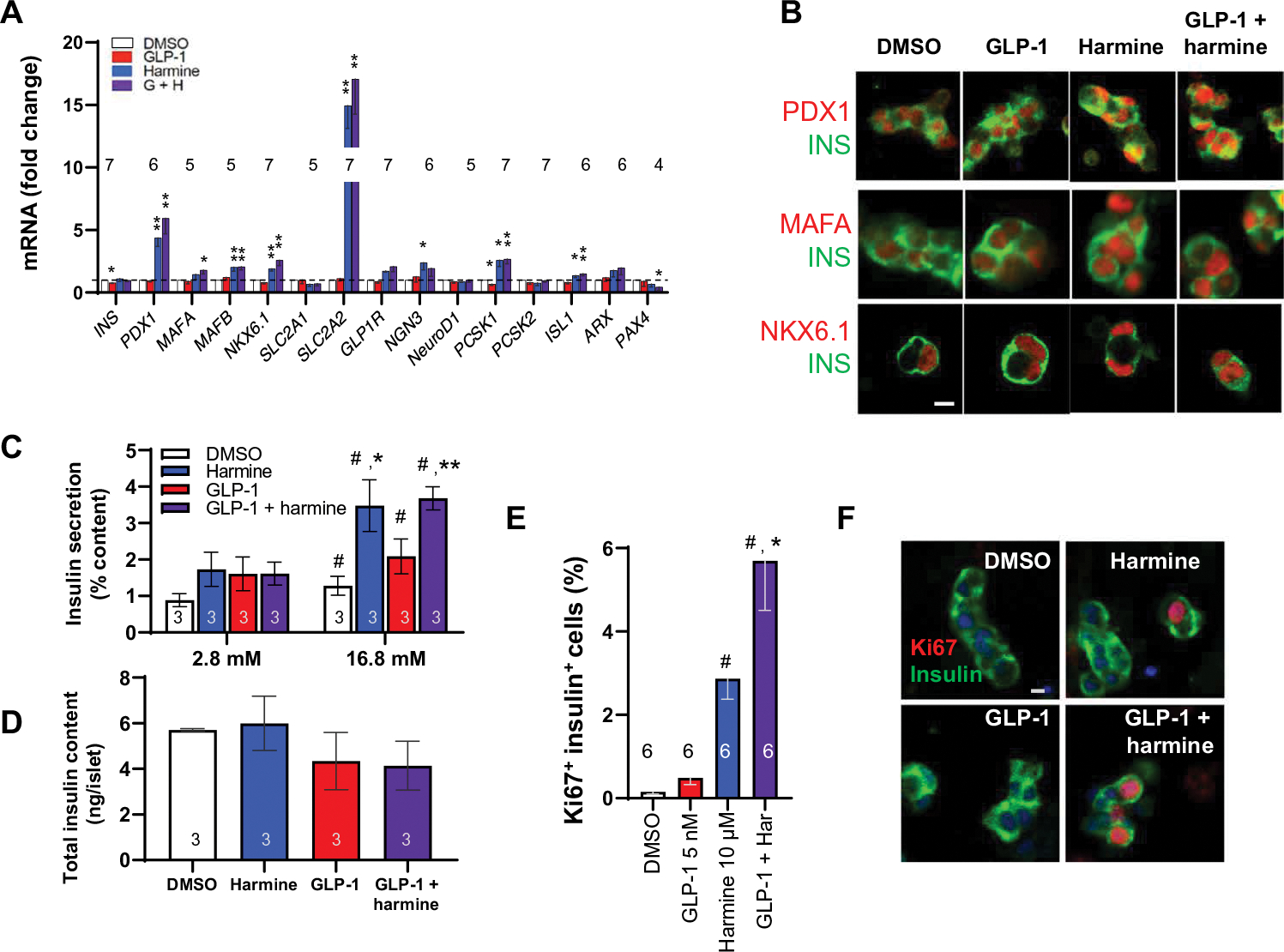
(A) The effects of harmine with or without GLP-1 on β cell differentiation markers. *P < 0.05 and **P < 0.01 versus control by paired two-tailed t test. (B) Confocal imaging examples of PDX1, MAFA, and NKX6.1 immunolabeling of dispersed human T2D islets after the treatments shown. (C) Insulin secretion in response to low (2.8 mM) and high (16.8 mM) glucose in three different T2D islet preparations pretreated with vehicle, GLP-1, harmine, or their combination for 72 hours. (D) Residual insulin content in the islets from (C). The average insulin concentration in the 2.8 mM glucose control (DMSO) wells was 18.1 ± 3.2 pmol per islet, and that at 16.7 mM glucose was 32.2 ± 4.6 pmol per islet. (E) Human T2D β cell proliferation in response to vehicle, GLP-1, harmine, or the combination. (F) Examples of insulin and Ki67 immunolabeling in β cells derived from donors with T2D. Values are means ± SEM. Numbers within or above bars indicate the sample size of human islet donors. (C to E) #P < 0.05 versus control; *P < 0.05 and **P < 0.01 versus harmine alone, both by one-way ANOVA. Scale bars, 10 μm (B and F).